

Dr. Maneesh Bapaye, B12628, Dr. Natarajan S, Dr. Mahesh Shanmugam P
![]()
![]()
Penetrating ocular injuries are associated with retained intraocular foreign body (IOFB) in 17-41%1 of patients. It is an important cause of visual morbidity and blindness especially in working age population. In majority of patients the IOFB is retained in posterior segment of the eye. Three port pars planavitrectomy with internal removal of IOFB is a standard procedure for removal of posterior segment IOFB. Advent of small gauge vitrectomy has lead to excellent visual and anatomical outcomes in majority of cases. While various instruments like intraocular foreign body magnets and various types of forceps have been successfully used for removal of IOFB, removal of large, spherical, non magnetic IOFBs like shot gun pellets, stones or large glass fragments remains challenging in majority of cases. We introduce a new device that can be used in such cases successfully.
Description of instrument:
The Claw (Fig.1) is an extendable foreign body forceps (Epsilon, USA). It is designed for secure grasping & removal of large, non magnetic foreign bodies from vitreous cavity. The instrument consists oftitaniumhandle and 19G stainless steel shaft. A Teflon plunger is housed inside the titanium handle. To and fro movement of the plunger is controlled by a screw shaped knob placed at center of the shaft. When deployed the plunger pushes the claw shaped prongs housed inside the stainless steel shaft in a symmetrical manner. The stainless steel shaft has outer diameter of 1.2 mm and inner diameter of 0.9mm. Length of the shaft is 27 mm.The retractable claw is made of 4 prongs of Nitinol wire.Nitinol is alloy of nickel and titanium which shows excellent shape memory and psuedoelasticity. Because of its biocompatible nature Nitinol is widely used in many medical devices. When completely extended the prongs measure 14mm and open up to 8-8.5mm.Theprongs is retracted fully into metallic cylinder while introducing in the eye.Conjunctival opening and enlargement of sclerotomy is needed to introduce the forceps in vitreous cavity.The distal ends of the prongs are bulbous and hence non-traumatic to the retina.Forceps can be held by comfortable grip while prongs can be extended or retracted to extent required with the knob using one of the fingers. Once IOFB is grasped in the prongs of the claw are retracted to hold the IOFB in-situ. The prongs twine around the IOFB to hold it secured manner. The forceps can be reused after autoclave.
The Claw has been used by surgeons for removal of various large and non magnetic IOFBs in different clinical settings.
Clinical Scenario 1.
A 42 year old male presented with history of penetrating trauma in right eye while standing beside a stone cutter. At presentation visual acuity was no light perception. Clinical examination revealed scleral tear on nasal side. Posterior extent could not be ascertained. Cornea was clear. Hyphema precluded view of fundus. Eyeball appeared collapsed. CT scan examination showed a large radio-opaque IOFB with collapsed eyeball (Fig 2). Surgery was planned for wound exploration and suturing and removal of IOFB to prevent traumatic endophthalmitis. Intraoperatively scleral wound was explored to the posterior extent after disinsertion of medial rectus muscle and sutured with 6-0 vicryl suture with hand over hand technique. Lensectomy was performed through limbus. Standard 3 port pars planavitrectomy performed with 23G TSV system. A large stone IOFB along with total RD and vitreous hemorrhage were noted. Posterior vitreous detachment was absent. IOFB was released of all vitreous attachments and IOFB was lifted to papillary plane using the Claw (Fig 3). Superior 180 degrees limbal section was made and IOFB removed with superior rectus holding forceps by handshake technique. It measured 10mm X 5mmX 4mm (Fig 4).
Clinical Scenario 2.
In July 2016, Kashmir valley erupted with social unrest of unprecedented proportions. Extensive stone pelting was resorted to by unruly crowds. Security forces were forced to use pellet guns for crowd control. However this resulted in extensive ocular injuries. Over 2000 subjects suffered pellet injuries. Of these 855 had ocular injuries. 118 patients had posterior segment IOFBs.
The pellet gun is technically known as 12 bore pump action gun.These guns are manufactured at ordinance factory at Ishapore, West Bengal. A cartridge of pellet gun contains several hundred pellets which spread over a large area once fired. Cartridges which containpellets or shots of various sizes measured on scale BB and 1-9.Pellets are marked as BB are largest in size, shot no.1 is smaller than shot BB and shot no. 9 is the smallest of all.The size of these pellets varies from 2.03mm(Size 9) to 4.57mm (Size BB) .The pellets are made of lead, usually spherical in shape and have smooth surface, resembling ball bearings. It makes them difficult to remove from eye. The ‘Claw’ was used to remove these IOFBs (Fig.5). Two of the authors, Drs.SN & MPS were surgeons in-charge of operating on these patients.
