
Dr. Aditi Singh, S16943, Dr. Meena Gopinath Menon
Introduction:
In India, the estimated number of cases of glaucoma is 12 million, around one fifth of the global burden of glaucoma.1The National Blindness survey 2001 showed that glaucoma is the third major cause of blindness in India and is responsible for 5.9% of blindness (VA <6/60).2
Trabeculectomy is the gold standard for intraocular pressure control, however in refractory cases, glaucoma drainage devices (GDDs)play a predominant role in getting the intraocular pressure under control. Even in pediatric glaucoma, surgical management (trabeculotomy or goniotomy or trabeculotomy with trabeculectomy) is the mainstay of treatment.3 ,4Howeverthe use of glaucoma drainage devices (GDD) has gained an increased importance in a glaucoma surgeon’s armamentarium for treatment of advanced and refractory cases in both adults and children . Refractory glaucoma is one which does not respond adequately to medical and surgical treatment and needs subsequent surgical intervention. GDDs are typically used in uveitic glaucomas, neovascular glaucoma, post penetrating keratoplasty surgery or post vitreoretinal surgery. Even in children,they are especially used in situations where filtering surgery has failed or is known to have a high risk of failure, such as significant conjunctival scarring,prior surgeries or aniridia. 5,6 The Ahmed glaucoma valve (AGV; New World Medical, Inc., Rancho Cucamonga, California, USA) is a shunt device with a restriction flow mechanism, to prevent early postoperative hypotony, that is used in refractory glaucoma as either a primary surgical option or after failure of conventional filtration procedures.7,8The purpose of this study is to evaluate the safety and efficacy ofAGV implants in refractory glaucomas in children as well as adults, in a tertiary care eye hospital in India .
Material and Methods:
This is a retrospective cohort studyof29 patients,both adults and children with refractory glaucoma who underwent tube shunt surgery using AGV with or without combined surgical procedures like phacoemulsification with intraocular lens (IOL) implantation,
penetrating keratoplasty (PK)or keratoprosthesis (Kpro) by a single surgeon in the Department of Ophthalmology, Sankara Eye Hospital, between August 2012 and August 2015.
Data Collection:
Medical records of all the patients operated with AGV between August 2012 and August 2015, for refractory glaucoma were included in this study. Pre-operative data were collected from patients’ recordsincluding age at the time of surgery, gender, eye laterality,specific glaucoma diagnosis, number of anti-glaucoma medicationsused pre-operatively, number of prior incisional surgeries and pre-operative IOP on medicaltreatment. Postoperative data included IOP on last follow up, number of anti-glaucoma medications usedpost-operatively, any significant intra-operative or post-operativecomplications and any additional surgical intervention.
Preoperative and postoperative IOPs were measured by Goldmann applanation tonometry when applicable and/or Tono-Pen in eyeswhere using Goldmann tonometry was not possible. Success
was defined as IOP lower than 21mmHg and higher than 5 mmHg with or without glaucoma medications, (qualified and complete success) without additional glaucoma surgery and without the loss of light perception. The HP(needs full form of HP)was defined as IOP > 21 mm Hg during the first 3 months after surgery. Resolution of the HP was defined as an IOP < 22 mm Hg and an IOP reduction of 3 mm Hg with the same or fewer number of glaucoma medications.Patients were followed up for a minimum of 6 months.
