
Dr. Vijay Kumar.S, K20263, Dr. Saravanan V R, Dr. Virna Shah, Dr. Reshma K.T. Balan
Abstract:
AIM: To study the correlation between ganglion cell layer (GCL) thickness in differentiating ischemic optic neuropathy (NAION) and optic neuritis (ON) using optical coherence tomography (OCT) in acute phase.
METHODS: prospective case control study of 40 cases and 40 age matched controls, the GCL and RNFL thickness were compared between NAION and ON with age matched controls and the mean thickness in each quadrant was analyzed using unpaired t-test.
RESULTS: Difference between superio -inferior quadrant GCL thickness was significant in NAION (5.4-7.8mm) compared to ON (3.1-3.8mm).
CONCLUSION: Analysis of GCL thickness can be used as noninvasive, cost-effective tool to differentiate NAION and ON in cases with overlapping clinical picture.
INTRODUCTION
Optic neuritis (ON) and non-arteritic anterior ischemic optic neuropathy (NAION) are the two most common types of optic neuropathies in adults. They also share a host of overlapping clinical features, which poses the difficulty in distinguishing between the two. However, differential diagnosis is generally possible based on age of onset, presence of pain, rate of recovery and type of visual field loss. Optic disc edema, is most commonly associated with NAION, although it may also be seen with one – third of ON cases (Warner et. al 1997; Galetta et al. 2011).
AIM :
To differentiate between optic neuritis and Non arteritic anterior ischemic optic neuropathy using optical coherence tomography in acute phase.
STUDY :
A prospective study was undertaken in the outpatient department of Aravind eye hospital, Coimbatore, between January to May 2017.
MATERIALS AND METHODS :
A total of 40 patients with acute optic neuritis and 40 NAION patients were enrolled along with their age matched controls, after obtaining informed consent. OCT is done to assess the mean GCL thickness, especially in the superior and inferior quadrant and the absolute values of their differences were compared between ON and NAION .
Study design :
A prospective, observational study was performed to compare the mean GCL thickness between eyes with NAION and those with ON. A case control analysis was performed using healthy controls, age matched to each patient, evaluated with OCT at one point in time.