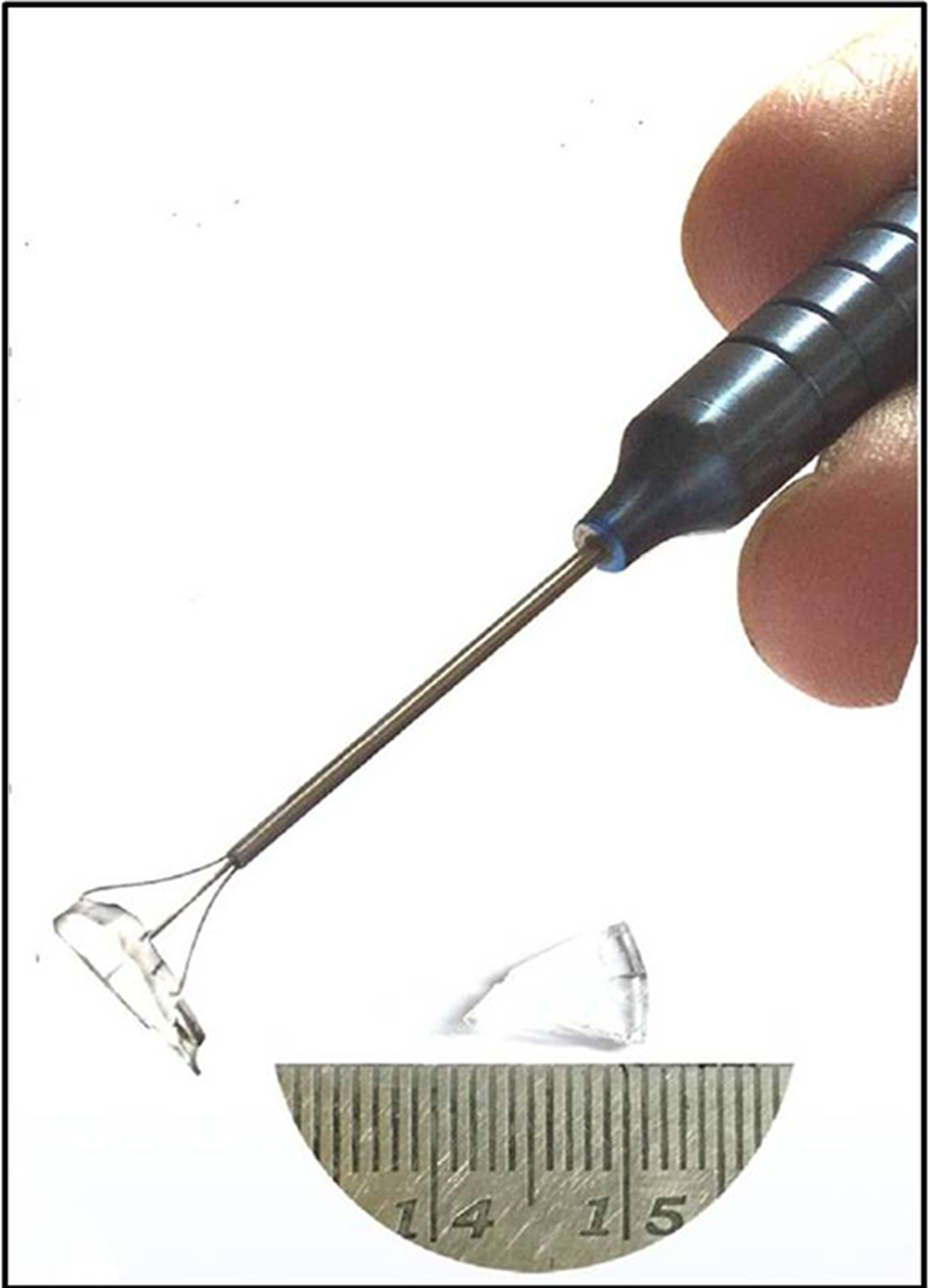
The Claw has also been used in vivo to pick up various objects like large glass pieces without crushing them into smaller splinters (Fig. 6)
Discussion:
Removal of IOFB in setting of penetrating trauma is challenging scenario. In majority of cases the IOFBs are small in size and magnetic in nature, which makes removal of these IOFB amenable to magnets for removal. However when IOFB is non-magnetic and/or large in size (4 mm or more), there are limited options available for holding the IOFB securely inside the vitreous cavity.
