
Dr. Mahesh G, M09321, Dr. Prashant Jain
Abstract
Diabetic Chorioretinopathy (DCR) – Is there such an entity?
Purpose
To evaluate the findings of Diabetic retinopathy cases with large serous macular detachment by multimodal imaging. Study tries to understand whether this is two different conditions i.e. Diabetic Macular edema with superadded central serous Chorioretinopathy associated together or a new entity.
Methods
Retrospective consecutive case series of 17 patients. All patients underwent multimodal imaging including FFA, Spectral OCT, fundus autofluorescence and EDI. FFA showing CSCR like RPE leaks and/or fundus autofluorescence showing Hyperautofluorescent patches were included. Cases with hazy media obscuring the interpretation of FFA and FAF were excluded.
Results
18 eyes of 17 patients, including 14 males with a mean diabetes mellitus of 15.4 years were analyzed. Mean Subfoveal fluid height in OCT was 216.5 microns. 33.3 % had double layer sign and mean Subfoveal choroidal thickness was 312 microns. 66% had pachyvessels in EDI. 16 eyes had Hyperautofluorescent patches in autofluorescence test. 88.8% had NPDR. 77.7% had RPE smoke stack leaks other than diabetic changes. Focal laser to the leak alone resulted in resolution of fluid in most of the cases. Younger age of onset of diabetes with long duration and presence of hypertension appears to be associated with this condition
Conclusion
FFA and Fundus autofluorescence confirm CSCR like picture in some diabetic retinopathy cases. This could be a new subtype of DME called diabetic Chorioretinopathy (DCR) supported by the EDI and presence of pachyvessels rather than an association of DME with CSCR
Introduction
The primary method for evaluating diabetic retinopathy involves biomicroscopy and indirect ophthalmoscopy. This was the gold standard in managing diabetic macular edema (DME) in the past with the criteria of clinically significant macular edema as indicator for treatment.Various imaging modalities are of significant utility in the screening, evaluation, diagnosis, and treatment of the different presentations of this disease. Many imaging techniques can be useful depending on the manifestation of diabetic retinopathy. Optical coherence tomography is an imaging technique capable of evaluating retinal morphology with microscopic resolution.Since it became commercially available in 1996, it has now become a mainstay in the management of a variety of retinal diseases, particularly in macular diseases. In diabetics, OCT is most useful to measure and quantify macular edema, and in the era of anti-VEGF therapy, it has become the most important imaging tool in managing patients with diabetic macular edema.OCT can determine whether diabetic macular edema is center involving or noncenterinvolving, which has become an important distinction in the era of anti-VEGF therapy.
OCT shows different types of macular edema in diabetic retinopathy, which includes focal, diffuse and mixed. Cystoid, spongiform and serous macular detachment are types of OCT edema along with tractional type. There appears to be a yet undescribed type of edema where there is large serous macular detachment like central serous chorioretinopathy (CSCR). Fluorescein angiography has shown in some of these cases a RPE leak like CSCR along with standard diabetic retinopathy. While evaluating the patient of diabetic retinopathy using multi modal imaging, some of the cases have large serous macular detachment on OCT along with double layer sign and RPE irregularity. There may bepachy vesselswith increased choroidal thickness in EDI mode on SD-OCT. On fundus autofluorescence (FAF) hyper autofluorescence was observed in such cases, which suggests towards the diagnosis of central serous chorioretinopathy along with diabetic retinopathy.
The purpose of this study is to understand whether these are two different conditions i.e. Diabetic macular edema with superadded central serous chorioretinopathy or a new entity which we termed as Diabetic Chorioretinopathy (DCR).FFA and fundus autofluorescence confirm CSCR like picture in some diabetic retinopathy cases. This could be a new subtype of DME called diabetic chorioretinopathy supported by the EDI and presence of pachyvessels rather than an association of DME with CSCR.