Surgical technique:
The surgical procedure consisted of AGV implantation (models FP7, FP8) using a standardized surgical technique by a single surgeon. Surgery was done after obtaining informed written consent under peribulbar or general anesthesia. After applying a corneal traction suture, a fornix-based conjunctival flap and tenon’s capsule were dissected to allow insertion of the plate of the implant into sub-tenon’s space 8 mm behind the corneal limbus in superotemporal quadrant. In one case with superior ciliary staphyloma, AGV had to be implanted in inferotemporal quadrant. Before insertion of the plate, the valve of the implant was primed with balanced salt solution. The plate wasfixed to the sclera with 9–0 black nylon sutures. The tube was shortened to the desired length with its sharp bevel facing anteriorly to allow 2–3 mm of tube in anterior chamber. The tube of the implant entered the AC parallel to the iris planethrough the sclerostomy.Concurrentanterior or pars plana vitrectomy was performed in aphakicpatients and in patients in whom pars plana insertion of tubewas planned. In case where AGV was inserted with Boston Keratoprosthesis Type II, Kpro was instilled after the AGV tube had been inserted into the AC. The tube was anchored to the sclera with 9–0 blacknylon (Ethicon, Ethilon) suture. The anterior part of the tubewas covered with a partial thickness donor scleral patch graft, which was thenfixed to the sclera with 9–0 black nylon sutures. The conjunctivawas closed with 10-0 nylon suture. Patients with neovascular glaucoma were treated withpanretinal photocoagulation and/or intravitreal bevacizumab(Avastin, Genentech, South San Francisco, CA, USA) beforethe AGV was implanted.
Definition of success and failure:
The primary outcome variable for success was postoperative IOP on last follow up less than 21mmHg and more than 5mmHg, in the absence of devastating ocular complications, without further glaucoma surgeries, with or without anti-glaucoma medications. Eyes that met the above criteria and were not on supplemental anti-glaucoma medical therapy were defined as complete successes and those that met the criteria with supplemental medical therapy were defined as qualified successes. Eyes not adhering to these criteria were considered as failures.
Statistics
Clinical data was analyzed using SPSS software. Simple descriptive statistics (frequency, mean, percentage) were used to describe the study variables. The difference of the meanpreoperativeand postoperative IOP was calculated using Wilcox Sign Rank Test, due to a small sample size. Mean reduction in preoperative and post-operative IOPs between the qualified success group, complete success group and the failure group was calculated using a nonparametric test, Krushkal Value Test, again because of a limited sample size. Kaplan-Meier survival analyses were applied to assesslong-term success and was done for two groupsof eyes: those who hadnot undergoneprior glaucoma surgery and those who had undergone prior glaucoma surgery. Kaplan-Meier survival analyses was also applied to calculate the cumulative probability of survival in all the patients.
Results:
Preoperative characteristics:
The present study included 29 eyes from 29 glaucoma patients who underwent an AGV implant. Table 1 shows clinical and demographic characteristics of the subjects.Patients were followed for a mean duration of2.62 yrs ± 1.84years. Mean age was 31.86± 22.092 years. Among the 29 patients 12 (49.37 %) were of pediatric age group and 17 (58.62 %) were adults. 2 children received the Ahmed FP 8 valve and the rest underwent Ahmed FP7 valve implantation. There were 15(51.7 %) males and 14 (48.3 %)females. 12 (41.4 %) cases were of right eye and 17(58.6%) of left eye.
The most common type of glaucoma was post traumatic glaucoma 8 cases (27.6%), followed by post retinal detachment surgery secondary glaucoma, post Penetrating Keratoplasty (PKP) secondary glaucoma and neovascular glaucoma 4 cases (17.20%), in each category , post IOL surgery secondary glaucoma and congenital glaucoma 2 cases (6.9%) in each category , uveitic glaucoma , primary angle closure glaucoma (PACG) primary open angle glaucoma (POAG) and glaucoma due to other causes such as congenital aniridia syndrome 1 case (3.4%) respectively .
