
Dr. Vivek Gupta,G18640, Dr. Praveen Vashist, Dr. Atul Kumar, Dr. Noopur Gupta Parakh, Dr. Suraj Singh Senjam
Abstract
WHO aims to eliminate trachoma globally by the year 2020 but the status is uncertain in India. This survey was conducted using World Health Organization approved the population-based survey methodology to assess the prevalence of active trachoma infection among children and sequelae among adults. A total of 10 previously hyper-endemic districts were surveyed and in each district, 2000 children aged 1-9 years were covered for active infections and adults above 15 years age in same households were examined for trachoma sequelae. The result showed that the active infection (TF&TI) has been eliminated in the previously hyper-endemic districts (prevalence 0.72%). Only 25% of the clinically active cases were confirmed positive on microbiological investigation by direct immune-fluorescence assay analysis. The age & gender adjusted prevalence of trichiasis was 3.3/1000. There is need to identify and treat the cases with trichiasis and its complications to eliminate trachoma in adults.
INTRODUCTION
Trachoma is an ancient scourge of mankind and was considered the most important cause of blindness at the time of Indian independence. The National Trachoma Control Program was among the initial national disease control programs launched by the Indian government in 1960s. In the initial surveys conducted under the National Trachoma Control Pilot Project, then states of Punjab, Uttar Pradesh, Bihar, Rajasthan and Gujarat were identified as hyper-endemic for trachoma (prevalence>50% in all age groups).[1]The Trachoma Rapid Assessment (TRA) surveys of 2006-2007 were conducted in ten selected districts in six previously hyper-endemic states (including new states of Uttaranchal which was split from Uttar Pradesh) and had shown considerable decline in the burden of the disease in the surveyed districts of these states. At the same time, the Car Nicobar island was identified as a hotspot for the disease in 2010 in a rapid assessment survey and led to mass drug administration of azithromycin for three consecutiveyears for the very first time in India as well as implementation of other SAFE interventions.The results of the intervention showed positive results in trachoma prevalence reassessment done in 2013 in the Car Nicobar island.[2,3]On the global front, the World Health Organization (WHO) launched the Global Elimination of Trachoma by 2020 (GET2020) in the year 1999. As part of this initiative, India too is targeting trachoma elimination. Population based prevalence surveys are considered the gold standard to assess true prevalence. Therefore,to assess the present status of trachoma in India, the NPCB National Trachoma PrevalenceSurveywas planned and implemented in the known hyperendemicdistricts where previous trachoma rapid assessments had been conducted.
METHODS
Study Setting and Sampling
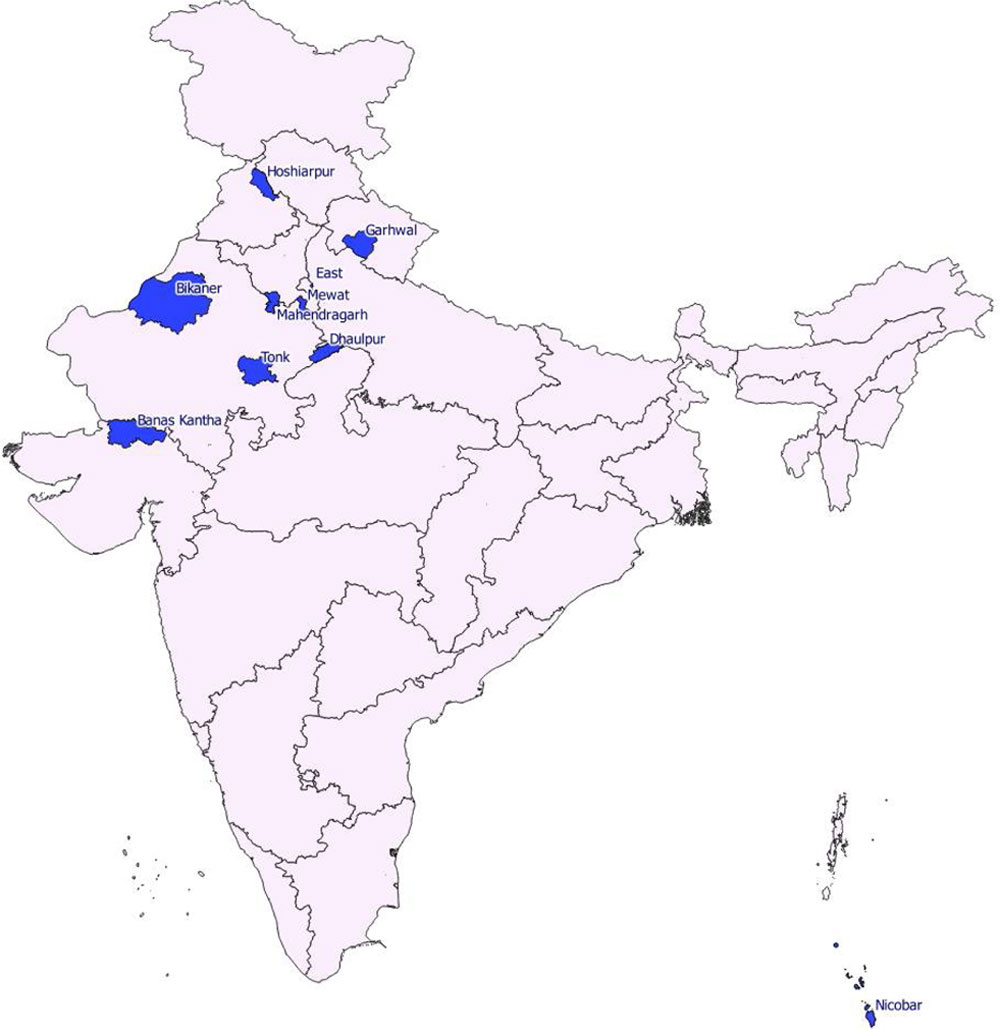
The Trachoma Prevalence Surveys were conducted in those districts, which have been marked as endemic by earlier population based surveys and where Trachoma Rapid Assessment has already been conducted in 2006-2007. In addition, prevalence survey was also done in Car Nicobar Island since this was a new area identified as endemic in a Rapid Assessment conducted in 2007. Ten districts were included in the Trachoma Prevalence Surveys.(Figure 1)