Study area: Outpatient department of Aravind eye hospital, Coimbatore.
Study Size: 40 patients in optic neuritis group and 40 patients in ischemic optic neuropathy group and age matched controls
Diagnosis criteria: On the basis of clinical presentation
Nonarteritic Ischemic Optic Neuropathy:
Painless swelling of the optic disc
Sudden visual loss,
Altitudinal field defect,
Color deficit,
Optic nerve haemorrhages,
Pallor of the disc
Optic disc crowding of the other eye (after excluding other causes of optic neuropathy and confirmed by the stable condition at follow up)
Optic neuritis:
Sudden, painful loss of vision,
Usually with a central scotoma,
Color deficit,
Mild or no optic disc swelling,
Improvement with follow up
Study details :
Based on the diagnostic criteria, patients were selected after a complete neuro – ophthalmological examination which included the assessment of the best corrected visual acuity using Snellen’s optotypes. Color vision discrimination was assessed using Ishihara’s charts. Fundus examination was done and high definition OCT (HD-OCT). Each subject had both their eyes scanned using standard acquisition protocol. The macular cube (521 9 128 line scans) were used to assess GCL.
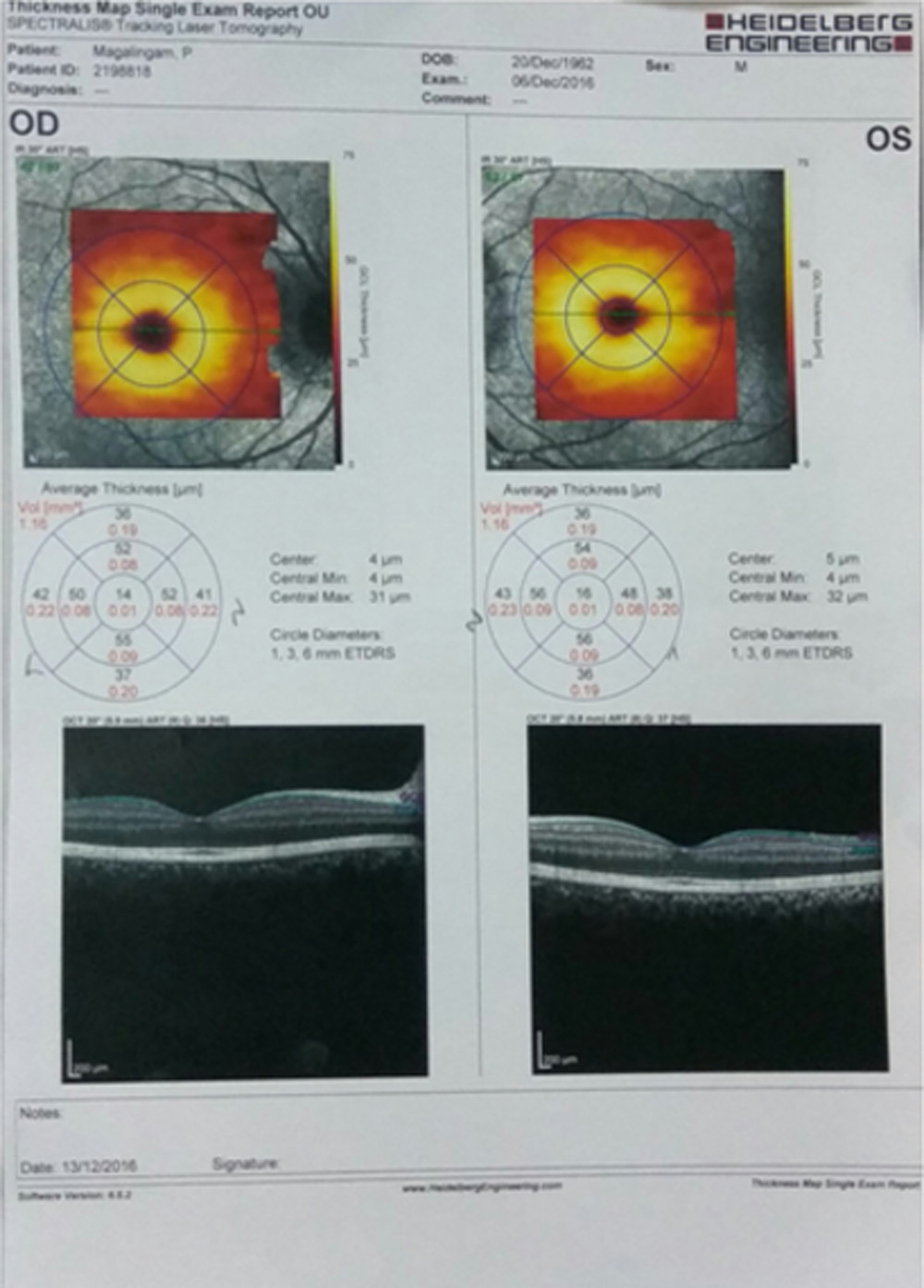
The scanned area was 6mm in the protocol with no signal averaging. Signal strength (0 – 10 arbitrary units) was used to assess the quality of the obtained images. Scans with signal strength of more than 6 units were included in the study. Automatic algorithms were used to determine GCL thickness, using HD – OCT (SPECTRALIS).
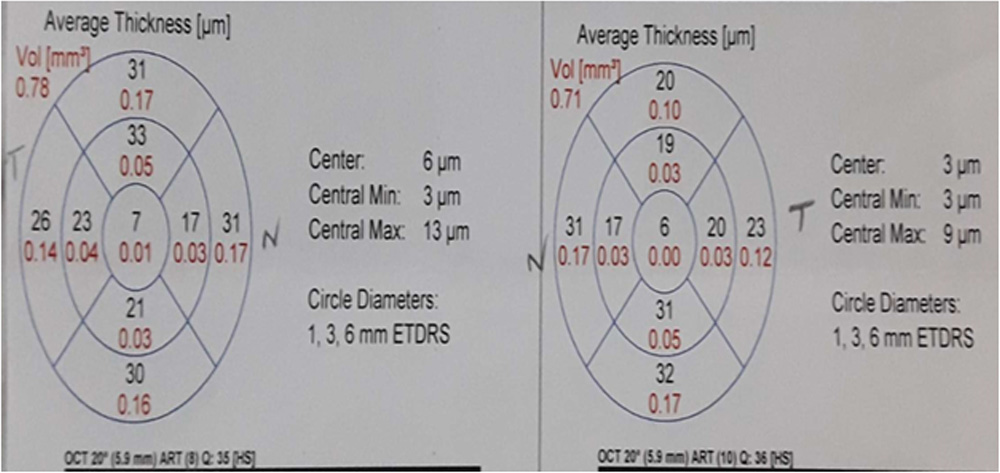
GCL analysis was done by calculating the thickness of the ganglion cell layer and the inner plexiform layer.The GCL thickness was measured in different parts of the macula, around the foveal centre: temporal superior, superior, nasal superior, nasal inferior, inferior, temporal inferior and global. The average, minimum and sectoral thickness of the GCC are measured in an elliptical annulus around the fovea. Global GCL thickness values, and those in each of the said location, expressed in microns (µ), were used for analysis.
