
Dr. Ravi Chandra K, K19872, Dr. Rama Krishnan R, Dr. Venugopal V Anitha
Authors :
Ravi Chandra K,Anitha Venugopal,Sowmya Periand Rengappa Ramakrishnan
Purpose:To assess the pattern of intraocular pressure (IOP) changes after Descemet stripping endothelial keratoplasty (DSEK) in a South Indian population.
Methods: A retrospective chart review of patients who underwent DSEK at Aravind Eye Hospital (Tirunelveli, South India) from January 2014 to December 2015 was performed. All the surgeries were performed by a single surgeon. Preoperative data collected included the best corrected visual acuity (BCVA), baseline IOP, indication for graft, prior history of glaucoma, any history of previous glaucoma surgery and any medical therapy used to control glaucoma. Patients with a minimum follow-up of 6 months were included. Postoperatively, duration of follow-up, any graft rejection episodes and antiglaucoma therapy were noted in addition to IOP measurement at each visit and BCVA at the last visit. An IOP elevation of 10 mm Hg from baseline or an absolute IOP of >24 mm Hg at any postoperative visit was considered significant.
Results: Sixty two eyes from 62 patients were included. 15 patients (24.2%) were known cases of glaucoma and 6 of these underwent prior glaucoma surgery. IOP elevation of 10 mm Hg from baseline was seen in 40.3% patients (25/62) regardless of glaucoma status.In known glaucoma patients, 8(8/15, 53.3%) had such an increase in IOP and 17 patients (17/47, 36.2%) with no prior glaucoma had such increment. Absolute IOP of >24mm Hg was observed in 38.7% patients (24/62), with 36.2% of patients without prior glaucoma and 46.7% of patients with prior glaucoma showing such increment. Graft rejection was noted only in 1 patient, whereas primary graft failure was observed in 10 patients, out of which 2 patients required penetrating keratoplasty. About 40% patients required a change in therapy postoperatively, which was more in patients with prior glaucoma.
Conclusion(s): Elevation of IOP was noted in a significant proportion of patients regardless of glaucoma status. Pre-existing glaucoma further increased the risk. Postoperativesteroid response could be the most common cause, owing to the timing of rise of IOP in most of the patients. Close monitoring of IOP and thorough evaluation postoperatively is recommended, particularly in patients with prior glaucoma.
Introduction
The corneal transplantation surgery has seen a shift towards lamellar procedures in recent times,owing to the improvements in graft preparation and technology.Among these, Descemet stripping endothelial keratoplasty (DSEK) has become the preferred treatment for corneal endothelial dysfunction.1 It scores over conventional penetrating keratoplasty(PK)2 due to the avoidance of open-sky procedure, fewer sutures required, and thus less suture-related complications including induced astigmatism, tectonic stability, reduced rates of graft failure from ocular surface disease, and rapid visual recovery.
Glaucoma is a major postoperative complication of any corneal graft surgery.In addition to the risk of irreversible vision loss, preexisting glaucomaand uncontrolled intraocular pressure(IOP) are riskfactors for poor outcome, endothelial cell loss, and subsequentgraft failure after PK.3-6 The incidence of glaucoma after PK rangedfrom 9% to 31% in the early postoperative period7,8 and from18% to 35% in the late postoperative period.9,10 A higher incidence of elevatedIOP, ranging from 29% to 80%, was found after PK in caseswith preexisting glaucoma.11Preexisting glaucoma and poorly controlled postoperative IOP are considered to be major risk factors contributing to graft failure in PK.10
With regard to DSEK, IOP fluctuations postoperatively are expected to be less affected as the structural integrity of the cornea is relatively preserved.Few studies found lesser IOP changes post DSEK when compared with PK.12,13 A substantial incidence of IOP elevation was reported by some studies,14,15 especially in the presence of prior glaucoma or ocular hypertension.16 Limited data is available about direct comparison between the two procedures,with one study17 concluding that DSEK had lesser IOP elevation postoperatively compared with PK,while another study18 found that DSEK has an equivalent incidence of IOP elevation to PK in comparable patients.
In our study we conducted a retrospective chart review to characterize the pattern of IOP changes and visual outcomes after DSEK in patients with or without pre-existing glaucoma.
Materials and methods
A retrospective chart review of 62 DSEK cases, performed by a single surgeon from January 2014 to December 2015 was performed. All DSEK surgeries and preoperative evaluations were performed at Aravind Eye Hospital, Tirunelveli, South India, a tertiary referral center for cornea and refractive surgery.