TABLE 1:
Characteristics of patients treated with Ahmed glaucoma valve implant surgery n-29:
| Age (years)
Mean ±SD
|
31.86 ± 22.092 |
| Gender, ?(%)
Male Female |
15 (51.7%) 14 (48.3%) |
| Eye, ?(%)
Right Left |
12 (41.4%) 17 (58.6%) |
| Type of implant, ?(%)
Ahmed FP 8 Ahmed FP7 |
2 (6.89 % ) 27 (93 .10%) |
| Adults,?(%)
Pediatric |
17 (58.62%)
12 (51.17%) |
| Type of glaucoma, ?(%)
Traumatic Neovascular Penetrating keratoplasty Post retinal detachment surgery Post IOL surgery Congenital Primary open angle Uveitic Primary angle closure Others |
8 (27.6% ) 4 (17.20 %) 4(17.20 %) 4(17.20 %) 2 (6.9%) 2 (6.9%) 1 (3.4%) 1(3.4%) 1(3.4%) 1(3.4%) |
| Follow-up (years)
Mean ±SD |
2.26 ± |
Previous interventions:
7 cases (24.13%) had undergone RD surgery ± Silicon oil removal . 4 (13.79%) underwent PKP . 3 cases each (10.34%) underwent RD surgery with lensectomy and RD surgery with trabeculectomy . 2 cases (6.89%) had undergone IOL surgery . 1 case (3.44%) each had undergone trabeculectomy + trabeculotomy , trabeculectomy, corneal tear repair + RD surgery + SOR + PKP and RD surgery + lens aspiration + trabeculectomy . (Table 2)
Table 2: Previous Interventions:
Prior Surgeries n (%)
| Trabeculectomy + trabeculotomy | 1 (3.44%) |
|
Trabeculectomy |
1 (3.44%) |
| PKP | 4 (13.79%) |
| RD surgery with lensectomy | 3 (10.34%) |
| RD surgery ±
Silicon oil removal |
7 (24.13%) |
| RD surgery with trabeculectomy | 3 (10.34%) |
| Corneal tear repair + RD surgery + SOR + PKP(later) | 1(3.44%) |
| IOL surgery | 2 (6.89%) |
| RD surgery + Lens aspiration + trabeculectomy | 1(3.44%) |
| Nil Intervention | 6 (20.68%) |
In 20 (68.96 %), cases AGV was inserted in anterior chamber and 9(31.03%) cases in pars plana. 2 (6.89%) caseswere of AGV in anterior chamber along with IOL insertion and 1 (3.44 %) case of AGV implantation along with keratoprosthesis. (Table 3)
Table 3:
Ahmed glaucoma valve drainage device (AGV) surgery: Types of Procedure
| Type of procedure | N (%) | Additional procedure |
| AGV in AC | 20 (68.96%) | 1AGV in inferotemporal quadrant (one due to ciliary staphyloma superiorly and other due to unhealthy conjunctiva following multiple surgeries).
2 cases were performed with simultaneous removal of Band Buckle. 1 case was along with Kpro insertion ( congenital aniridia) 2 cases were performed along with IOL implantation
|
| AGV in pars plana | 9 (31.03%) |
Mean IOP decreased from 36.20 ±9.92 pre-operatively to 14.88 ± 6.46 mmHg at the last follow-up (?< 0.001). Mean number of medications decreased from 3.14 ± 0.875 prior to surgery to 2.10 ± 1.17at the last follow-up (?< 0.001). Table 4
Table 4:
Comparison between baseline and postoperative IOP and glaucoma medications.
Parameters Baseline Postoperative ?value
| IOP
Mean ± SD |
36.20 ± 9.92 | 14.88 ± 6.46 | <0.001 |
| Glaucoma medications
Mean ± SD |
3.14 ± 0.875 | 2.10 ± 1.17 | <0.001 |
A total of 2 eyes ( 6.89 %) had filtering surgery only prior to theAGVimplantation. 4 eyes ( 13.79 %) underwent filtration surgery along with other surgeries. 17 ( 58.62 %) patients had undergone other surgeries but not filtration surgeries . 6 ( 20.68 %) patients did not have any previous surgeries. The mean reduction in IOP pre and post-operative in the qualified success, complete success and the failure group was significant (p < 0.30). It was calculated using Krushkal Value Test, a nonparametric test used due to limited sample size .Total cases of success were 20 (68.96%),2 cases of complete success and 18 cases of qualified success. Hypertensive phase was seen in 9 (31.03%) out of 29 eyes. Out of these in 4 eyes the IOP returned to normal after 6 months, with the patients being on AGMs. In 5 of the eyes IOP could not be brought under control even with maximum medical therapy.