Considering the operational definition for trachoma elimination, taking prevalence of active trachomaas 5%, absolute precision 2%, design effect of 4 and response rate of 90%, sample size per district is calculated as 2,000 subjects in age group of 1- 9 years to be selected across 20 clusters in the district, each cluster having 100 chidlren. With an expected per-cluster total population size of 400, the total population coverage is estimated as 8000 individuals in one survey district.The sample size for Car Nicobar district was calculated as 800, taking prevalence of active trachomaas 3%, absolute precision 2%, design effect of 3 and response rate of 90% while accounting for a finite population correction of 6500 children 1-9 years of age in entire Car Nicobar island.
Participants were eligible for inclusion if they had completed one year of age and were usual residents of the survey area during the previous six months. The surveys were conducted using compact segment sampling technique in each clusters. In each cluster, 100 children aged 1-9 years were enrolled and all older members in the enumerated households were also examined.All households in the selected compact segment were visited and all residents were examined, including those residing in households where no eligible child was present. Revisits of locked households and individuals not available in first visit were done to maximize coverage.
Data Collection
Data collection includedinformationabout the household composition, education, occupation, assessment of overcrowding, access to water and functional latrine, presence of solid waste or animal pens, and cleanliness of faces in examined children. Household level environmental risk factors assessed were, (i) distance ofthe water source, (ii) presence of solid waste & animals around the household, and (iii) absence of functional sanitary latrine in the house. Information on main source of drinking water in dry season, main source of water for washing faces, type of toilet in household, presence of handwashing facility within 15 metres of toilet, and availability of soap or ash at handwashing facilitywas also elicited.Each clusterwas assessed for facilities like availability of primary health centre, trichiasis surgical facility, village pharmacy, market & schools in terms of the distance of these facilities.In recording the distance to a facility like PHC/trichiasis facility, it was decided that distance to all facilities within the village would be recorded in walking time while for all facilities outside the village it would be recorded in time taken by public transport.For identifying a market, respondents were queried about the distance to shops selling groceries, vegetables and other items for daily living.Household survey in the cluster continued till a minimum 100 children aged 1-9 years were examined in that cluster.
Clinical Assessments
Trained ophthalmologists examined all the available household members above one year of age. Ocular examination for ascertaining signs of trachoma on upper tarsal conjunctiva was performed with the help of 2.5x binocular corneal loupe and torch light.The ophthalmologists were trained in identification of stages of trachoma using the WHO simplified grading system.[4]Examination of eyes was done to check for follicular inflammation (TF) or intense trachomatous inflammation (TI) among children aged 1-9 years. TF wasdefined as presence of five or more follicles (at least 0.5 mm in size) in the upper tarsal conjunctiva.TI was considered in case of pronounced inflammatory thickening of the upper tarsalconjunctiva obscuring more than half of the deep tarsal vasculature of the upper lid.Active trachoma infectionwasconsidered to be present when either features TF or TI were detected in either eye.Clean faces were assessedbased on the absence of nasal or ocular discharge and absence of fliesaround nose and eyes.
