
Dr. Tuhin Chowdhury, C07211, Dr. Nibedita Das, Dr. Aditya Pradhan
Introduction
Thermal burns of the anterior segment destroy the blood vessels of the sclera and limbus, which can lead to sclerocorneal ischemia and extensive necrosis. Moreover, the release of toxic substances from necrotic cells can further worsen sclerocorneal ulceration or rapidly melt the anterior segment. Ultimately, the globe may be perforated and eyeball integrity lost. Although amniotic membrane is often used to cover a sclerocorneal melt, it remains in place temporarily.
Tenonplasty is a well-established technique for the repair of ocular burns. It covers the ischemic sclera with healthy vascularized tissue from the depth of the orbit and reconstructs the conjunctival matrix of the globe, up to the limbus. It can also ensure initial stabilization of eyes with thermal injuries. Reestablishment of the conjunctival surface through tenonplasty can be very effective in treating sclerocorneal ulceration and melting, because tenonplasty offers a bridge for migration of conjunctival or limbus cells.
Purpose
To analyze the outcomes (anatomical and functional) of tenonplasty in serious ocular thermal injuries (Grade 3 to 6 Dua’s Classification) associated with scleral or sclerocorneal ischemia
Patients and Methods
The records of 8 patients who underwent tenonplasty for thermal injuries by molten metal were analyzed retrospectively.
The time of intervention following injury, need of any revision surgery, time for completeepithelialization, any other procedures for surface reconstruction and visual rehabilitation were analyzed
Surgical Techniques
General anesthesia was used in 1 case with a bilateral involvement, rest all cases surgery done under peribulbar anesthesia. Two traction sutures made of 7-0 doubled armed polyglactin were placed 2– 3 mm from the limbus with episcleral bites; the eye was rotated to allow adequate exposure. Sharp Westcott scissors were used to release the healthy conjunctiva along the border of the scleral ischemia/melt and to create relaxing incisions radially from the edge of the scleral melt toward the healthy fornix, allowing subsequent isolation of the Tenon capsule.
Cryopreserved amniotic membrane transplantation (AMT) done over the melt area by using fibrin glue and then Tenon’s capsule is stretched to cover the ischemic area using 7-0 polygalactin suture. A second AMT is placed and aconformer should be placed.