Inclusion criteria were defined to include all patients who underwent DSEK as the primary corneal transplantation procedure. Only one eye of each subject was included. Preoperative data collected included the indication for graft, prior history of glaucoma, any history of previous glaucoma surgery and any medical therapy used to control glaucoma. Patients with a minimum of 6 months follow-up were included. The exclusion criteria comprised of any indication for which PK was the preferred procedure or any history of previous corneal transplantation.
Surgical Technique
All the surgeries were performed by a single surgeon. The technique of performing DSEK was similar to that described previously in the literature.19 All the surgeries utilized 7.5 to 8 mm donor lenticule, 5 to 6 mm temporal sclerocorneal tunnel, descemet membrane rhexis, donor lenticule push-in, air injection into the anterior chamber (AC) for 10 minutes and later 30-40% of the AC air bubble replacement with balanced salt solution. Postoperatively, patient is instructed to maintain a supine position for at least 4 to 6 hours and started on steroid and antibiotic combination eyedrops (Dexamethasone and Moxifloxacin) 8 times per day, along with an antibiotic and a cycloplegic(atropine).The drops were tapered slowly(at a rate of once a week) depending on the clinical status of the transplant to once daily dosing over a period of 4 months. If a steroid-induced elevation in IOP was suspected, the drops were changed to a less potent steroid preparation such as fluorometholone. If the IOP was not controlled, steroid drops were discontinued. If graft rejection episode occured, drops were again escalated according to clinical response.
Preoperative and postoperative Evaluation
All patients were subjected to a comprehensive preoperative evaluation. Visual acuity (VA) was measured with a Snellen VA chart. The best-corrected visual acuity (BCVA) at each visit was included. Clinical specular microscopy (Topcon, SP 3000P, Japan) was performed preoperatively for endothelial cell density. IOP was measured with a Goldmann tonometer (Hagg-Streit, Konig, Switzerland) in all patients. If the view of the fundus was adequate, fundus examination was performed and the cup-to-disc ratio (C/D) of the optic nerve was documented.
Primary outcome measure was IOP postoperatively at 1 week, 1 month, 3 months 6 months, and the last visit to the hospital. Secondary outcome measures included BCVA, any graft failure, use of antiglaucomatous medications, and subsequent glaucoma surgery or regraft surgery.
Definition of Preexisting Glaucoma and Postoperative Elevated Intraocular Pressure
A patient was considered to have preexisting glaucoma if any of the following features are fulfilled: documented history of glaucoma, prior glaucoma filtration surgery, preoperative use of antiglaucomatous medications, preoperative IOP ≥24 mmHg, or C/D ≥0.6. For cases with hazy view of the fundus at preoperative evaluation, C/D on the subsequent examination was used. Patients with a history of narrow angle or laser iridotomy were not classified with preexisting glaucoma unless they meet the other criteria.
Anpostoperative IOP <21mm Hg was considered as normal IOP. An IOP elevation of 10 mm Hg from baseline or an absolute IOP of >24 mm Hg was considered significant.At any visit, a single IOP measurement that met the above criteria would be classified as postoperative IOP elevation.
An addition of a new antiglaucoma agent or changing of one agent to another, or the addition of another agent to existing agents, for control of IOP was considered as a change in medical therapy. It did not include a reduction in number of agents.
Statistical Analysis
The data were entered into a Microsoft Excel 2011 spreadsheet (Microsoft Corp, Redmond, WA, USA). The data were analyzed using statistical software (STATA 11.1,Texas, USA).Ap-value of <0.05 was considered statistically significant. Mean ± standard deviation (SD) and frequency (percentage) were used to describe the summary data. Paired t test & Wilcoxon signed rank test were used to compare the mean differences between preoperative and final postoperative visit. Mann Whitney test was used to compare the mean differences between patients with prior glaucoma and without prior glaucoma.
Results
On the basis of the inclusion and exclusion criteria, 62 eyes from 62 patients qualified for the study. The demographic data and baseline characteristics are summarized in Table 1. 12 patients(19%)had concurrent intraocular lens implantation, out of which 6 were iris claw lenses and 1 was a scleral fixated intraocular lens. 15 patients(24%) had a prior history of glaucoma with 6 patients(6/15,40%) having undergone prior glaucoma surgical intervention(3-trabeculectomy, 2-aqueous drainage devices and 1-trabeculotomy+trabeculectomy). Graft rejection was noted only in 1 patient, whereas primary graft failure was observed in 10 patients within the follow-up period,out of which 2 patients required penetrating keratoplasty.Rebubbling with C3F8 was required in 2 cases and re-DSEK in 1 patient. 1 patient each underwent trabecuectomy and drainage device implantation respectively in the follow-up period.
