
Dr. Sheera K R, S19348, Dr. Unnikrishnan Nair R, Dr. Manoj S
BACKGROUND
Retinopathy of prematurity (ROP) is a retinal vascular disorder in premature infants and theleading cause of childhood blindness. Because effective treatment exists[1,2], focus has shifted towards ensuring that all babies at risk for development of ROP are screened. The gold standard for diagnosis of ROP is binocular indirect ophthalmoscopy ‘‘by an ophthalmologist”. But two recent events have precipitated increased utilisation of those who provide ROP screening—increase in the eligible screening population and a decrease in the willing screener population. Digital imaging and telemedicine have the capability to alleviate these screening problems by takingstandardised wide-angle digital retinal images and allowing remote interpretation of these photographs by an ophthalmologist experienced in ROP. This technology may improve the quality, delivery, accessibility, and cost of ROP care[3,4].Over the last decade, the sensitivity and specificity of this technology have been continually improving, with recent studies showing comparable outcomes between digital screening and screening with indirect ophthalmoscopy[5,6].
AIMS AND OBJECTIVES
To assess the initial experience of RETCAM based digital telescreening for retinopathy of prematurity (ROP) in neonatology centres through the mobile CRADLE ROP screening initiative.
MATERIALS AND METHODS
Twelve Neonatal Intensive Care Units (NICUs) in the state were enrolled in the first 8 month period and infants meeting the ROP screening criteria by National Neonatology Forum (NNF)of India were screenedbetween October 2016 and May 2017.NNF screening criteria was babies born<34 weeks of gestation and/or <1750 grams birth weight; as well as in babies 34-36 weeks gestation or 1750-2000 grams birth weight if they have risk factors for ROP or if the neonatologist feels there is risk for ROP.The risk factors considered are mechanical ventilation, prolonged oxygen therapy, hemodynamic instability,neonatal jaundice,unstable clinical course, hypoxemia, hypotension, anaemia, blood transfusion, late –onset sepsis, delay in return to birth weight beyond 14 days, hypercarbia and hypotension.All the screening examinations were done by using RETCAM SHUTTLE(fig:1)in the NICU step down room in the presence of a paediatrician or neonatologist.
Fig:1 RETCAM shuttleTM. Natus Medical Inc.

Pupillary dilation was achieved with 2.5% phenylephrine and 0.5% cyclopentolate30–60 min prior to examination. Aspiration precautions consisted of discontinuing feedings 1 h pre- examination. All examinations were performed with close cardiac and respiratory monitoring, and if the heart rate or oxygen saturation was unacceptably low, the examination was halted until the infant was deemed stable to continue.
A topical anaesthetic, 0.5% proparacaine, was instilled in each eye before examination. A sterile lid speculum was used to open the eye and provide adequate exposure for photography. Lubricating jelly or hydroxypropyl methylcellulose (2.5%) was used to couple the digital camera lens to the infant’s cornea. Digital images were taken by a trained person and stored on the RETCAM shuttle computer hard drive. After screening Moxifloxacin 0.5% was instilled in both eyes.
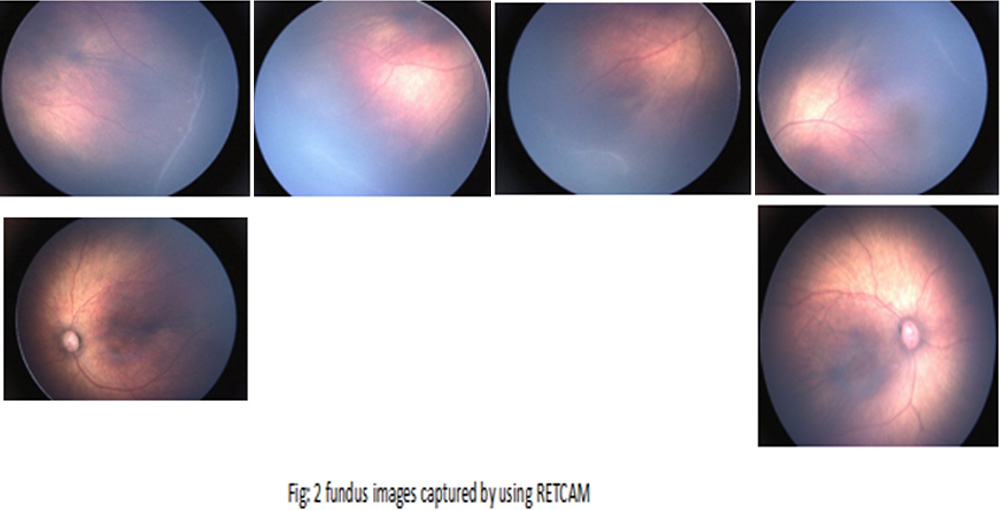
Details regarding the baby, like gestational age at birth, birth weight, born out of single or multiple pregnancy, risk factors present were collected from the NICU records. The goal of each imaging session was to obtain six clearly focused images in each eye (1) optic nerve centred, (2) macula centred (3) optic nerve superior, (4) optic nerve inferior, (5) optic nerve nasal and (6) optic nerve temporal(fig:2).Images were captured as necessary until they were seemed to be of adequate quality for examination. In cases of inadequate exposure, artefact, poor visualisation of the periphery or lack of a complete standardised image set, indirect ophthalmoscopic examination was done by an ophthalmologist.
