
Dr. Kaushik Murali, M10521, Dr. Vidhya C
ABSTRACT:
Aim:To evaluate safety of reconstituted atropine 0.01% eye drops for Indian children with myopic progression.
Methods:50 consecutive children with progressive myopia were put on atropine 0.01%.Ocular exam including near vision, near point of accommodation (NPA), pupil size was done.Subjective symptoms of glare & photophobia noted.Parameters converted to Ease of Vision lndex(EVI) & graded.Good EVI 6-10,Moderate EVI 11-15 & Poor EVI greater than 15.Systemic side effects were documented.Refractive error was converted to spherical equivalent for analysis.
Results:Average age was 9.5 years(Range- 5-14 years) follow-up for 10 months.Average mesopic & photopic pupil size was 5mm & 4mm respectively.Average NPA was 9cm.Mean increase in spherical equivalence was 0.18D over 6 months.80% had good score & none with poor EVI.No systemic side effects were recorded.
Conclusion:Ease of Vision is not affected in children due to Atropine 0.01% eyedrops & safe for Indian children with progressive myopia
INTRODUCTION:
Myopia one of the most common ocular disorders in the world and considered to be the leading cause of visual impairment.1 Various prevalence studies have shown a substantial increase in myopia among adolescents and it is now thought to be approaching 10–25% in the west and 60–80% in the east.2 Various surveys in India have found myopia prevalence ranging from 6.9 percent to 19.7 percent 3,4.
At present, the mechanisms involved in the etiology of myopiaare unclear and both environmental and genetic factors have been associated with the onset and progression of myopia.1, 5,6
Atropine eyedrops were first proposed as a treatment of myopia in the 1920s. Since then, there have been numerous studies on this subject. However, evidence from randomized control trials has become available only over the last 2 decades. These trials confirm that atropine eyedrops are effective in the control of myopia in a dose-related manner.7-10
There is however no published literature of the effect and side effects of Atropine Eye Drops used to prevent Myopia Progression in India. A commercial preparation of the concentration shown effective is not available making safety a concern. A study was undertaken to study the safety with reconstituted atropine 0.01% eye drop used daily in children with progressive myopia.
Materials and Methods:
The study was approved by our hospital ethical committee and informed consent was obtained from the parents regarding the off label use of the drug and that a reconstituted preparation was being used.
Reconstitution was done under aseptic precautions and laminar flow by mixing 0.1 ml of Atropine 1% (AtrosulphEyedrops,Entod pharma) into 10 ml of Carboxymethylcellulose Eye Drops 5mg/ml (ExtralubeEyedrops, Microlabs Limited) and the drops to be used within one month of reconstitution.
A prospective study was conducted enrolling 50 children presenting to the paediatric ophthalmology outpatient department between May 2016 to June 2016, between 5 to 15 years with a minimum base line refractive error -2D ( Spherical equivalent) with progressive myopia where progression was defined as documented increase of myopia by 0.75 D or more within a period of 6 months.
Children with any severe congenital or developmental delay or systemic diseases, inability to communicate or undertake a complete ophthalmic exam or with conditions in the eye affecting visual acuity (apart from the refractive error) were excluded.
Enrolled patients underwenta comprehensive eye examination and the following tests ;
- Visual acuity with LogMAR chart
- Contrast sensitivity and Glare test
- Mesopic and photopic pupil size
- Orthoptic evaluation which included
- Near Point Accommodation (NPA)
- Negative Relative Accommodation (NRA)
- Positive Relative Accommodation (PRA)
All these values were taken as baseline values. Refractive error was documented as spherical equivalent.
All the selected children were given reconstituted Atropine 0.01% eye drops to be applied one drop to each eye at night.
The above tests were repeated during each review visits and subjective symptoms of glare to light and photophobia while playing in the sunlight were elicited from the children and graded as score 1(never), 2 (sometimes/ occasional) and 3 (always).