There were 9 (31.03%) cases of failure. The major cause of failure was excessive fibrosis and encapsulated cyst formation in 5 cases .All these cases faileddue to high IOP despite being on additional antiglaucoma medications. In one of these eye needling was tried due to encysted bleb, but the bleb failed eventually. The cause of failure in the rest of the cases is described below. In one eye, the tube of AGV got blocked due the keratoprosthesis and the tube had to be removed eventually. In another case the AGV was explanted because of scleral patch giving way and the pars plana clip extrusion. One patient in whom tube was reinserted into anterior chamber with a tube extender after removing it from pars plana, had tube exposure thrice and finally tube had to be removed, and the patient underwent trasscleral cyclophotocoagulation. Blebitis at 14 months of surgery was another cause of valve explanation. This patient too underwent trasscleral cyclophotocoagulation to control the IOP.
Surgical complications and additional surgeries:
There were no intraoperative complications.There were total of 13 cases with post-operative complications with 7 resurgeries were reported .
1st case eye had to undergo keratoprosthesis implantation post AGV due to failed penetrating keratoplasty. The tube of AGV subsequently got partially blocked against the Kpro plate.2nd case of pars plana AGV insertion, tube exposure was seen which was covered with amniotic membrane but later there was extrusion of the pars plana clip with scleral patch giving way for which the tube was explanted.
3rd case there was conjunctival retraction seen twice which was corrected with repositioning and suturing the conjunctiva. This was followed by a third episode for which scleral patch graft, amniotic membrane, conjunctival auto graft from inferior fornix and postoperative doxycycline oral tablets were used for 2 months.
4thcase, there was tube exposure near its entry site in pars plana insertion, so it was repositioned in anterior chamber by using tube extender. Finally this tube had to be removed due to 3 more episodes of tube exposure.
5th case tube had to be reinserted from anterior chamber into pars plana due to exposure.
6th case developed blebitis for which the tube had to be explanted.
Hypertensive phase was seen in 9 cases, out of which 4 resolved and 5 cases failed. In one of the cases bleb needling was done at the end of first month but this bleb subsequently failed.