The mean IOP (with SD) values over time are expressed in Figure 1 and Table 2.The mean preoperative IOP was 14.37(3.0) mm Hg and the mean IOP at last visit was 16.19(3.7) mm Hg and thus over the follow-up period, the mean IOProse by 1.82 mmHg(p=0.0005). In patients without prior glaucoma, the mean IOP rose by 1.68 mmHg over the follow-up period(p=0.0050), whereas it rose by 2.27 mm Hg in patients with prior glaucoma (p= 0.0064), (Figure 2). The average number of antiglaucoma medications per patient is presented in Table 3.Theaverage number of antiglaucoma medications per patient preoperatively was 0.21, while at last visit it was 0.87 (p= <0.001).A total of 25 patients (40.3%) required a change in antiglaucoma medications. In patients without prior glaucoma(n=47), 36.17 % patients(17/47) required a change in therapy to control IOP. If there was prior glaucoma (n=15), 53.3 % of patients(8/15) required a change in therapy.
An elevation of IOP of 10 mm Hg from baseline was seen in 40.3% patients(25/62) regardless of glaucoma status. In known glaucoma patients, 8 (8/15,53.3%) had such an increase in IOP and 17 patients (17/47,36.2%) with no prior glaucoma had such increment.An absolute IOP of >24mm Hg during at-least one postoperative visit was observed in 38.7% patients(24/62) and this was seen in 7 (7/15,46.7%) patients with known glaucoma and 17 (17/47,36.2%) patients without prior glaucoma. The elevation of IOP was noted at 1 month postoperative visit in 17 patients(17/25,68%).Figure 3 shows the percentage of eyes without pre-existing glaucoma that remained free of IOP elevation as defined by the study criteria (elevation of IOP of 10 mm Hg from baselineor an absolute IOP of >24 mm Hg) as a function of time after DSEK. At the end of the study, the survival probability was 62%.
The preoperative BCVA and their postoperative outcomes are represented in Table 4. The mean preoperative BCVA (LogMAR) (with SD) was 1.55(0.5) (Snellen equivalent 2/60, range 6/36 – Perception of light) and at the last postoperative visit was 1.00(0.7) (Snellen equivalent 6/60, range 6/6 – Hand motion) (p<0.001). In patients without preexisting glaucoma, it was 1.55(0.5) (Snellen equivalent 2/60, range 6/36 – Perception of light) preoperatively and 0.93(0.6) (Snellen equivalent 6/60, range 6/6 – Hand motion) (p<0.001) at the last postoperative visit. In patients with preexisting glaucoma, it was 1.53(0.4) (Snellen equivalent 2/60, range 6/36 – Hand motion) preoperatively and 1.22(0.7) (Snellen equivalent 4/60, range 6/9 – Hand motion) (p=0.046) at the last postoperative visit.
Discussion
Elevated IOP after corneal transplant surgery is a serious postoperative complication that may endanger the survival of the graft and long term visual potential. In this retrospective review of 62 DSEK cases, we found a high percentage of postoperative elevated IOP in eyes with and without preexisting glaucoma. 2 patients had to undergo further glaucoma surgical intervention in the follow-up period.In terms of visual outcome, all the patients had a statistically significant visual improvement at the last postoperative visit, irrespective of the glaucoma status.
Glaucoma post corneal transpantation is usually defined on the basis of elevated IOP, with or without associated visual field loss or optic nerve changes asthe structural and functional changes are difficult to assess both pre and postoperatively.Few studies reported a significant IOP elevation 14,15 following DSEK, especially in the presence of prior glaucoma or ocular hypertension.16Our study found an incidence of raised IOP in about 39 to 40% patients overall, and a significantly higher percentage in patients with preexisting glaucoma. In our study, 27% of patients without prior glaucoma and 53% of patients with prior glaucoma required a change in therapy to control IOP. Sandhu S et al.18 reported similar patterns of IOP elevation and need for change in therapy post DSEK.