The instrumentdesign was based on concept of dormia basket that has been extensively used in urology for removal of proximal ureteric stones. The dormia basket consists of retractable basket of nitinol cables which is passed beyond the ureteric stone in retracted state and then deployed while it is pulled out so as to catch the stone within the basket and then removed. Similar principle is also used in sialoendoscopy for removal of salivary stones. We started by working with design concept of a retractable nitinol basket. In case of IOFBs in ocular trauma, the major differences from prior mentioned applications of basket design are variability in shape of IOFBs rather than spherical shape of ureteric or salivary stone. The IOFBs are lying on relatively flat surface rather than tubular lumen and can potentially float in liquid environment of vitrectomised eye prior to removal. Claw design was used as it enables the surgeon to hold the IOFB securely by approaching in antero-posterior direction and picking it up from retinal surface.
Various authors have described snare or loop design that can hold an irregular IOFB. Erkagun et al2& Murthy et al3have described cost effective & disposable snares using thick suture materials, which can be quickly assembled prior to surgery and disposed off once used. Eckardt C et al4 (Memory snare IOFB Extractor; DORC, Zuidland, Holland) and Smith JM et al5 (QuikStik; Microsurgical technology, Redmond WA) have described expandable memory loop devices which contain expandable nitinol loop. While all these elegant devices can be effectively used linear IOFB, it is difficult to hold larger and spherical IOFB. Snare design devices can cause repeated slippage of IOFB. Iatrogenic trauma by slipped IOFB can lead to less than satisfactory anatomical and visual outcomes, especially if macular region is affected.
Different types of forceps have also been used in these cases with large IOFBs. Hickinbotham D et al6 have described diamond coated forceps to hold IOFB in vitreous cavity. However the opening of prongs is not quite as wide to hold large IOFB and presence of 2 prongs makes removal of spherical IOFB difficult. Liang S et al7have used micro-alligator forceps for removal of large IOFB. To introduce this forceps needs very large sclerotomy. Crushing force of forceps can also be significant leading to crushing or splintering of the IOFB prior to removal. This may further complicate the situation for the surgeon. McCarthy M.J. et al8 have used ureter stone forceps itself. This has very large handle and needs assistant to operate the instrument.
The claw offers various advantages over all of the aforementioned devices. The 4 prongs offer secure grip without crushing or splintering the IOFB. As mentioned before, the IOFB can be approached in antero-posterior direction and picked up from flat retinal surface. Chances of IOFB slippage and thereby causing retinal trauma are minimized. It makes other procedures like creating limbal incision or enlargement of sclerotomy with other hand while FB is securely held with one hand in mid-vitreous cavity or at the pupillary plane. The forceps can be sterilized with standard methods and thus reusable and cost effective option. Design of 4 pronged claw shaped disposable forceps has been described by Hildebrandt C el al9 of University of Wisconsin, Madison as a part of term project for biomedical engineering course. However in their instrument, which was a prototype, the claws couldn’t be retracted fully in metallic cylinder. This instrument was never used in human subjects.
References:
- Shock JP, Adams D. Long-term visual acuity results after penetrating and perforating ocular injuries. Am J Ophthalmol. 1985;100(5):714-718.
- Erakgun T, Akkin C, Mentes J. Management of the posterior segment foreign bodies with a simple snare. Retina 2003;23:858-860
- Murthy KR, Murthy PR. Foreign body snare for the removal of large non magnetic intravitreal foreign bodies and dislocated lens nuclei/IOLs. Retina. August 2003: Vol23(4), 584
- Eckardt C, Eckert T, Eckardt U. Memory snare for extraction of intraocular foreign bodies. Retina. 2006: Vol 6(7), 845-7
- Smith JM, Hwang RY, Erlanger M, Olsen JL. A new multifunctional expandable memory loop design. Retina 2015: Vol 35(10), 2154-2157
- Hickingbotham D, Parel J-M, Machemer R. Diamond-coated all-purpose foreign-body forceps. Am J Ophthalmol 1991;91: 267–268.