Among participants aged 10+ years, examination of eyes was done to assess trachomatous trichiasis (TT) and trachomatous corneal opacities (CO).TT was assessed based on evidence of at least one eyelashrubbing the eye ball was looked for and/or recent history of removal of any inturned eyelash. Any cornealopacity (CO) was labeled to be trachomatous when co-existing signs of trachomatousinfection and signs of healed infection in form of conjunctival scarring (Arlt’s line) and trichiasiswere present. In case a person with CO was identified, visual acuity was measured in both eys using Snellens E Chart. Additionally, environmental risk factorswere also assessed.
Microbiological investigations
Conjunctival swabs were taken by the ophthalmologists from all the children found to be positive for clinical trachoma. After thorough swabbing and rolling of the entire upper conjunctival surface by a sterile swab stick, a smear was prepared on a clean teflon-coated glass slide. All the slide specimens were air dried, fixed in acetone for ten minutes and stored in an ice box for maintaining the cold chain. The samples were stored and frozen in the refrigerator (at a temperature of zero degree Celsius). On completion of the survey in the district, the samples were transferred in an ice box by ship and air with the survey team to Ocular Microbiology department at the base hospital for further analysis.
Direct Immunofluorescence assay was performed using the MicroTrak Chlamydia Trachomatis Direct Specimen Kit for detection of Chlamydia antigen. A positive control and a negative control, as provided by the supplier, were processed along with each set of specimens to ensure reliability of the reagents. Morphology for positive specimens was confirmed at a magnification of 1000x. All slides were screened for a minimum of 100 high power fields. Specimens were considered positive only if a minimum of 10 smooth elementary bodies (apple green, regular, refractile and fluorescent indicative of Chlamydia trachomatis) were observed.
Data analysis
The data entry system was designed in MS Access TM. The system had in built consistency checks and 10% of all data was again verified. After verification, the data was exported as CSV files and analyzed using the Stata 14 software.The key assessment indicators were:
- Prevalence- of active infection TI, TF and TI+TF in population aged 1-9 years
- Age-gender standardized prevalence of TT and TT with CO among population aged 15+ years.
- Prevalence of facial cleanliness in population aged 1-9 years
- Prevalence of environmental risk factors among enumerated households
- Access to treatment facilities among visited clusters
The age-sex standardized prevalence rates per 1000 population in each district were calculated by direct standardization against the 2011 census age-sex distribution of the 15+ population within the district.
RESULTS
The trachoma prevalence survey was conducted across ten districts in seven states.(Figure 1)A total of 81363 eligible individuals were enumerated in 13,802 households – of which 59251 were aged 10 years or above, 51992 were aged 15+ years, and 20929 were children 1-9 years of age. The number of participants examined was 19662 among children 1-9 years, 50603 among 10+ years old participants and 44135 among 15+year old participants with coverage rates of 93.9%, 85.4% and 84.9% respectively.
Active trachoma
Among the examined 1-9 yraged children, 139 were identified with TF, and two children with TI grade active trachoma infection were identified yielding aprevalence of active trachoma infection to be 0.72% (95% CI 0.59%-0.83%). The district with highest TF prevalence wasDholpur(2.1%) followed by Nicobar (1.4%), Mewat (1.18%), and Hoshiarpur (1.01%). Other six districts had prevalence of less than1%. Conjunctival swabs were collected from 132 children (93.6%) aged-1-9 years with a TF or TI grade trachoma infection. These samples were transported to Dr RP Centre under cold chain for assessment of Chlamydia Trachomatis. A total of 35 (26.5%) samples were positive.
Trachoma sequalae
Among the examined participants aged 15 years and more, 140 had trachomatous trichiasis (TT) and 45 of them had trachomatous corneal opacities (TT with CO). WHO has recommended TT prevalence threshold of < 1/1000 total population or < 2 /1000 population aged 15+ years in each formerly endemic district as one of the elimination criteria for trachoma. We observed an age-sex standardized prevalence of TT ranging from a high of 23.99 per 1000 in Car Nicobar to a low of 1.03 per 1000 in PauriGarhwal. The districts of Bikaner, Car Nicobar, Dholpur, East Delhi, Hoshiarpur, and Tonk had a prevalence rate over the elimination threshold of 2/1000 population aged 15+ years while Banaskantha, Mahendragarh, Mewat and PauriGarhwal had prevalence under the elimination threshold.