RESULTS:
There were 40 eyes in the NAION cohort and 40 eyes in the ON cohort. Mean age was 61.3 ± 10.6 years in the NAION cohort and 35.9 ± 11.6 years in the ON cohort. Mean age of age-matched control cohorts was 62.0 ± 11.8 and 35.0 ± 11.6 years, respectively. There were 13 women and 27 men in the NAION cohort and 21 women and 19 men in the ON cohort. ON-matched controls had 14 women and 26 men. NAION-matched controls had 23 women and 17 men.
Mean time from onset of symptoms to initial presentation was 10.7 ±6.6 days in NAION and 11.7 ± 8.6 days in ON (p = 0.67). There was a significant hemispheric difference in GCL thickness in the NAION cohort than the ON cohort (infero-superior): acute onset (p = 0.032).
Mean hemispheric difference was 5.7 µm in the NAION cohort , compared with 1.1 µm in the ON group. Healthy controls had a mean hemispheric difference of 1.9 lm in the NAION age matched cohort and 1.1 lm in the ON age-matched cohort. Six eyes with NAION showed bihemispheric loss, with significant thinning in both superior and inferior hemispheres and a hemispheric difference in GCL thickness of 3µm or less.
Mean GCL thickness in ON patients was not significant compared to age matched controls as in NAION compared to age-matched controls .
| Mean of Superior in ON | Mean of Superior in NAION | Mean of Inferior in ON | Mean of Inferior in NAION | |
| Case | 63.4 | 66.9 | 64.5 | 72.6 |
| Control | 71.7 | 71.5 | 70.6 | 70.7 |
DISCUSSION:
This study demonstrates that ganglion cell loss in NAION follows an altitudinal pattern, resulting in a difference in mean GCL thickness between the superior and inferior hemispheres of the macula that is significantly greater than that found in ON or in healthy controls. This difference had a mean of 5.7 µm. This corresponds to the difference in visual field defects typically found between NAION and ON.
NAION is most commonly characterized by an altitudinal field defect, whereas diffuse visual field loss or central scotoma is most often found in ON (Keltner et al. 1993; Gerling et al. 1998; Horowitz et al. 2010). The segmental ischemia of the optic nerve is associated with edema initially, which may lead to subsequent damage to other areas of the optic nerve (Ho et al. 2013; Miller & Arnold 2015). Aggarwal et al. (2012) showed that GCL thinning in NAION correlated with visual field loss when visual field defect was superior or inferior, although 16 out of 23 eyes in their study had bihemispheric loss.
We found in our analysis, the difference in mean hemispheric thickness in NAION showed a significant difference statistically when compared with ON eyes or with control eyes. This distinctive, altitudinal pattern was also clearly seen upon viewing OCT images of many of the NAION patients.
This is a possible critical factor in the differentiating a patient with ON or NAION who exhibits features common to both diseases. We found that thinning of the ganglion cell layer is evident in both ON and NAION as early as 11 days after onset of symptoms when compared to age-matched controls.
Previous studies have shown RNFL thinning in NAION to be statistically greater in the superior quadrant than the inferior quadrant, but not until 6 months after onset, when the initial swelling has resolved (Contreras et al. 2007; Horowitz et al. 2010). Other studies have shown that GCL thickness may be a better metric by which to evaluate the degree of damage in both ON (Syc et al. 2012; Ratchford et al. 2013; Gabilondo et al. 2015; Kupersmith et al. 2015) and NAION (Aggarwal et al. 2012; Keller et al. 2015) during the acute phase, because the ganglion cell layer, as opposed to the retinal nerve fibre layer, is not affected by the initial oedema that is frequent in ON and ubiquitous in NAION. Our finding that ganglion cell loss can be seen at less than 2 weeks.
In a recent study, Kupersmith et al. (2015) found a significant difference in GCC thickness between affected and unaffected eyes with multiple sclerosis (MS) at 1 month after onset of ON. They found no significant difference in GCL thickness at presentation, on average 7.3 days after onset (Kupersmith et al. 2015). It is possible that the initial difference was underestimated due to progressive, subclinical GCL thinning that occurs in clinically unaffected eyes of patients with MS (Davies et al. 2011; Ratchford et al. 2013).
Meta-analysis by Petzold et al. (2010) found a mean difference in RNFL thickness between ON and control eyes of 20.38 lm. Our data is consistent with this, with a difference of 23.2 lm at 16 + weeks after onset. The presence of three NAION eyes with subretinal fluid out of the 32 eyes in our study is consistent with findings by Hedges et al. (2008) that subretinal fluid occurs in approximately ten per cent of NAION patients. Although the ganglion cell loss of these patients could not be accurately evaluated, the presence of subretinal fluid may be another way to rule out a diagnosis of optic neuritis in favour of NAION.