2 cases had localized corneal endothelial decompensation due to tube endothelial touch and patients were started on hypertonic saline but these patients did not come for further follow up .Table 5.
Table 5 :Post-operative complications:
Case no Postop complications Intervention success/ failure
| 1 | AGV tube block d/t Kpro plate | AGV explantation | Failure |
| 2 | Tube exposure ,
pars plana clip exposure and scleral patch giving way |
AMT and conjunctival repositioning for tube exposure ,
Agv explantation subsequently |
Failure |
| 3 | 2 incidences of tube exposure
3rd episode of conjunctival exposure |
Conjunctival repositioning twice
Scleral patch graft , amniotic membrane, conjuctval auto graft from inferior fornix and postoperative doxycycline oral tablets , for 3rd episode |
Qualified success |
| 4 | tube exposure near its entry site in pars plana insertion
3 more episodes of tube exposure |
Repositioned in anterior chamber by using tube extender
Agv explantation subsequently |
Failure |
| 5 | Tube exposure near the limbus | Inserted into pars plana | Qualified success |
| 6 | Encysted bleb | Bleb needling | Failure |
| 7 | Blebitis | Agv explantation | Failure |
| 8 | Tube endothelial touch | Started on hypertonic saline | Qualified success till last follow up |
| 9 | Tube endothelial touch | Started on hypertonic saline | Qualified success till last follow up |
| 10,11,12,13 | Hypertensive Phase | Anti-glaucoma medications | Failure |
In Kaplan Meier survival analysis ,there was an 83% success rate at 1 year and 77% , 62% and 49% success rate at 2 years , 3 years and 4 years respectively ,for all the patients who had undergone glaucoma surgery.( Figure 1 )
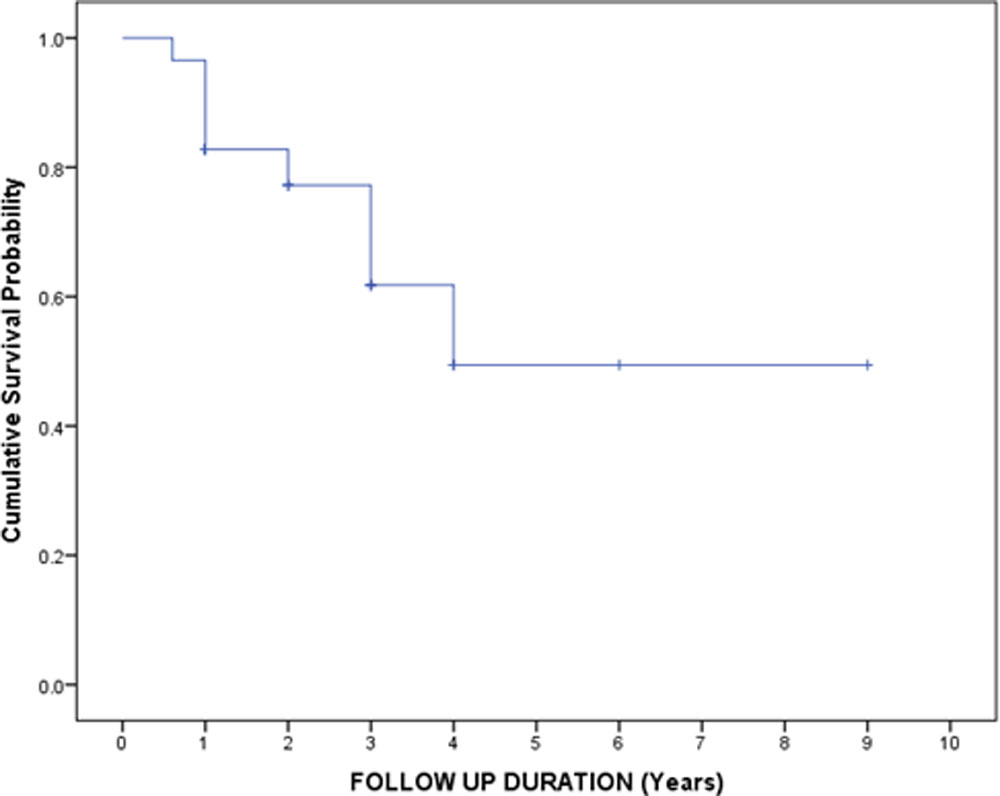
Figure: 183% success rate at 1 year and 77%, 62% and 49% success rate at 2 years, 3 years and 4 years respectively, for all the patients who had undergone glaucoma surgery.
The cumulative probability of success at 1 year was 96% and 78% at 2years and 3 years respectively and 59% at 4 years and from 6 to 9 years it remained same 59% (n=23) in the eyes that had not undergone prior glaucoma surgeries, compared with 80% at 1, 2 years and 3 years and 40% at 4 years in the eyes (n =6) that had undergone prior glaucoma surgeries. (Figure 2)
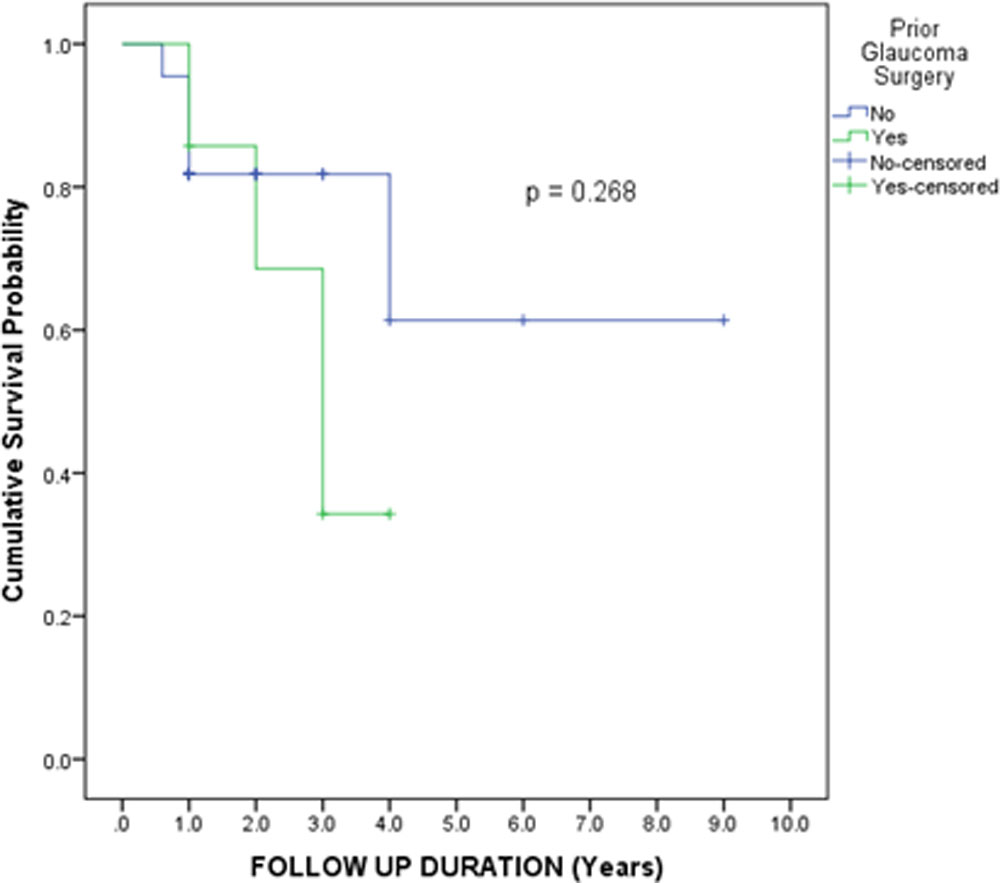
Figure 2:96% and 78% at 2years and 3 years respectively and 59% at 4 years and from 6 to 9 years it remained same 59% (n=23) in the eyes that had not undergone prior glaucoma surgeries, compared with 80% at 1, 2 years and 3 years and 40% at 4 years in the eyes (n =6) that had undergone prior glaucoma surgeries.