Findings at 1 months, 3 months, 6 months and at final follow up was taken for analysis. An Ease of Vision Index was calculated as details in the table below.
| Parameter | Score 1 | Score 2 | Score 3 |
| Near Vision | N6 | N8 | >N10 |
| Near Point Of Accommodation (NPA) | Difference from baseline by 0-2 cm | Difference from baseline by 2-4 cm | Difference from baseline by >4 cm |
| Pupil size variation
(Mesopic) |
Difference from baseline of pupil size by 0.5-1mm | Difference from baseline of pupil size by 1-1.5 mm | Difference from baseline of pupil size by >1.5 mm |
| Pupil size variation
(Photopic) |
Difference from baseline of pupil size by 0.5-1mm | Difference from baseline of pupil size by 1-1.5 mm | Difference from baseline of pupil size by >1.5mm |
| Glare to Light
|
Never | sometimes/ occasional | Always |
| Photophobia
|
Never | sometimes/ occasional | Always |
A score of 6-10 was considered Good EVI,Moderate EVI 11-15 & Poor EVI greater than 15.
Children and parents were also asked if the Atropine eye drops were acceptable to the child as a long term medication and if it interfered with their daily tasks resulting in discontinuation.
Any systemic side effects were elicited and documented. 10 eye drop samples were also cultured on blood agar for possible contamination when the eye drop bottle was returned after use.
Results:
Average age was 9.5 years(Range- 5-14 years). The average follow-up was 10 months( Range – 7 mon -12 months) .
Average spherical equivalent was 5.5 D( range– 3-9.5D) with a mean progression of 1.0D (range 0.75D-1.50D).Best corrected visual acuity on presentation and at every follow up was 0.1 LogMAR and near vision in all was N6 equivalent. Intraocular pressure on presentation was 14 mm Hg ( Range 10-16 mm Hg ) and on final follow up 13 mm Hg ( Range 10-15 mm Hg). Slit Lamp examination showed no evidence of any conjunctival congestion or corneal affliction. No systemic side effects were recorded.
Averagemesopic & photopic pupil size recorded on atropine therapy was 5mm & 4mm respectively.
Figure1: Showing the average increase of spherical equivalent (Dioptres) with atropine 0.01%
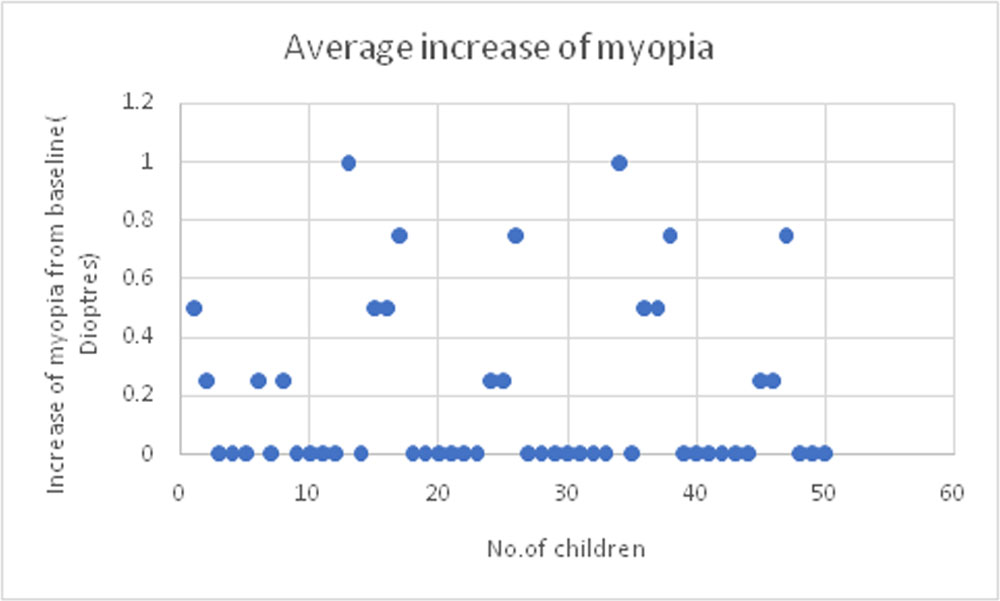
Mean increase in spherical equivalence was 0.18 + 0.29D over 6 months.