Staging was done using the International classification of ROP. Stage 0 ROP referred to incomplete vascularisation, stage 1 – presence of demarcation line, stage 2 – ridge of elevated tissue, stage 3 was presence of extra retinal fibrovascular proliferation, stage 4 was partial retinal detachment, 4a –macula spared, and 4b- macula involving, stage 5 – total retinal detachment. Plus disease was diagnosed if posterior venous dilatation and arteriolar tortuosity were present in at least two retinal quadrants. Preplus disease referred to vascular abnormalities of the posterior pole that was more than normal but not mounting to plus disease.
After staging babies are divided in to with threshold ROP or pre threshold ROP. Threshold ROP was diagnosed in zone I stage 3 with plus disease or zone II stage 3 (5 contiguous or total 8 clock hours) with plus disease. Pre threshold ROP was diagnosed when zone I stage 1, 2 with plus disease, or stage 3 without plus disease, zone II stage 2 or 3(<5 contiguous or total <8 clock hours) with plus disease.
Statistical analysis was done by SPSS v20. Categorical data are displayed as proportions and continuous data as mean ± standard deviation. Pearson/Spearman’s chi-square test and Fisher exact test were used for comparison of discrete variables as appropriate. The t-test was used for comparison of continuous variables. All p-values were two – tailed and a value of less than 0.05 was considered statistically significant.
RESULTS
A total of 184 infants(368 eyes) fromtwelve neonatology centres were enrolled resulting in 359unique examinations done in various hospitals in Trivandrum, Kollam and Kottayam districts of Kerala. The average gestational age at birth was 32.8 (±3) weeks and average birth weight was 1841 (±663) grams. The average postnatal age atfirst screening for ROP was 4.6weeks.
Out of 184 babies, 46 (25%) were diagnosed with ROP. The mean postnatal age of diagnosis of ROP was 5.07 (±2.6) weeks. The corrected gestational age of these babies diagnosed with ROP was 34.37 (±5.9) weeks. This diagnosis was made at a median of 1st screen (range 1-3) of these babies by our team.
The diagnosis of ROP did not show any gender predilection. Oxygen supplementation, respiratory distress syndrome, the use of non-invasive ventilation, invasive ventilation were all more commonly associated with the diagnosis of ROP (table 1). While anemia was a more common diagnosis in babies with ROP, the need for blood transfusion in these babies was not significantly different. Babies born to parents who received treatment for infertility did not have a higher incidence of ROP compared to those borne of spontaneous conception (p=0.120). ROP was not more frequent in babies borne of multiple gestation as compared to singletons.
Table 1: Comparison of risk factor profile in babies with ROP and those without ROP
| ROP present (46) | No ROP (138) | Statistics | |
| Birth weight (g) | 1398 ±468 | 1989 ±654 | P<0.001 |
| Gestational age at birth (weeks) | 29.8 ±2.9 | 33.8 ±2.8 | P<0.001 |
| Male sex | 21 (45.7) | 79 (57.2) | P=0.177 |
| Multiple gestation | 19 (41.3) | 45 (32.6) | P=0.290 |
| Oxygen supplementation | 34 (73.9) | 67 (48.6) | P=0.003 |
| Non-invasive ventilation | 21 (48.8) | 22 (15.9) | P<0.001 |
| Invasive ventilation | 25 (54.3) | 33 (23.9) | P<0.001 |
| Respiratory distress syndrome | 33 (71.7) | 54 (39.1) | P<0.001 |
| Sepsis | 13 (28.3) | 23 (16.7) | P=0.091 |
| Anemia | 6 (13) | 4 (2.9) | P=0.017 |
| Blood transfusion | 6 (13) | 6 (4.3) | P=0.076 |
| Neonatal jaundice | 28 (60.9) | 68 (49.3) | P=0.233 |
| Seizures | 0 (0) | 7 (5.1) | P=0.195 |
| Infertility treatment | 12 (26.1) | 21 (15.2) | P=0.120 |
Multivariate analysis was done using a model created from the significant risk factors from univariate analysis. The results showed that gestational age a birth, birth weight, oxygen supplementation, invasive and non-invasive ventilation and a diagnosis of respiratory distress syndrome were all significantly associated with a diagnosis of ROP in these babies.