Discussion:
The AGV was launched in 1993 as the first GDD with a unidirectional valve mechanism contributing to the prevention of postoperative hypotension9 . The two models of AGV which we used in this study, differ in their surface areas: FP8 (96 mm2) is used in children and FP7 (184 mm2) is usually used in adults.
According to different authors, the AGV implantation is considered an effective treatment option for patients withrefractory glaucoma and the success varies in a wide range from 43 to 83.6%. 10-14
It is difficult to compare surgical success rates from different published studies because of the differences in the populations studied, types of implants used, and lengths of follow-up.
In the present study, the mean IOP was reduced by 58.89 % from the baseline of 36.20 ± 9.92 pre-operatively to 14.88 ± 6.46 mmHg at the last follow-up; 2/29eyes (6.89 %) had complete successes while 18/29 eyes (62.06 %) had qualified success. This is in agreement with outcomes reported in the literature.
The cumulative probability of success at one year in our study was 83%, which is similar to what has been seen in other studies. 15-18 . The Kaplan-Meier survival analysis performed on two subgroups of eyes demonstrated a favorable surgical outcome for those eyes that had not undergone prior glaucomasurgery compared with the eyes that had undergone prior glaucoma surgery as seen in other studies. 10
There were 9 (31.03%) cases of failure. Our study also found that the hypertensive phase was a
major risk factor for AGV failure. In our sample, the hypertensive phase occurred in 9 out of 29 eyes (31.03 %), among which 5 failed. Previous studies have reportedan incidence of hypertensivephase ranging from 56 to 82% following the implantation of a glaucoma drainage device. Thus the major cause of failure was excessive fibrosis and encapsulated cyst formation which was consistent with the other studies.19,20
There were four cases of tube exposure, out of which 2 cases had episodes of recurrent exposure out of which one case had qualified success after surgical intervention. In 2 cases AGV had to be explanted. 3 of these cases had undergone multiple previous surgeries and one case was of NVG.This was similar to studies done previously.21
The current study is limited by its retrospective design, small sample size and the short period of follow-up. To conclude, it is safe to say that AGV implantation has proved itself as an effective surgical modality for refractory glaucoma.