There can be multiple causes for elevation of IOP post DSEK, which include steroid induced ocular hypertension, inflammation, graft rejection, peripheral anterior synechiae formation with chronic angle closure and air bubble induced (either due to trabecular meshwork damage intraoperatively, or immediate postoperative air bubble pupillary block). Progression of pre-existing glaucoma is also a cause for postoperative IOP elevation.Vajaranant et al.13 elaborated the role of steroid response in detail and opined that steroid response is likely the major cause of postoperative IOP elevation after DSEK. The reasons could be minimal postoperative angle distortion as DSEK is performed with a small incision and often without suturing, lesser incidence of inflammation and graft rejection after DSEK when compared to PK and the fact that the frequency and peak IOP in all patients mimic what would be expected in steroid-related ocular hypertension. In our study,we found about 68% of patients with elevated IOP had their spike 1 month postoperatively, which could most probably be explained by a steroid response. The incidence of initial graft rejection episodes in the first 2 years was 7.5% in endothelial keratoplasty cases (deep lamellar endothelial keratoplasty and DSEK) and 13% in a PK comparator group.20Vajaranant et al.13suggested that the risk of elevated IOP increases with duration of topical steroid use, whereas other studies suggest that prolonged topical steroid use may significantly reduce the risk of graft rejection.20,21 The risk of graft rejection was 2-fold higher in DSEK eyes13 that experienced steroid-related ocular hypertension, compared with DSEK eyes that did not experience IOP elevation.22 In our study, we observed only 1 case of graft rejection.Yi et al23 found that patients with preexisting glaucoma are much more likely to develop a steroid response after DSEK as compared with normal individuals. In view of lower rates of graft rejection in DSEK2, an earlier tapering of steroids could be advocated leading to a lower risk of steroid induced glaucomatous optic nerve damage24,however further research is awaited.
The other two mechanisms that may influence postoperative IOP could be graft dislocation and pupillary block. Graft dislocation is more common in DSEK than in PK and can contribute to angle distortion postoperatively.10 Any damage to the graft or poor posterior donor-recipient adherence can lead to earlier graft failure or increased primary graft failures.24 In our study, 2 patients required rebubbling with C3F8 and 1 patient required re-DSEK, however all 3 patients maintained good IOP control. Pupillary block due to air bubble, although transient can cause an acute trabecular injury and in addition to corticosteroid use, can contribute to the long-term progression toward glaucoma.25 Air migration posterior to the iris can also cause papillary block and IOP elevation.26 Retaining less air less air within the anterior chamber could be helpful to avoid this complication.27 In our study, we did not observe any postoperative pupillary block.
The IOP measurements in our study were done by Goldmann Applanation Tonometer (GAT). The measurements thus could possibly be affected by high values of IOP,central corneal thickness(CCT) (thick or thin corneas) and age.28,29 Previous studies have reported an increased CCT postoperatively following DSEK.30 Such a condition can mask the true IOP readings measured by GAT.31.32 Vajaranant et al15 concluded that the increased CCT did not falsely elevate the IOP post-DSEK when measured by GAT. These findings were supported by studies done by Yi et al23 and Clemmensen and Hjortdal.33
Previous studies found that preexisting glaucoma and elevated IOP are associated with poor outcome and graft failure after PK.3-6In our study, patients with and without preexisting glaucoma had a similar mean BCVA at baseline. Although patients with glaucoma had a slightly lower mean BCVA at the last postoperative visit, all the patients had a statistically significant visual improvement at the last postoperative visit,irrespective of the glaucoma status.
There are certain limitations in our study. First, the retrospective nature of the study. Second,the broad criteria used to define preexisting glaucoma(IOP ≥24 mmHg, or C/D ≥0.6),as a result of which patients with ocular hypertension or glaucoma suspect could also have be included. In addition, gonioscopy, visual field testing, and optic nerve analysis were not reviewed in the present study.Third, in patients with corneal pathology and post any transplantation technique,corneal structure is altered and there are reports of increased corneal thickness following DSEK. In addition, the preoperative IOP measurements could have been falsely high as they may have been performed on edematous corneas. Strengths of our study include the inclusion of wide range of corneal pathologies and also that all the surgeries were performed by a single surgeon.
Conclusions
Elevation of IOP following DSEK is a very common complicationthat needs to be addressed.Elevated IOP post DSEK was noted in about 40% patients, regardless of glaucoma status and it was more common in patients with prior glaucoma. Pre-existing glaucoma increased the risk of developing IOP elevation and post-DSEK glaucoma.Although there can be a number of causes of postoperative IOP elevation,postoperativesteroid response could be the most common cause, owing to the timing of rise of IOP in most of the cases.Inview of low incidence of graft rejection post DSEK in our study and also in previous studies, an earlier tapering of steroids could be advocated, howeverfurther prospective controlled studies are required in this regard.Asthe incidence of postoperative IOP elevation is high, close monitoring of IOP and thorough glaucoma evaluation including visual field examination and optic nerve analysis after clearance of corneal edema is recommended, particularly in patients with previous history of glaucoma and persistent IOP elevation.