Patients treated with systemic corticosteroids within 2 weeks of onset may have faster resolution of optic disc oedema, as well as better recovery of visual fields and acuity (Hayreh & Zimmerman 2008). Experimental models have suggested that the initial swelling in NAION results in compression by the nerve sheath, leading to a compartment syndrome that increases the degree of ischemic damage (Burde 1993; Hayreh & Zimmerman 2008; Levin & Danesh-Meyer 2008; Hayreh 2009; Bernstein et al. 2011), raising the possibility that early treatment targeting this initial swelling might have an impact on the extent of neuronal damage and visual loss).
Our findings help in recognizing acute NAION which is crucial as appropriate treatment can be started early and vision can be salvaged. Optic neuritis and ischemic optic neuropathy may often be misdiagnosed for one another in overlapping scenarios such as a middle aged patient with disc edema, and also in younger patients with NAION and older patients with ON. We have shown that altitudinal difference in GCL thickness as measured with OCT is significantly greater in NAION than in ON, which may play a role in distinguishing these conditions. An altitudinal loss of ganglion cells supports a diagnosis of NAION, whereas a more diffuse loss is indicative of ON. (bihemispheric loss, as seen in one fourth of our patients, does not rule out a diagnosis of NAION).
CONCLUSION:
Though clinical assessment remains the mainstay of diagnosing optic neuritis and NAION, OCT-GCL thickness (Superior/inferior) might aid in differentiating the two in overlapping scenarios .Since we have studied in acute stage of the disease , a long term follow-up with serial OCTs will help in detailed evaluation of the GCL thickness in both the diseases.
REFERENCES:
1.Distinguishing ischaemic optic neuropathy from optic neuritis by ganglion cell analysis: Natalie Erlich-Malona,1 Carlos E. Mendoza-Santiesteban,1,2,3 Thomas R. Hedges III,1 Nimesh Patel,1 Caitlin Monaco1 and Emily Cole , Acta ophthalmologica 2016
2.Aggarwal D, Tan O, Huang D & Sadun AA (2012): Patterns of ganglion cell complex and nerve fiber layer loss in nonarteritic ischemic optic neuropathy by Fourierdomain optical coherence tomography.Invest Ophthalmol Vis Sci 53: 4539–4545
3.Contreras I, Noval S, Rebolleda G & Munoz-Negrete FJ (2007): Follow-up of nonarteriticanterior ischemic optic neuropathy with optical coherence tomography. Ophthalmology14: 2338–2344.
4.Bernstein SL, Johnson MA & Miller NR (2011): Nonarteritic anterior ischemic optic neuropathy (NAION) and its experimental models. Prog Retin Eye Res 30: 167–
5.Ho JK, Stanford MP, Shariati MA, Dalal R & Liao YJ (2013): Optical coherence tomography tudy of experimental anterior ischemic opticneuropathy and histologic confirmation.Invest Ophthalmol Vis Sci 54: 5981–5988.
6.Burde RM (1993): Optic disk risk factors for nonarteritic anterior ischemic optic neuropathy.Am J Ophthalmol 116: 759–764.
7.Keller J, Oakley JD, Russakoff DB, Andorra- Ingles M, Villoslada P & Sanchez-Dalmau BF (2015): Changes in macular layers in theearly course of non-arteritic ischaemic optic neuropathy. Graefes Arch Clin Exp Ophthalmol 254: 561–567.
8.Keltner JL, Johnson CA, Spurr JO & Beck RW (1993): Baseline visual field profile of optic neuritis. The experience of the optic neuritis treatment trial. Optic Neuritis Study Group. Arch Ophthalmol 111: 231–234.
9.Syc SB, Saidha S, Newsome SD et al. (2012): Optical coherence tomography segmentationreveals ganglion cell layer pathology after optic neuritis. Brain 135: 521–533
10.Kupersmith MJ, Garvin MK, Wang JK, Durbin M & R KARDON (2015): Retinal ganglion cell layer thinning within one month of presentation for optic neuritis.Mult Scler 22: 641–648.
11.Gabilondo I, Martinez-Lapiscina EH, Fraga- Pumar E et al. (2015): Dynamics of retinal injury after acute optic neuritis. Ann Neurol 77: 517–528.
12.Petzold A, de Boer JF, Schippling S, Vermersch P, Kardon R, Green A, Calabresi PA & Polman (2010):Optical coherence tomography in multiple sclerosis: a systematic review and meta- analysis.Lancet Neurol 9:921–932.
13.Hayreh SS & Zimmerman MB (2008): Nonarteritic anterior ischemic optic neuropathy: role of systemic corticosteroid therapy. Graefes Arch Clin Exp Ophthalmol 246: 1029–1046.
14.Miller NR & Arnold AC (2015): Current concepts in the diagnosis, pathogenesis and management of nonarteritic anterior ischaemic optic neuropathy. Eye 29: 65–79.
Leave a Comment