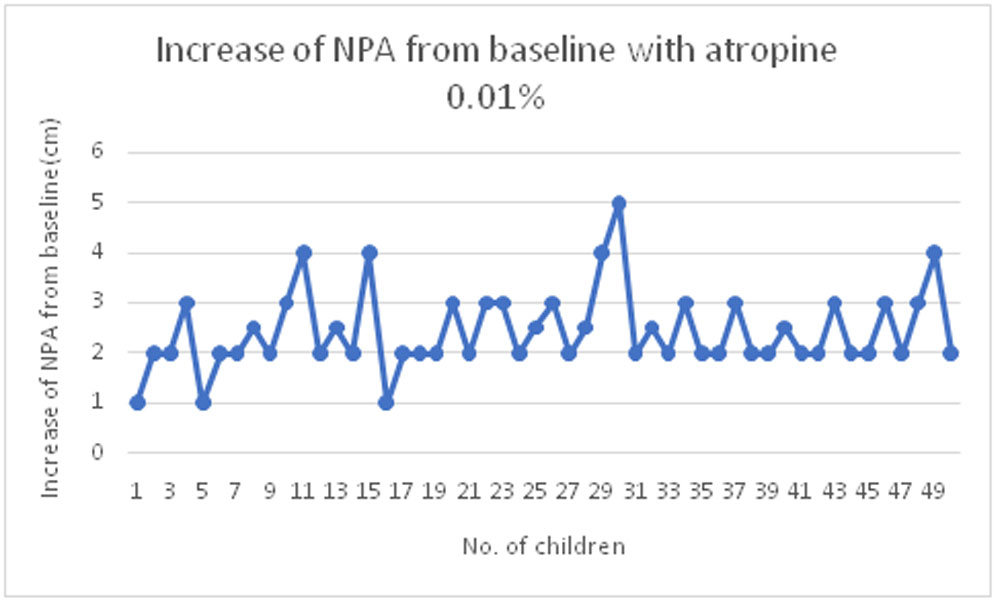
Figure 2: Showing the average increase of NPA (cm) with atropine 0.01%
Average NPA was 9cm while on Atropine 0.01% . Average increase of NPA from baseline was 2.44 + 0.79 cm.
5 children had occasional glare to light and 4 children had occasional photophobia.
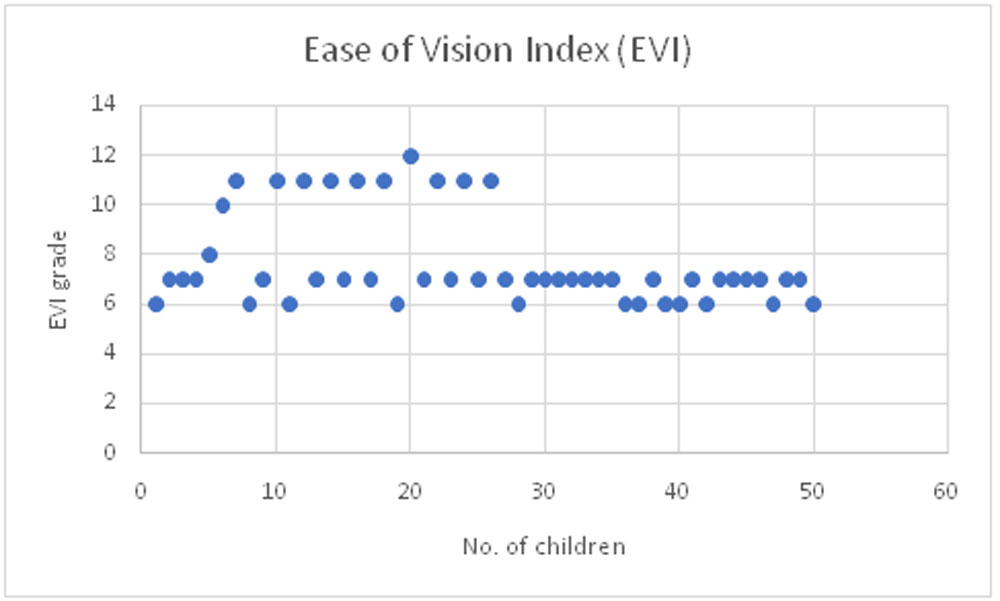
Figure 3: showing the Ease of vision Index(EVI) grading
40 children (80%) had good score of 6-10 & none with poor EVI. The average score found to be 7.5.
All cultures were negative.
Discussion:
In any medication that is used for long period of time, concerns apart from effectiveness of treatment are safety and also ability to tolerate and comply.
Atropine at 1.0%, 0.5% and 0.01% has been demonstrated through randomized trials to be effective in slowing myopia progression.11 However, the safety profile of atropine (systemic side effects and visual disturbances) often has been a source of concern and deterred many from using this medication.
Every unit increase in pupil size results in an exponential increase in the amount of light entering the eye,and this can cause glare and potential phototoxicity. Atropine also decreases accommodation amplitude and near vision so that children may require bifocal or progressive glasses to read.