Clean faces, water, hygiene and sanitation
Overall, 15.7% children had unclean faces, prevalence being highest in Mewat (40%) and Dholpur (31.8%), while prevalence of under 10% was observed in Banaskantha, Hoshiarpur, Nicobar and East Delhi.A total of 13802 households were assessed by the survey teams for environmental risk factors.In 2.5% households, water source was located beyond 30 minutes walking distance. Non-availability of water source within 30-minute walking distance was a major risk factor in Mewat with nearly 10.57% households affected, Dholpur (9.2% households) and in Car Nicobar (6.7%) while excellent access was observed in Banaskantha, Bikaner, East Delhi, Hoshiarpur, Mahendragarh, PauriGarhwal and Tonk. More than half (55%) of the surveyed households had solid waste or animal pens within 20 metres and functional latrines were absent in 33% households.Poor environmental hygiene was observed across all the districts with overall 55.4% households having solid waste or animal present within 20 metres of the household. The worst affected district included Dholpur, Car Nicobar, Tonk and Mahendragarh. Almost one-third households lacked access to a functional latrine. In Dholpur, 73% households lacked access to a functional latrine, and a poor status was also observed in Tonk (51.9%), Mewat (48.2%), and Banaskantha (43.2%). Good access to functional latrine was observed in Car Nicobar (2.5% lacking access), Bikaner (7.2% lacking access), and Hoshiarpur (9.7%).
Access to treatment facilities, market and primary school among visited clusters
It was observed that a primary health care facility was located within 30-minute local travel time across all clusters surveyed in Tonk, East Delhi and Hoshiarpur while 15% clusters were located at over 2-hour travel time from a primary health care centre in PauriGarhwal. Access to trichiasis surgery facilities was particularly lacking in visited clusters PauriGarhwal while in Mewat, 80% clusters were located at 30 minute-<2-hour travel time from a trichiasis surgery facility. In Dholpur as well, 50% clusters were located at 30 minute-<2-hour travel time from a trichiasis surgery facility. All the visited clusters had access to a primary school in under 30 minutes. The access to market was also very good in all districts except Mewat.
CONCLUSIONS AND RECOMMENDATIONS
A low 0.7% prevalence of active trachoma infection was observed. None of the surveyed districts reported more than 5% prevalence/proportion of active trachoma. Our results suggest that active trachoma is no longer a public health problem in India and that India has met the goal of trachoma elimination. TTcontinues to be common in certain pockets and surgical interventions are required.
All states which were previously hyperendemic and states where trachomatous trichiasis cases have been reported need to develop a strategy for community based case finding of patients of trachomatous trichiasis. This can be implemented through involvement of ASHAs and other community based volunteer workers with due incentives. On an average 2-3 cases are expected in each ASHA worker’s area (1000 total population) in previous hyperendemic states. These cases must be provided free entropion surgery/ treatment in local hospitals. A careful record of each case identified and its management status must be maintained as per the WHO Guidelines. Interventions for prevention of spread of trachomashould be sustained byensuring cleanliness of environment, access to sanitary toilets, availability of safe water and promoting facial cleanliness. The ongoing Swacch Bharat program of the central government as well as other Water, Sanitation and Hygiene programs (WASH) must be prioritized in all the districts since they are the most effective way for preventing acute trachoma infections among children.Before India can be certified as having eliminated trachoma, adequate surveillance of the disease must be done all over the country. Monthly data on indicators of trachoma surveillance as per WHO guidelines must be regularly sent to the NPCB. A central monitoring team should be constituted to ensure effective the implementation of case finding, surgery, preventive and surveillance components of the plan in the country.Finally, after a 3 year period (by 2020) of effective implementation, surveillance and monitoring, India will be in a position of declaring Elimination of Trachoma from the country.