References
- Price MO, Price FW. Descemet’s stripping endothelial keratoplasty. Curr Opin Ophthalmol. 2007;18:290–294.
- Lee WB, Jacobs DS, Musch DC, et al. Descemet’s stripping endothelial keratoplasty: safety and outcomes: a report by the American Academy of Ophthalmology. Ophthalmology. 2009;116:1818–1830.
- Price MO, Thompson RW Jr, Price FW Jr. Risk factors for various causes of failure in initial corneal grafts. Arch Ophthalmol 2003;121:1087–92.
- Irvine AR, Kaufman HE. Intraocular pressure following penetrating keratoplasty. Am J Ophthalmol 1969;68:835– 44.
- Ayyala RS. Penetrating keratoplasty and glaucoma. Surv Ophthalmol 2000;45:91–105.
- Seitz B, Langenbucher A, Nguyen NX, et al. Long-term follow-up of intraocular pressure after penetrating keratoplasty for keratoconus and Fuchs’ dystrophy: comparison of mechanical and excimer laser trephination. Cornea 2002;21: 368–73.
- Goldberg DB, Schanzlin DJ, Brown SI. Incidence of increased intraocular pressure after keratoplasty. Am J Ophthalmol.1981;92:372–377.
- Chien AM, Schmidt CM, Cohen EJ, et al. Glaucoma in the immediate postoperative period after penetrating keratoplasty.Am J Ophthalmol. 1993;115:711–714.
- Foulks GN. Glaucoma associated with penetrating keratoplasty. 1987;94:871–874.
- Huber KK, Maier AK, Klamann MK, et al. Glaucoma in penetrating keratoplasty: risk factors, management and outcome.Graefes Arch Clin Exp Ophthalmol. 2013;251:105–116.
- Banitt M, Lee RK. Management of patients with combined glaucoma and corneal transplant surgery. 2009;23:1972–1979.
- Espana EM, Robertson ZM, Huang B. Intraocular pressure changes following Descemet’s stripping with endothelial keratoplasty. Graefes Arch Clin Exp Ophthalmol. 2010;248:237–242.
- Vajaranant TS, Price MO, Price FW, et al. Visual acuity and intraocular pressure after Descemet’s stripping endothelial keratoplasty in eyes with and without preexisting glaucoma. 2009;116:1644–1650.
- Maier AK, Klamann MK, Torun N, et al. Intraocular pressure elevation and post-DSEK glaucoma after Descemet’s stripping endothelial keratoplasty. Graefes Arch Clin Exp Ophthalmol.2013;251:1191–1198.
- Vajaranant TS, Price MO, Price FW, et al. Intraocular pressure measurements following Descemet stripping endothelial keratoplasty. Am J Ophthalmol. 2008;145:780–786.
- AllenMB, Lieu P, Mootha VV, et al. Risk factors for intraocular pressure elevation after descemet stripping automated endothelial keratoplasty. Eye Contact Lens. 2010;36:223–227.
- Moisseiev E, Varssano D, Rosenfeld E, et al. Intraocular pressure after penetrating keratoplasty and Descemet’s stripping automated endothelial keratoplasty. Can J Ophthalmol.2013;48:179–185.
- Sandhu S,Petsoglou C, Grigg J, Veillard AS. Elevated intraocular pressure in patients undergoing penetrating keratoplasty and Descemet stripping endothelial keratoplasty. J Glaucoma 2016;25:390-396.
- Basak SK. Descemet stripping and endothelial keratoplasty in endothelial dysfunctions: Three-month results in 75 eyes. Indian J Ophthalmol 2008;56:291-6
- Allan BD, Terry MA, Price FW Jr, et al. Corneal transplant rejection rate and severity after endothelial keratoplasty. Cornea 2007;26:1039–42.
- Nguyen NX, Seitz B, Martus P, et al. Long-term topical steroid treatment improves graft survival following normal-risk penetrating keratoplasty. Am J Ophthalmol 2007;144:318–9.
- Price MO, Jordan CS, Moore G, Price FW Jr. Graft rejection episodes after Descemet stripping with endothelial keratoplasty: part two: the statistical analysis of probability and risk factors.Br J Ophthalmol 2009;93:391–5.
- Yi K, Bae G, Kong M, et al. Intraocular pressure measured with Goldmann, noncontact, Schiotz, and dynamic contour tonometry after DSEK. 2013;32:1089–1093.