Atropine 0.01% has been proved to be effective in controlling progression of myopia. But atropine 0.01% is currently not commercially available. If atropine needs to be used as a part of our clinical practice it would need to be reconstituted. Contamination of the eye drops on storage becomes and additional concern apart from those listed above.
Molly Smith et al12 stated that, in order to be considered clinically meaningful, a myopia control modality should slow the progression by approximately 50%. In our patients the progression while the medicines were in use was reduced by 82% indicating efficacy.
Our study collaborated findings of others13-15 in the absence of any systemic side effects with daily use over a period of 11 months. There were no gross vision disturbances affecting their day to day life. There was no contamination of the eye drop at the end of one month.We converted the various parameters to an Ease of Vision Index to try and quantify them for comparison over time. Since our children come from diverse backgrounds a purely subjective Visual function questionnaire did not seem apt. Hence we used the ease of vision index with what we thought were critical parameters.
The limitations of the study being small sample size and shorter follow up.The Ease of Vision Index would need more validation for comparison across other sites and time.
The lowest concentration of 0.01% reconstituted atropine thus seems to retain efficacy in Indian children with darker iris and is a viable concentration for reducing myopia progression in children while being well tolerated and safe from adverse effects with long term usage.
Conclusion:
Reconstituted atropine 1% to 0.01% eye drops can be used in Indian children with progressive myopia. Ease of Vision is not affected in children due to Atropine 0.01% eyedrops & safe for Indian children with progressive myopia.
References:
- World Health Organization. Elimination of Avoidable Visual Disability due to Refractive Errors (WHO/PBL/0079). Geneva: World Health Organization, 2000. Vision 2020
- Saw S-M. A synopsis of the prevalence rates and environmental risk factors for myopia.ClinExpOptom 2003; 86:289–94.
- Jain IS, Jain S, Mohan K. The epidemiology of high myopia—changing trends. Indian J Ophthalmol 1983;31:723-8.
- Mohan M, Pakrasi S, Zutshi R. Myopia in India. ActaOphthalmolSuppl 1988;185:19-23.
- Goss DA, Hampton MJ, Wickham MG. Selected review on genetic factors in myopia. J Am OptomAssoc 1988;59:875-84.
- Donald O. Mutti, Myopia – The Nature Versus Nurture Debate Goes On, Invest Ophthalmol Vis Sci, May 1996, Vol. 37, No. 6
- Yen MY, Liu JH, Kao SC, Shiao CH. Comparison of the effect of atropine and cyclopentolate on myopia. Ann Ophthalmol 1989;21:180–2, 187.
- Shih YF, Chen CH, Chou AC, et al. Effects of different concentrations of atropine on controlling myopia in myopic children. J OculPharmacolTher 1999;15:85–90.
- Shih YF, Hsiao CK, Chen CJ, et al. An intervention trial on efficacy of atropine and multi-focal glasses in controlling myopic progression.ActaOphthalmolScand 2001;79:233–6.
- Chua WH, Balakrishnan V, Chan YH, et al. Atropine for the treatment of childhood myopia. Ophthalmology 2006;113: 2285–91.
- Audrey Chia, Wei-Han Chua, Yin-Bun Cheung, Wan-Ling Wong, Mbiostat, AnushiaLingham Et al. Atropine for the Treatment of Childhood Myopia: Safety and Efficacy of 0.5%, 0.1%, and 0.01% Doses (Atropine for the Treatment of Myopia 2). Ophthalmology 2011.
- Molly J Smith and Jeffrey J .Controlling myopia progression in children and adolescents.WallineAdolesc Health Med Ther.2015; 6: 133–140.Published online 2015 Aug 13.
- .Wu PC, Yang YH, Fang PC. The long-term results of using low concentration atropine eye drops for controlling myopia progression in schoolchildren. J OculPharmacolTher. 2011;27(5):461-6
- . Loughman J, Flitcroft DI. The acceptability and visual impact of 0.01% atropine in a Caucasian population.Br J Ophthalmol. 2016 Nov;100(11):1525-1529.
- Nishiyama Y, Moriyama M, Fukamachi M, Uchida A, Miyaushiro H, Kurata A, Tokoro T, Ohno-Matsui K. Side Effects of Low Dose Atropine.Nippon GankaGakkaiZasshi.2015 Nov;119(11):812-6.
Leave a Comment