Table 1:Active Trachoma Infection Indicated by Prevalence of Follicular Inflammation (TF) and Intense Inflammation (TI),and Unclean Faces among Participants Aged 1-9 years
| District | Examined | TF
N (%) |
TI
N (%) |
TF+TI
N (%) |
Unclean face
N (%) |
| Banaskantha | 2,058 | 9 (0.4) | 0 (0) | 9 (0.4) | 114 (5.5) |
| Bikaner | 2,101 | 2 (0.1) | 0 (0) | 2 (0.1) | 297 (14.1) |
| Car Nicobar | 831 | 12 (1.4) | 1 (0.12) | 13 (1.6) | 53 (6.4) |
| Dholpur | 2,129 | 45 (2.1) | 1 (0.05) | 46 (2.2) | 676 (31.8) |
| East Delhi | 2,090 | 11 (0.5) | 0 (0) | 11 (0.5) | 206 (9.9) |
| Hoshiarpur | 2,086 | 21 (1) | 0 (0) | 21 (1) | 122 (5.8) |
| Mahendragarh | 2,119 | 2 (0.1) | 0 (0) | 2 (0.1) | 221 (10.4) |
| Mewat | 2,113 | 25 (1.2) | 0 (0) | 25 (1.2) | 841 (39.8) |
| PauriGarhwal | 2,068 | 3 (0.1) | 0 (0) | 3 (0.1) | 236 (11.4) |
| Tonk | 2,067 | 9 (0.4) | 0 (0) | 9 (0.4) | 323 (15.6) |
| Total | 19,662 | 139 (0.7) | 2 (0.01) | 141 (0.72) | 3089 (15.7) |
Table 2: Prevalence of Trachomatous Trichiasis (TT), and Trachomatous Corneal Opacity (CO) among participants aged 15 years and older
| District | Examined | TT
N (Prevalence per 1000) * |
TT with CO
N (Prevalence per 1000) * |
TT Total
N (Prevalence per 1000) * |
| Banaskantha | 4397 | 3 (7.5) | 2 (0.5) | 5 (1.05) |
| Bikaner | 4914 | 6 (1.2) | 2 (0.4) | 8 (2.06) |
| Car Nicobar | 1561 | 39 (25.0) | 6 (3.8) | 45 (23.99) |
| Dholpur | 4337 | 7 (1.6) | 11 (2.5) | 18 (4.45) |
| East Delhi | 4466 | 5 (1.1) | 1 (0.2) | 6 (2.14) |
| Hoshiarpur | 4468 | 11 (2.5) | 8 (1.8) | 19 (6.64) |
| Mahendragarh | 5427 | 2 (0.4) | 6 (1.1) | 8 (1.34) |
| Mewat | 4252 | 2 (0.5) | 3 (0.7) | 5 (1.15) |
| PauriGarhwal | 4901 | 3 (0.6) | 1 (0.2) | 4 (1.03) |
| Tonk | 5412 | 17 (3.1) | 5 (0.9) | 22 (3.76) |
| Total | 44135 | 95 (2.2) | 45 (1.02) | 140 (3.45) |
*Age-sex standardized prevalence figures per 1000 population have been reported for TT among 15+year population examined in trachoma prevalence surveys;
Table 3: – Environmental Risk Factors for Trachoma among Visited Households
| District | Households visited | Water Source unavailable within 30-minute walking distance
N (%) |
Solid waste/ animal present within 20 meters
N (%) |
Functional latrine absent
N (%) |
| Banaskantha | 1465 | 0 (0.00) | 470 (32.08) | 633 (43.21) |
| Bikaner | 1432 | 0 (0.00) | 791 (55.24) | 103 (7.19) |
| Car Nicobar | 446 | 30 (6.73) | 356 (79.82) | 11 (2.47) |
| Dholpur | 1336 | 123 (9.21) | 1171 (87.65) | 975 (72.98) |
| East Delhi | 1526 | 0 (0.00) | 783 (51.31) | 494 (32.37) |
| Hoshiarpur | 1473 | 0 (0.00) | 434 (29.46) | 143 (9.71) |
| Mahendragarh | 1624 | 4 (0.25) | 1097 (67.55) | 465 (28.63) |
| Mewat | 1202 | 127 (10.57) | 751 (62.48) | 579 (48.17) |
| PauriGarhwal | 1700 | 45 (2.65) | 674 (39.65) | 283 (16.65) |
| Tonk | 1598 | 14 (0.88) | 1120 (70.09) | 830 (51.94) |
| Total | 13802 | 343 (2.48) | 7647 (55.41) | 4516 (32.72) |
Figure 1: Sites of Trachoma Prevalence Surveys -2013-17
REFERENCES
1. Gupta UC, Preobragenski VV. Trachoma in India – Endemicity and epidemiological study. Indian J Ophthalmol 1964;12(2):39.
2.Malhotra S, Vashist P, Gupta N, Kalaivani M, Satpathy G, Shah A, et al. Prevalence of Trachoma in Car-Nicobar Island, India after Three Annual Rounds of Mass Drug Administration with Azithromycin. PloS One 2016;11(7):e0158625.
3.Vashist P, Gupta N, Rathore AS, Shah A, Singh S. Rapid assessment of trachoma in underserved population of Car-Nicobar Island, India. PloS One 2013;8(6):e65918.
4.Thylefors B, Dawson CR, Jones BR, West SK, Taylor HR. A simple system for the assessment of trachoma and its complications. Bull World Health Organ 1987;65(4):477–83.
Leave a Comment