- Jordan CS, Price MO, Trespalacios R, et al. Graft rejection episodes after Descemet stripping with endothelial keratoplasty: part one: clinical signs and symptoms. Br J Ophthalmol.2009;93:387–390.
- Price FW Jr, Price MO. Descemet’s stripping with endothelial keratoplasty in 200 eyes: early challenges and techniques to enhance donor adherence. J Catarct Refract Surg. 2006;32:411–418.
- Lee JS, Desai NR, Schmidt GW, et al. Secondary angle closure caused by air migrating behind the pupil in descemet stripping endothelial keratoplasty. 2009;28:652–656.
- Price MO, Price FW Jr. Descemet stripping with endothelial keratoplasty for treatment of iridocorneal endothelial syndrome. 2007;26:493–497.
- Iester M, Mermoud A, Achache F, et al. New Tonopen XL: comparison with the Goldmann tonometer. 2001;15(pt 1):52–58.
- Kim NR, Kim CY, Kim H, et al. Comparison of goldmann applanation tonometer, noncontact tonometer, and TonoPen XL for intraocular pressure measurement in different types of glaucomatous, ocular hypertensive, and normal eyes. Curr Eye Res. 2011;36:295–300.
- Ahmed KA, McLaren JW, Baratz KH, et al. Host and graft thickness after Descemet stripping endothelial keratoplasty for Fuchs endothelial dystrophy. Am J Ophthalmol. 2010;150:490 – 497.
- Kotecha A, White E, Schlottmann PG, et al. Intraocular pressure measurement precision with the Goldmann applanation, dynamic contour, and ocular response analyzer tonometers. 2010;117:730–737.
- Harada Y, Hirose N, Kubota T, et al. The influence of central corneal thickness and corneal curvature radius on the intraocular pressure as measured by different tonometers: noncontact and goldmann applanation tonometers. J Glaucoma.2008;17:619–625.
- Clemmensen K, Hjortdal J. Intraocular pressure and corneal biomechanics in Fuchs’ endothelial dystrophy and after posterior lamellar keratoplasty. Acta Ophthalmol. 2014;92:350–354.
TABLE 1. Summary of Demographics and Baseline Characteristics
| Age (years)
Mean age (±SD) 64.94 (±11.6) Range 21 – 83
Sex, n(%) Male 34(54.8) Female 28 (45.2)
Indications for DSEK, n(%) Pseudophakic bullous keratopathy 36 (58) Aphakic bullous keratopathy 6 (10) Fuchs endothelial dystrophy 6 (10) Iridocorneal Endothelial syndrome 2 (3) Scarred DM/ DM injury10 (16) PXF syndrome 2 (3)
History of glaucoma, n(%) 15 (24)
History of prior glaucoma-related 6/15 (40) surgery (% of subgroup)
Preoperative IOP 14.37 (3.0) (mm Hg) mean (SD)
Cup-to-disc ratio(mean) 0.49
BCVA (mean) 1.55, 2/60 (LogMAR, Snellen equivalent) |
SD indicates standard deviation;DSEK,Descemet stripping endothelial keratoplasty; DM, descemet’s membrane; PXF, pseudoexfoliation; IOP,intraocular pressure; BCVA, best corrected visual acuity
TABLE 2. Average IOP ± SD at various timepoints preoperatively and postoperatively in all Patients who underwent DSEK (n = 62)
| Visit | Overall (n=62) | History of Glaucoma | ||||
| No (n=47) | Yes (n=15) | |||||
| Mean(SD) | Range | Mean(SD) | Range | Mean(SD) | Range | |
| Preop | 14.37(3.0) | 8 – 28 | 14.51(2.0) | 10 – 19 | 13.93(5.1) | 8 – 28 |
| Week 1 | 15.97(5.6) | 8 – 47 | 15.87(5.5) | 9 – 47 | 16.27(6.2) | 8 – 26 |
| Month 1 | 16.98(6.5) | 9 – 48 | 16.85(6.6) | 10 – 48 | 17.40(6.5) | 9 – 32 |
| Month 3 | 15.27(3.7) | 10 – 30 | 15.13(3.5) | 11 – 30 | 15.73(4.4) | 10 – 23 |
| Month 6 | 16.58(5.1) | 11 – 36 | 16.51(5.4) | 11 – 36 | 16.80(4.3) | 11 – 24 |
| Final | 16.19(3.7) | 10 – 28 | 16.19(3.9) | 10 – 28 | 16.20(3.2) | 11 – 22 |
| p-value* | 0.0005 | 0.0050 | 0.0640 | |||
*Wilcoxon signed rank test (comparing final visit with Preop)
IOP indicates intraocular pressure; SD, standard deviation;DSEK,Descemet stripping endothelial keratoplasty.