Objective:
To study the OCT features of DME with large serous macular detachment and describe a new type of DME based on OCT characteristics
Material and Methods:
This is a single centre retrospective case study which included 18 symptomatic eyes of 17 patients with diabetic retinopathy with large serous macular detachment presented at Department of Vitreo-retina, Giridhar Eye Institute, Kochi, India, between January 2014 and December 2016. All patients received a comprehensive ocular examination including best-corrected visual acuity (BCVA) and dilated fundus examination. Along with clinical examination multimodal imaging including spectral domain optical coherence tomography (SD-OCT) (Spectralis Heidelberg Engineering, Inc. Heidelberg, Germany), Enhanced depth imaging on OCT, Fundus Fluorescein angiography (FFA), and fundus autofluorescence(FAF) imaging (Heidelberg Retina Angiograph 2; Heidelberg Engineering, Heidelberg, Germany) were performed.FFA showing central serous chorioretinopathy like retinal pigment epithelium leaks and/or fundus autofluorescence showing hyperautofluorescent patches were included in the study.Cases with hazy media obscuring the interpretation of FFA and FAF were excluded.
Statistical analysis used was SPSS software version 16.0 (SPSS Inc. Chicago, IL, USA) to compare the logarithm of the minimal angle of resolution visual acuity at presentation and final follow-up. P < 0.05 was considered statistically significant.
Since our study was a retrospective analysis of patient data from the electronic medical records, consent was not obtained. The study was conducted in accordance to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board.
Results:
Out of 17 patients included 14 were males and 3 females with mean age of 53.39±8.40 years (Range 38 to 73 years). Out of 17 patients 8 patients were having hypertension and 4 were having chronic kidney disease with a mean diabetes mellitus of 15.4±7.8 years. The mean follow up period was 16.22 ± 21.27 months (Range 3-72 months).
The mean BCVA at baseline was +0.30 ±0.19 logMAR unit (Mean Snellen’s 20/33) and at final visit mean BCVA was +0.31 ± 0.17 logMAR unit.
On analyzing the SD-OCT features all 18 eyes were having serous macular detachment with mean Subfoveal fluid height in OCT was 216.5 ± 131.75 microns. 33.3% (6 patients) had hyporeflective double layer sign on OCT and mean Subfoveal choroidal thickness was 312 ± 74.86 microns (Table 1). 66%(12 patients) had pachyvessels on EDI. 16 eyes(88.9%) had hyperautofluorescent patches on fundus autofluorescence. On analyzing the FAF of other eyes, hyperautofluorescent patches were seen in 3 eyes.
Table 1: OCT Parameters
| OCT Parameters | Summary Details |
| Sub Retinal Fluid Height | |
| Mean | 216.50 |
| SD | 131.748 |
| Minimum; Maximum | 35; 571 |
| EDI(Fovea) | |
| Mean | 312.0 |
| SD | 74.858 |
| Minimum; Maximum | 228; 477 |
| SMD | |
| Yes | 18 (100) |
| No | – |
| DLS | |
| Yes | 6 (33.3) |
| No | 12 (66.7) |
| Pachyvessels | |
| Yes | 12 (66.7) |
| No | 6 (33.3) |
On analyzing the FFA of 18 eyes, 16 eyes (88.8%) had NPDR. Peripheral ischemia was seen in 6 eyes (33.3%). 14 eyes (77.7%) had RPE smoke stack leaks other than diabetic changes on FFA (Table 2).
Table 2: FFA Parameters
| FFA | Summary Details |
| NPDR/PDR | |
| NPDR | 16 (88.9) |
| PDR | 2 (11.1) |
| PERIPHERAL ISCHEMIA | |
| Yes | 6 (33.3) |
| No | 12 (66.7) |
| LEAK POINT | |
| Yes | 14 (77.8) |
| No | 4 (22.2) |
On analyzing the treatment modality given in study group, focal leak was given to RPE leak in 10 eyes (55.6%) and intravitreal anti-VEGF in 2 eyes (Table 3). In 6 eyes no treatment was given and patient was observed. Focal laser to the leak alone resulted in resolution of fluid in most of the cases (6 out of 10 eyes). Younger age of onset of diabetes with long duration and presence of hypertension appears to be associated with this condition.