The mean postnatal age at the time of earliest diagnosis of ROP significantly differed with the gestational age at birth (table 2). Babies born before 28 weeks of gestation had ROP diagnosed at 6.83 ± 4.24 weeks of life. The lesser preterm babies had relatively earlier diagnosis of ROP with respect to postnatal age (p=0.044). While extremely low birth weight infants (<1000 g) were diagnosed with ROP between 6 – 7 weeks of life, the age at diagnosis of ROP was not significantly different in the babies who weighed more (p=0.197, table 2).
Table 2:Relationship of the age at ROP diagnosis with respect to gestational age and birth weight
| Parameter | Babies with ROP | Age at ROP diagnosis (weeks) | Statistics |
| Gestational age at birth | |||
| · <28 weeks | 12 | 6.83 ± 4.24 |
P=0.044 |
| · 28 – 32 weeks | 18 | 4.44 ± 1.58 | |
| · 32 – 36 weeks | 15 | 4.33 ± 0.98 | |
| · >36 weeks | 1 | 6.00 | |
| Birth weight | |||
| · Extremely low birth weight (<1000 g) | 9 | 6.67 ± 4.30 |
P =0.197 |
| · Very low birth weight
(1000 – 1500 g) |
23 | 4.87 ± 2.29 | |
| · Low birth weight
(1500 – 2500 g) |
12 | 4.25 ± 0.97 | |
| · Normal birth weight
(>2500 g) |
2 | 5.00 ± 1.41 |
13 babies (7%) required treatment for ROP. The mean birth weight of babies who required treatment for ROP was 1005 (±180) grams.
The mean birth weight was significantly lower in babies with ROP (1398 ±468 g) than those without ROP (1989 ±654 g) (p<0.001). Babies with ROP were born more prematurely (29.8 ±2.9 weeks) as compared to those without a diagnosis of ROP (33.8 ±2.8 weeks) (p<0.001). The corrected gestational age of the youngest baby diagnosed with ROP in our study was 30 weeks. This baby was born at 25 weeks of gestation. The prevalence of ROP in babies who weighed <1500g at birth was 57%. The incidence of ROP in extremely low birth weight infants (<1000 g) was 69.2%.
Out of 46 babies diagnosed to have ROP,fourbabies had threshold ROP and treated with laser. Pre threshold ROP was diagnosed when zone I stage 1, 2 with plus disease, or stage 3 without plus disease, zone II stage 2 or 3(<5 contiguous or total <8 clock hours) with plus disease. In our study cohort,eight babies were diagnosed to have pre threshold ROP with features of progression. Aggressive posterior ROP (APROP) was diagnosed in zone I rapidly evolving pre plus and plus disease progressing to stage 4 and 5 in 2-3 weeks without passing through characteristic stage 2 and 3. One baby with gestational age at birth 26 week was diagnosed as APROP underwent intravitreal anti-VEGF injection followed by laser treatment in both eyes.
All babies diagnosed with APROP, threshold ROP and pre threshold ROP with features of progression underwent Laser treatment.In our study cohort total 12 babies underwent laser treatment. None of the babies developed retinal detachment or any anatomical adverse outcome on follow up.
One baby born at28 weeks of gestation evaluated at 37 weeks of corrected gestational ageand diagnosed to have stage 4a disease was referred for surgical management.
7 babies (4%) were lost to follow up either because of migration to different place or referred to another centre for further systemic management. Parents of five babies were not willing to come for follow up.
DISCUSSION
Improvement in neonatal care has led to improved survival of premature and extremely low birth weight babies with consequent increase in ROP disease burden in the country. Telemedicine and digital imaging for ROP holds promise for early diagnosis of the fragile patients in the neonatal intensive care setting. Our data suggests that RETCAM aided digital screening is feasible for early and accurate diagnosis of ROP in Kerala. This study suggests thatfourfold babies need to be screened for the diagnosis of ROP in a neonate with the current incidence of prematurity and advancement in neonatal care in the state.