TABLE 3. Average number of Antiglaucoma medications per patient at each timepoint preoperatively and postoperatively
| Visit | Overall (n=62) | History of Glaucoma | ||||
| No (n=47) | Yes (n=15) | |||||
| Mean(SD) | Range | Mean(SD) | Range | Mean(SD) | Range | |
| Preop | 0.21(0.5) | 0 – 2 | 0.06(0.2) | 0 – 1 | 0.67(0.7) | 0 – 2 |
| Week 1 | 0.40(0.7) | 0 – 2 | 0.28(0.6) | 0 – 2 | 0.80(0.7) | 0 – 2 |
| Month 1 | 0.68(0.9) | 0 – 4 | 0.51(0.9) | 0 – 4 | 1.20(0.7) | 0 – 3 |
| Month 3 | 0.74(0.9) | 0 – 4 | 0.55(0.9) | 0 – 4 | 1.33(0.8) | 0 – 3 |
| Month 6 | 0.82(0.9) | 0 – 3 | 0.64(0.9) | 0 – 3 | 1.40(0.8) | 0 – 3 |
| Final | 0.87(1.0) | 0 – 3 | 0.66(0.9) | 0 – 3 | 1.53(0.8) | 0 – 3 |
| p-value# | <0.001 | <0.001 | 0.004 | |||
#paired t test (comparing final visit with Preop)
SD indicates standard deviation;
TABLE 4. Preoperative BCVA (LogMAR) and their postoperative outcomes
| Visit | Overall (n=62) | History of Glaucoma | p-value** | ||||
| No (n=47) | Yes (n=15) | ||||||
| Mean(SD) | Range | Mean(SD) | Range | Mean(SD) | Range | ||
| Preop | 1.55(0.5) | 6/36 – PL | 1.55(0.5) | 6/36 – PL | 1.53(0.4) | 6/36 – HM | – |
| Final | 1.00(0.7) | 6/6 – HM | 0.93(0.6) | 6/6 – HM | 1.22(0.7) | 6/9 – HM | 0.139 |
| p-value* | <0.001 | <0.001 | 0.046 | ||||
*Wilcoxon signed rank test (comparing final visit with Preop) **Mann Whitney test (comparing every visit between groups)
BCVA indicates best corrected visual acuity; SD,standard deviation; PL, perception of light, CF , counting fingers; HM , hand motion;
Mean BCVA represented in LogMAR scale and range represented in Snellen equivalent.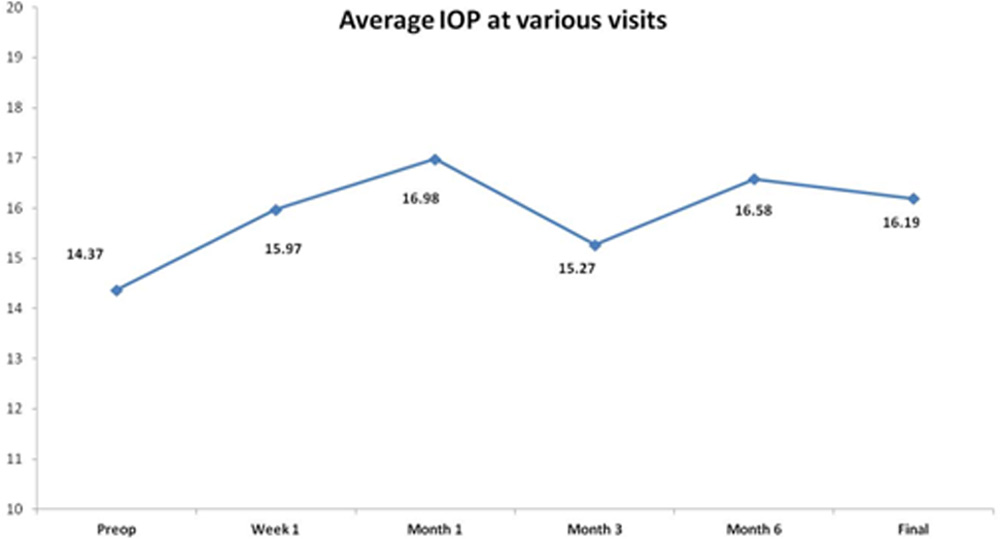
Figure 1.Average intraocular pressure over time in study population.