Fundus autofluorescence showed Hyperautofluorescent patches like CSCR in 16 cases. This was along the area of large serous macular detachment. 6 cases had RPE tracts that is typical of chronic CSCR.
Table 3: Treatment Details
| Treatment | Summary Details |
| Intravitreal | |
| Yes | 2 (11.1) |
| No | 16 (88.9) |
| Observe | |
| Yes | 6 (33.3) |
| No | 12 (66.7) |
| Focal Laser | |
| Yes | 10 (55.6) |
| No | 8 (44.4) |
On the last follow up there was improvement in the mean visual acuity with reduction of serous macular detachment.
Figure 1
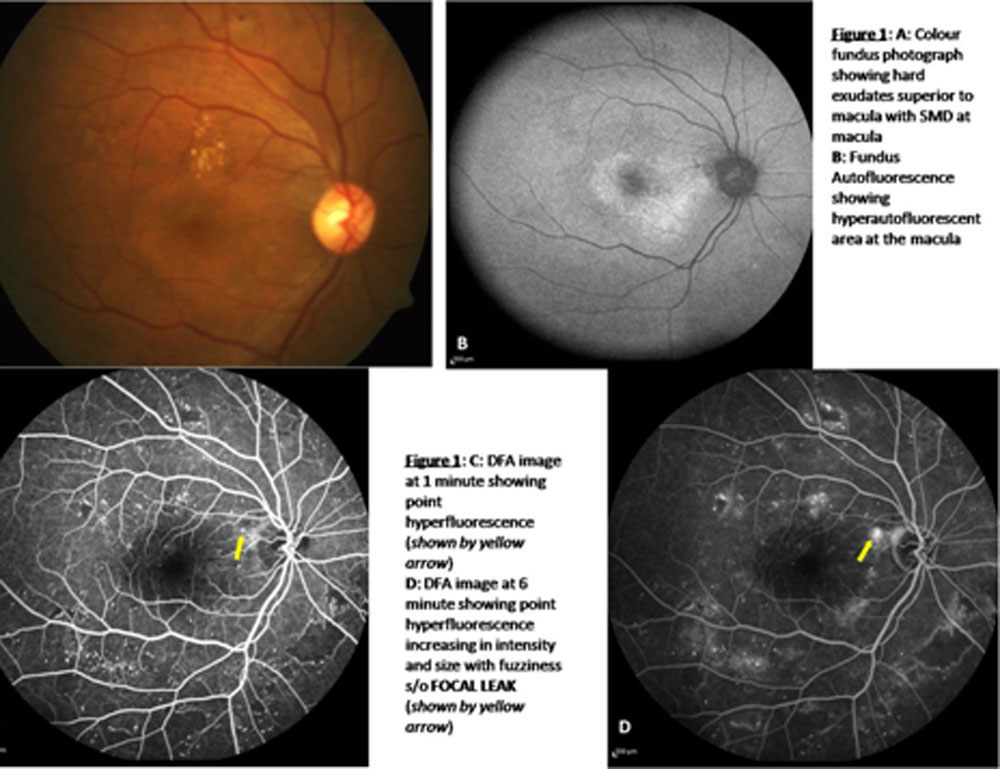
Figure 2
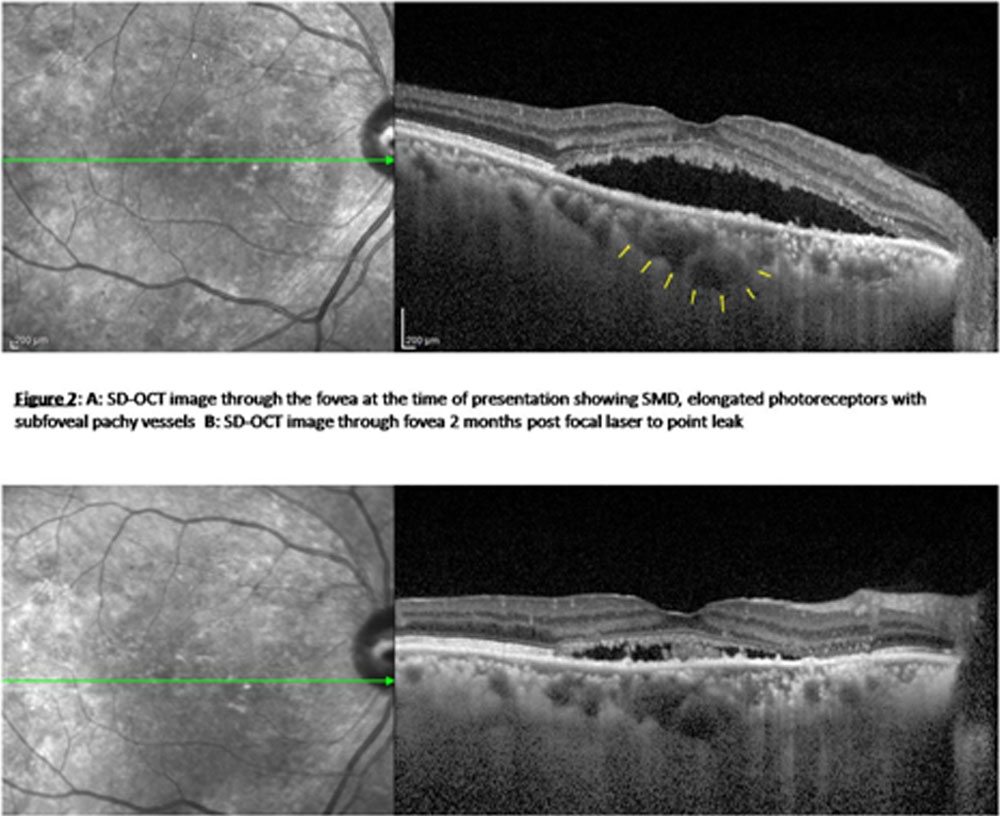
Figure 3 A.B.C showing focal leaks
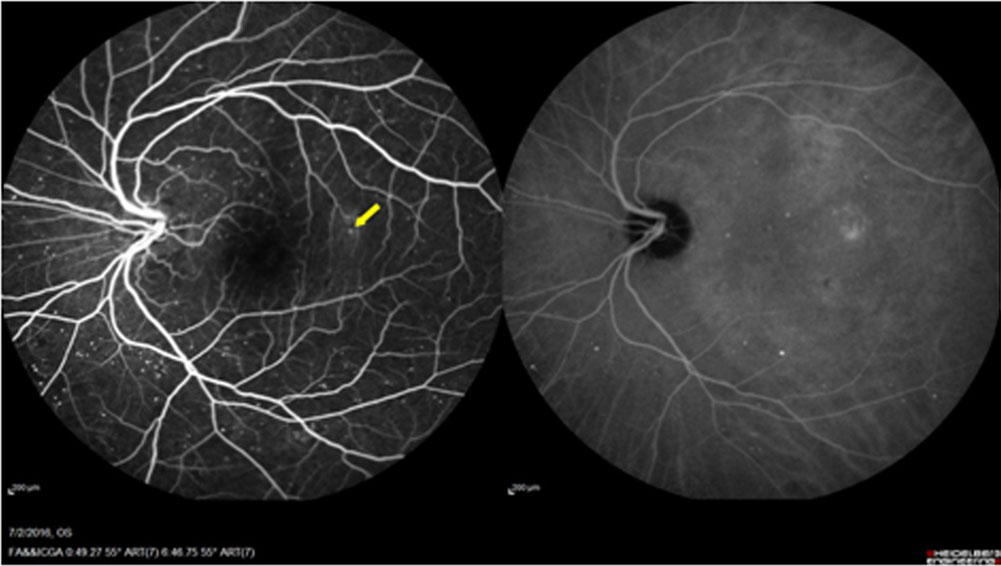
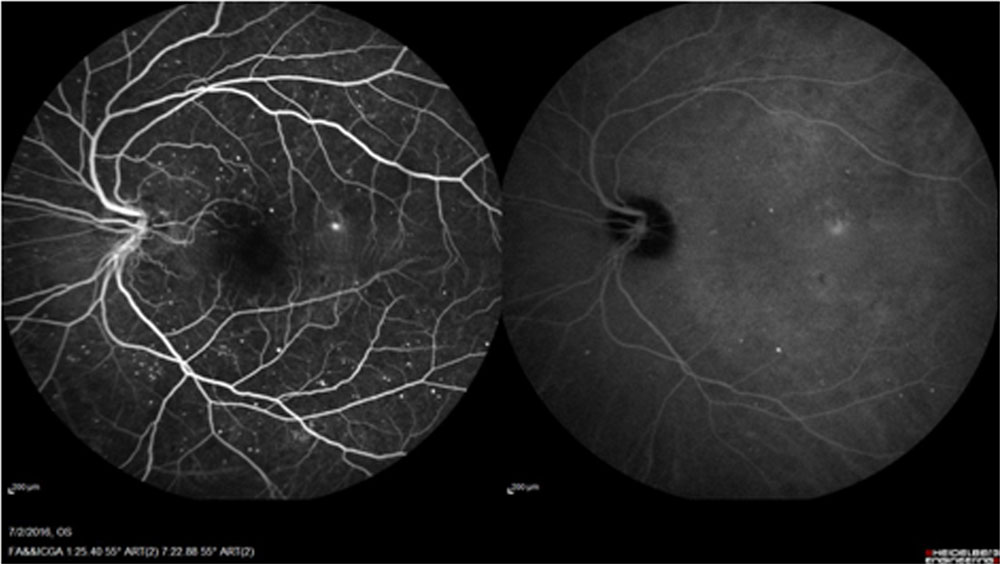