- Liang S, Guangming Wan, Xiujuan Li, Xiaoqiang Liu, Yu Zhu: Removal of a Giant Nonmagnetic Intraocular Foreign Body Using Micro Alligator Forceps. Ophthalmic Surgery, Lasers & Imaging Retina. 2014 : Vol. 45(3), 228-230.
- McCarthy MJ, Pulido JS, Soukup B. The use of ureter stone forceps to remove a large intraocular foreign body. Am J Ophthalmol 1990;110:208–209.
- Hildebrandt C, Kim A, Phung R, Strebel A. Device for extraction of non-metallic intraocular foreign bodies. BME 301. University of Madison-Wisconsin.
Legends
Legends
- Fig1: The Claw
- Fig2: CT scan images showing deformed eyeball with large IOFB
- Fig3: Large IOFB (Stone) being held in mid vitreous cavity using the claw
- Fig4: Composite depicting size of IOFB
- Fig5: Shotgun pellet after removal from eye
- Fig6: Irregular shaped glass piece held in-vivo
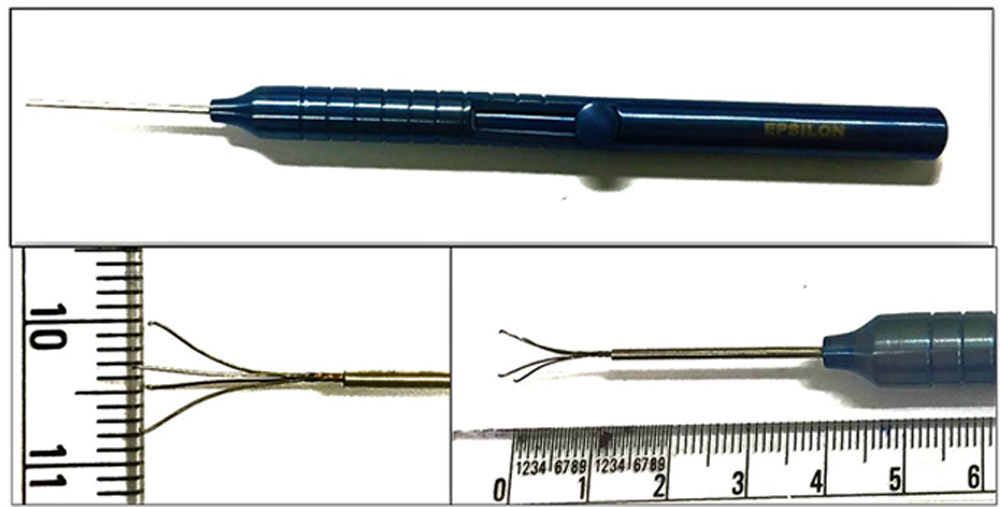
Figure 2:

Figure 3:
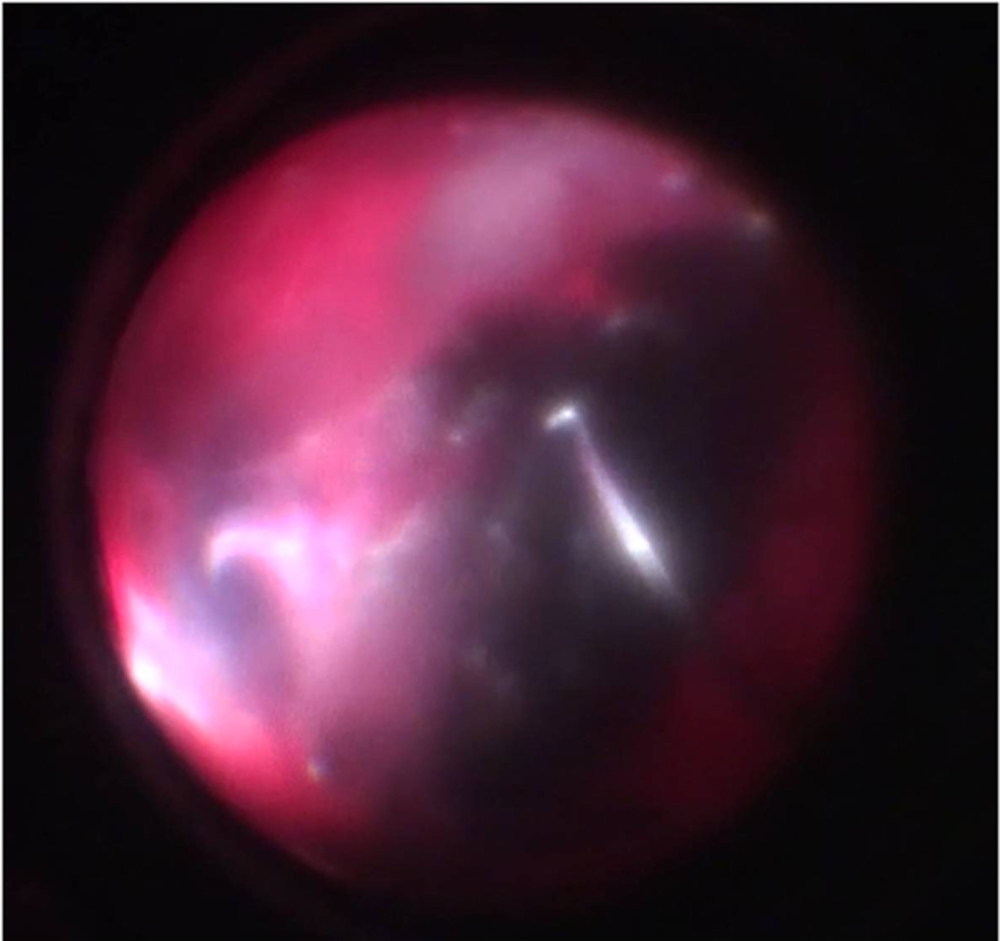
Figure 4:

Figure 5:
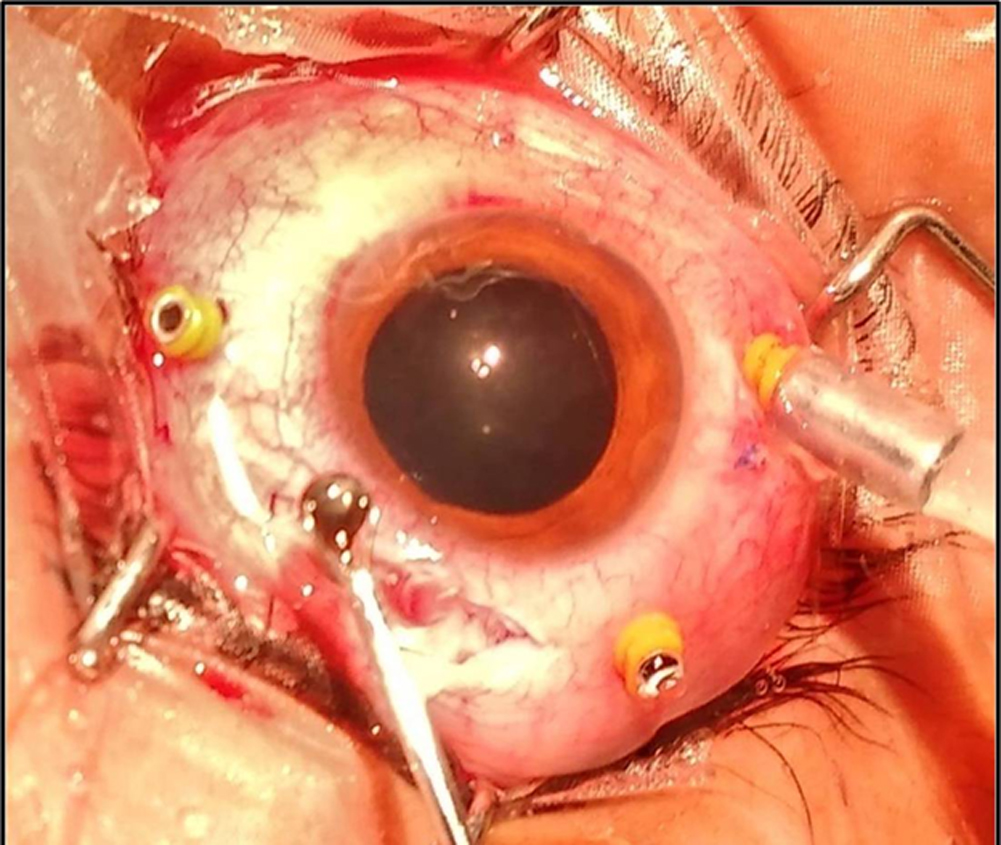
Figure 6:
Leave a Comment