RETCAM constitutes a wide-field digital imaging tool that facilitates rapid imaging of the preterm retina. Its ease of use permits retinal photography even by trained nurses and optometrists. While a routine screen of all preterms babies by ophthalmologists remains a far-fetched dream in the state, telescreening, networking and inter-departmental collaboration can be cost-effective for diagnosis of ROP in the NICU setting.
The diagnosis of ROP at a mean 5 weeks of postnatal age in our study is in concordance with data from other workers. Babies who were born at <28 weeks of gestation were diagnosed with ROP at 6.8 weeks of life even when screening was initiated in the initial weeks of life.
While prematurity, low birth weight, respiratory distress syndrome, oxygen supplementation and respiratory support measures were all associated with ROP, our data suggested that multiple gestation and infertility treatment were not associated with ROP.
The incidence of ROP was distinctly more common in the more premature babies. 4.3% of screened late preterm babies (34 –37 weeks) were also diagnosed with ROP in our series. These babies had established traditional risk factors for ROP. While a routine screening programme for all late preterm babies may not be cost effective, our data vouches for the existing NNF guidelines which suggests selective screening of late preterm babies <2000 g or have other established risk factors for ROP.
India accounted for nearly 10% of the worldwide estimate of blindness and visual impairment due to ROP in 2010[7]. In 2010, there were an estimated to be 3,519,100preterm births in India[8].If 30% of babies had access to specialised inpatient neonatal care (intensive care or neonatal special care) and gestation-specific survival rates amongst these admitted were similar to reported rates from other low middle income country settings, 98,077 babies would have survived neonatal care and be at risk of visual impairment from ROP. Among the survivors, an estimated 16,000 would develop any ROP, with 5,000 developing severe disease requiring treatment. Our study showed an incidence of ROP as 25% while screening at risk babies (preterm, low birth weight babies with or without risk factors).Remote ROP screening has been proposed as a result of a decrease in the number of subspecialists with expertise in ROP management. As an initiation for this we started CRADLE ROP project as RETCAM based photographic screening by a trained person in the presence of an ophthalmologist.RETCAM based screening of ROP initial experience in Kerala showed a good acceptance from the neonatology centres and from the parents of the new born babies.
Study limitations: Our data was derived from limited participating centres, all of which were from the private sector. Hence the data may not be entirely representative of the Kerala population. The newborn treatment protocol, including oxygen supplementation differed between the participating centres.
CONCLUSIONS
NICU based RETCAM Shuttle screening is an effective and safe modality for early diagnosis and treatment of retinopathy of prematurity. Known the paucity of screening personnel in our state, the acceptability and feasibility of telescreening as explored in this study may help in improving neonatal care and reducing childhood blindness.
REFERENCES
- Early Treatment For Retinopathy Of Prematurity Cooperative Group. Revised indications for the treatment of retinopathy of prematurity: results of the early treatment for retinopathy of prematurity randomized trial. Arch Ophthalmol Chic Ill 1960 2003;121(12):1684–94.
- Rezai KA, Eliott D, Ferrone PJ, Kim RW. Near Confluent Laser Photocoagulation for the Treatment of Threshold Retinopathy of Prematurity. Arch Ophthalmol 2005;123(5):621–6.
- Chiang MF, Starren J, Du YE, Keenan JD, Schiff WM, Barile GR, et al. Remote image based retinopathy of prematurity diagnosis: a receiver operating characteristic analysis of accuracy. Br J Ophthalmol 2006;90(10):1292–6.
- Ells AL, Holmes JM, Astle WF, Williams G, Leske DA, Fielden M, et al. Telemedicine approach to screening for severe retinopathy of prematurity: a pilot study. Ophthalmology 2003;110(11):2113–7.
- Kumar S, Yogesan K. Internet-based eye care: VISION 2020. Lancet Lond Engl 2005;366(9493):1244–5.
- Mehta M, Adams GGW, Bunce C, Xing W, Hill M. Pilot study of the systemic effects of three different screening methods used for retinopathy of prematurity. Early Hum Dev 2005;81(4):355–60.
- Mukherjee AN, Watts P, Al-Madfai H, Manoj B, Roberts D. Impact of retinopathy of prematurity screening examination on cardiorespiratory indices: a comparison of indirect ophthalmoscopy and retcam imaging. Ophthalmology 2006;113(9):1547–52.
- Roth DB, Morales D, Feuer WJ, Hess D, Johnson RA, Flynn JT. Screening for retinopathy of prematurity employing the retcam 120: sensitivity and specificity. Arch Ophthalmol Chic Ill 1960 2001;119(2):268–72.
Leave a Comment