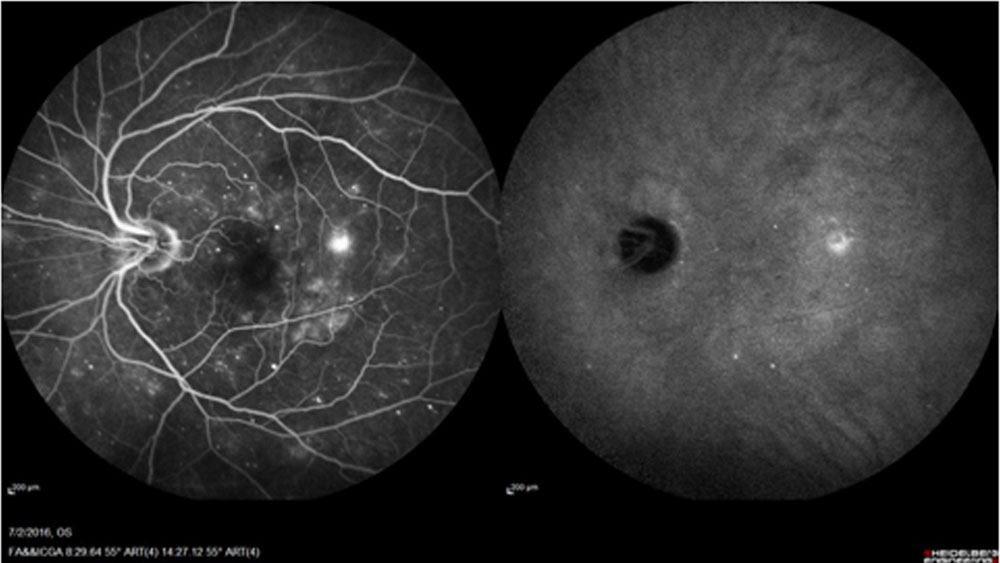
Figure 3 D FAF and E OCT
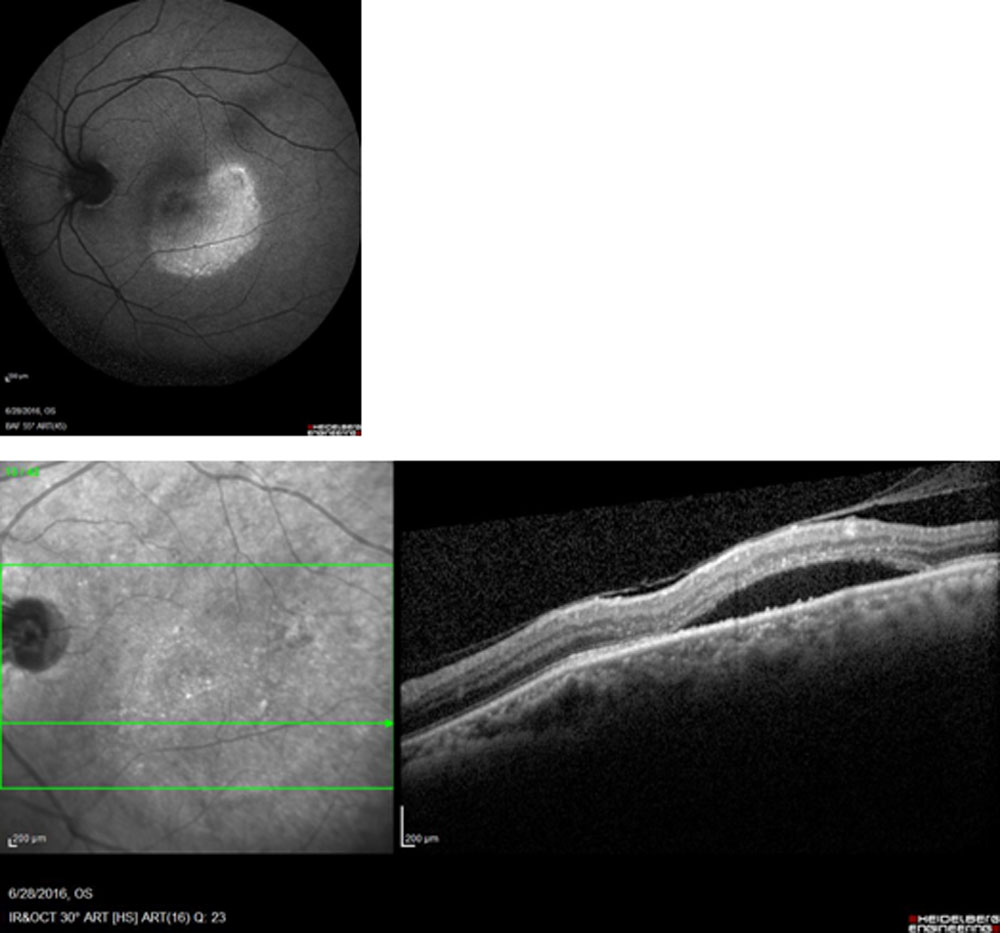
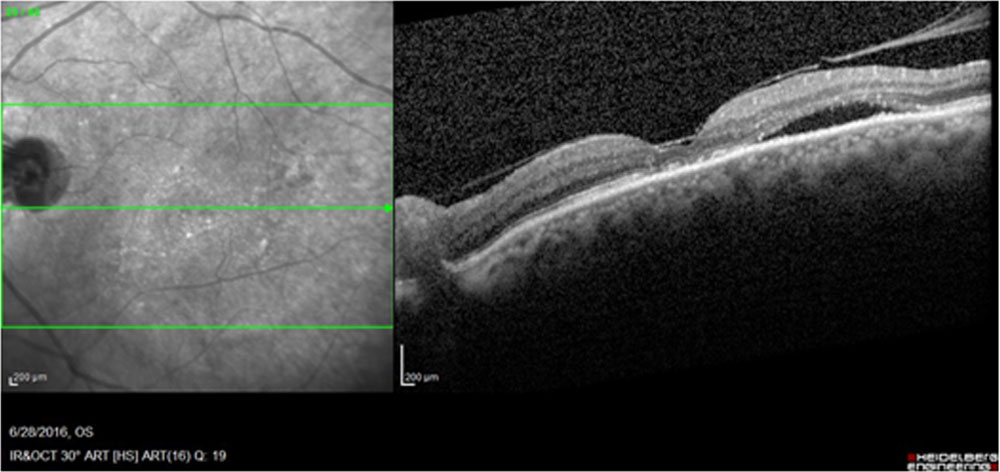
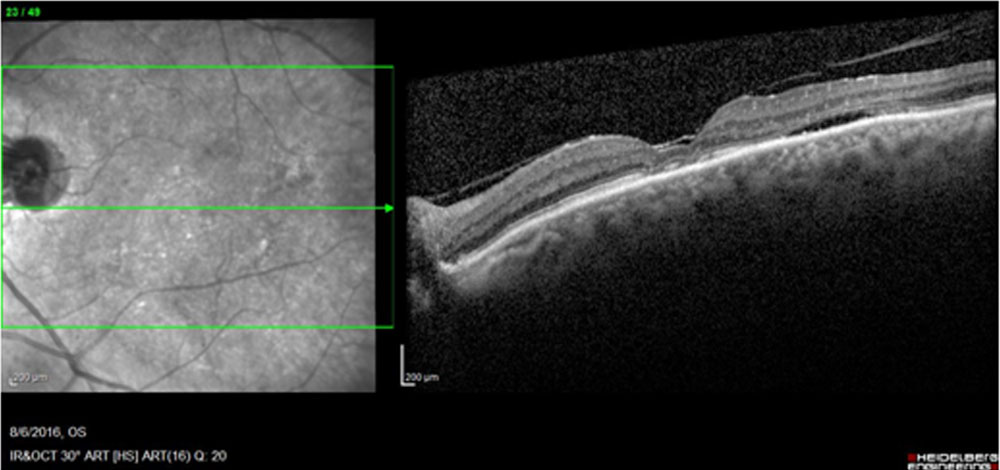
Figure 4 A and B: Before and after Conservative management
Discussion:
OCT has changed the management of DME over the last decade along with intravitreal pharmacotherapy. Laser photocoagulation has taken a back seat in the current scenario. The entity of serous macular detachment in DME was appreciated only with OCT. CSME has lost the primary importance in managing DME.Identifying the structural changes in eyes with DME using OCT may allow more effective management of these patients. A uniform and precise classification of DME would increase the possibility to optimize our indications, to compare and to judge the results of different therapeutic strategies.