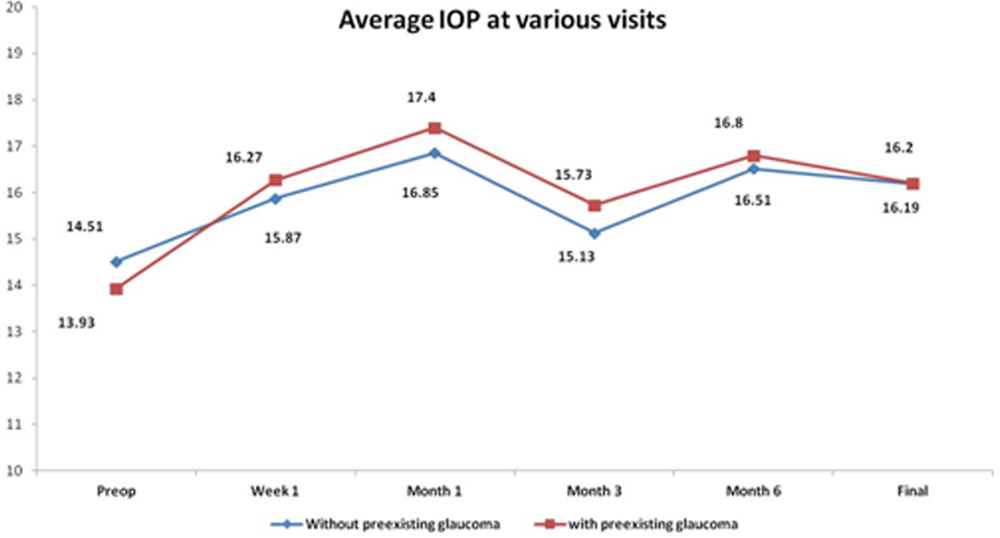
Figure 2. Average intraocular pressure over time in patients with and without pre-existing glaucoma. 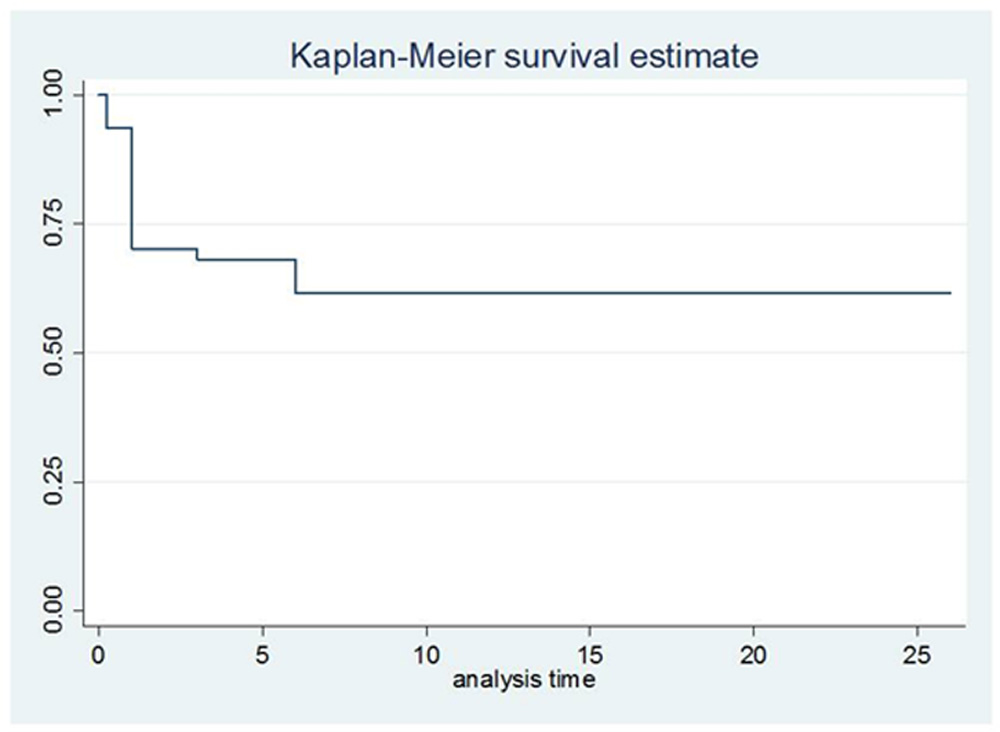
Figure 3. Kaplan–Meier plot showing the percentage of DSEK patients without preexisting glaucoma that did not experience elevated IOP as a function of time after grafting. DSEK indicates Descemet’s stripping endothelial keratoplasty; IOP, intraocular pressure.
Leave a Comment