Post-operatively, topical Steroids in tapering dose along with antibiotics and lubricants given.
Results
7 eyes were unilateral and 1 eye had bilateral thermal injuries and all were male (mean age-30.6 years).The mean time of presentation following injury was 5.4 days. Tenonplasty with AMT was performed as the primary surgery. Revision tenonplasty was required in 2 eyes. Mean time for complete epithelialization of the ocular surface was 48.4 days. Evisceration was performed in one eye for large non healing corneal ulcer with near total scleral melt in a patient with bilateral injury. The other eye of this patient underwent further free oral mucosal autograft. Promising results were found in rest of the cases.
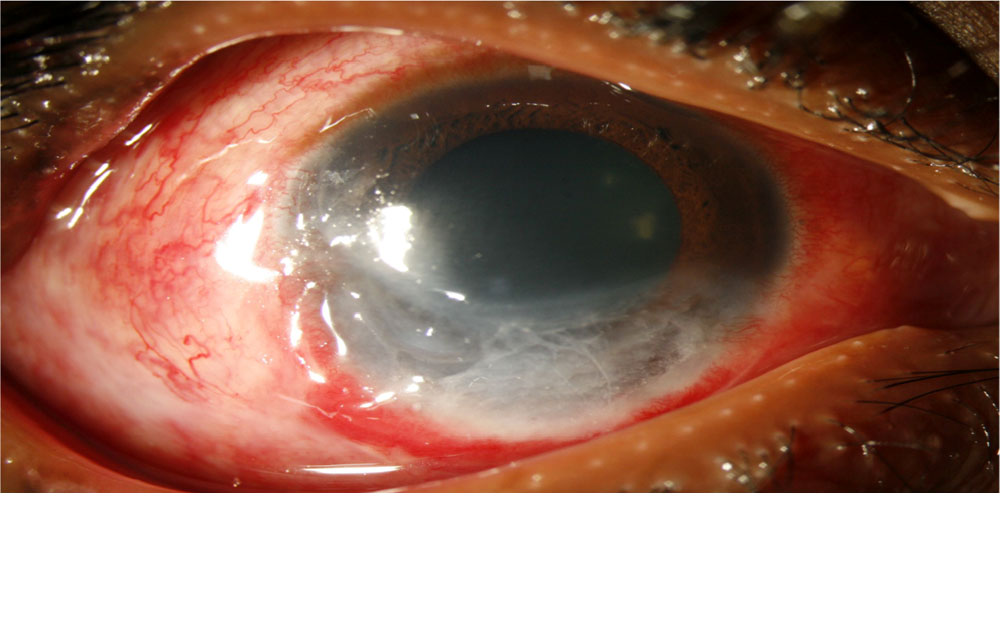
PRE OP
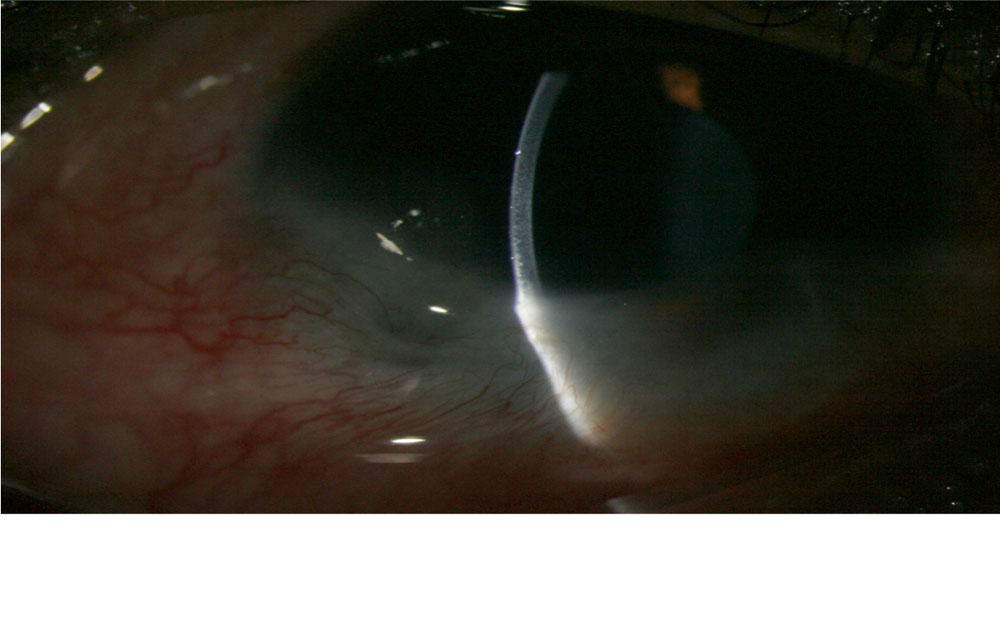
POST OP
Discussion
The aim in acute thermal injury is to debride all necrotic material, improve vascularity in areas of ischemia to facilitate healing, and aid epithelization as well as control inflammation with amniotic membrane. It is equally important to address issues related to exposure and intraocular pressure and sometimes we have to do tarsorrhaphy
Much emphasis has been placed on the use of amniotic membrane in the acute stage. It definitely has a role to play, but will be of benefit only if the ischemia is addressed by tenonplasty. Tenonplasty provides a vascular pedicle over which residual conjunctival cells if any, from the fornix, migrate and help in epithelization
Tenonplasty with AMT should be done together in almost all cases, and the need to use limbal allograft or mucus membrane grafting to be decided as per epithelization. In eyes where we did not use either, the source for the cells was probably from the palpebral conjunctiva or residual cells in the fornix.
A hooding-like procedure by advancing and suturing the Tenon’s flap covering the cornea can be performed in cases of non-epithelization or early corneal melts with a hope to maintain the globe integrity.
Conclusions:
In eyes with serious thermal burn, it is important to address scleral
or sclerocorneal ischemia and accelerate re-epithelialization by tenonplasty.Sometimes one may have to repeat the procedure or go for limbal
stem cell transplantation or oral mucous membrane grafting.When the globe integrity is saved and ocular surface is stable, one can plan further surgeries for better visual rehabilitation.
Leave a Comment