OCT classification of DME has five types described in literature: type 1 focal macular thickening, type 2 diffuse macular edema without cysts including spongiform, type 3 cystoid macular edema, type 4 tractional macular edema, type 5 serous retinal detachments.Each of the morphologic subtypes of DME represents distinct entity that requires specific treatment regimens to achieve the best final result. The OCT type 4 with tractional component should be the best candidate for vitrectomy.Subfoveal serous detachment responds well to intravitreal pharmacotherapy.
We are describing a new type of DME, which is characterized by large SMD with Pachychoroid or pachyvessels and RPE leak. The debate will be whether this is an association of CSCR with DME or a new type of DME. Diabetic changes in the choroidal vessels or diabetic choroidopathy is coming into clearer picture with the advent of multimodal imaging. We would like to believe that this subtype is a new DME type because of the following reasons- 1. It is not an uncommon situation. 2. Treatment implications are more considering the fact that focal laser to RPE leaks may work wonders compared to intravitreal injections.
Diabetic chorioretinopathy should be suspected if there is a large SMD. A careful FFA may give you RPE leak. This may be challenging in the presence of a lot of Microaneurysms. Fundus autofluorescence showing the hype auto fluorescent patches may give a clue to look for RPE leak. Also EDI shows pachyvessels.
Younger patients and longer duration of diabetes were found to be a risk factor for this type. The number of patients in the series was not adequate to study the risk factors statistically. Hypertension may be a factor leading to choroidal hyperpermeability in these cases.
Larger series of similar cases may give insights to this new subtype addressing the pathophysiology, risk factors and management strategies
Conclusion:
FFA and Fundus autofluorescence confirm CSCR like picture in some diabetic retinopathy cases with large serous macular detachment in OCT. This could be a new subtype of DME called Diabetic Chorioretinopathy (DCR) supported by the EDI and presence of pachyvessels rather than an association of DME with CSCR.
Leave a Comment