REFERENCES
- Glaucoma: An emerging peril. RohitSaxena, Digvijay Singh, Praveen Vashist 2013 | Volume : 38 | Issue : 3 | Page : 135-137
- Murthy GV, Gupta SK, Bachani D, Jose R, John N. Current estimates of blindness in India. Br J Ophthalmol 2005;89:257-60.
- Beck AD. Diagnosis and management of pediatric glaucoma. Ophthalmol Clin North Am 2001; 14: 501–512.
- Turach ME, Aktan G, Idil A. Medical and surgical aspects of congenital glaucoma. Acta Ophthalmol Scand 1995; 73: 261–263.
- .Netland PA, Walton DS. Glaucoma drainage implants in pediatric patients. Ophthalmic Surg 1993; 24: 723–729.
- Ishida K, Mandal AK, Netland PA. Glaucoma drainage implants in pediatric patients. Ophthalmol Clin North Am 2005; 18: 431–442.
- Wilson MR, Mendis U, Smith SD, Paliwal A. Ahmed glaucoma valve implant vs trabeculectomy in the surgical treatment of glaucoma: a randomized clinical trial. Am JOphthalmol 2000;130:267–273.
- Coleman AL, Smyth RJ, Wilson MR, Tam M. Initial clinical experience with the Ahmed glaucoma valve implant in pediatric patients. Arch Ophthalmol 1997;115:186 –191.
- Coleman AL, Hill R, Wilson MR, Choplin N, Kotas-Neumann R, Tam M, Bacharach J, Panek WC. Initial clinical experience with the Ahmed glaucoma valve implant. Am J Ophthalmol 1995Jul;120(1):23-31.
- Souza C, Tran DH, Loman J, Law SK, Coleman AL, Caprioli J. Long-term outcomes of Ahmed glaucoma valveimplantation in refractory glaucomas. Am J Ophthalmol 2007 Dec;144(6):893-900. Epub 2007 Oct 4.
- Papadaki TG, Zacharopoulos IP, Pasquale LR, Christen WB, Netland PA, Foster CS. Long-term results of Ahmed glaucoma valve implantation for uveitic glaucoma. Am J Ophthalmol 2007 Jul;144(1):62-69. Epub 2007 May 9.
- Lima FE, Magacho L, Carvalho DM, Susanna R Jr, Avila MP. A prospective, comparative study between endoscopic cyclophotocoagulation and the Ahmed drainage implant in refractory glaucoma. J Glaucoma 2004 Jun;13(3):233-237.
- Christakis PG, Kalenak JW, Zurakowski D, Tsai JC, Kammer JA, Harasymowycz P, Ahmed II. The Ahmed versus Baerveldt study: one-year treatment outcomes. Ophthalmol 2011 Nov;118(11):2180-2189.
- Quaranta L, Riva I, Floriani IC. Outcomes of using a sutureless bovine pericardial patch graft for Ahmed glaucoma valve implantation. Eur J Ophthalmol 2013 Sep-Oct;23(5):738-742.
- Shah MR, Khandekar RB, Zutshi R, Mahrooqi R. Short term outcome of Ahmed glaucoma valve implantation in management of refractory glaucoma in a tertiary hospital in Oman. Oman J Ophthalmol 2013; 6: 27-32.
- Ozdal PC, Vianna RN, Deschenes J. Ahmed valve implantation in glaucoma secondary to chronic uveitis. Eye 2006; 20: 178–183.
- Tai MC, Cheng JH, Chen JT, Liang CM, Lu DW. Intermediate outcomes of Ahmed glaucoma valve surgery in Asian patients with intractable glaucoma. Eye 2010; 24(4):547-52.
- Li Z, Zhou M, Wang W, et al. A prospective comparative study on neovascular glaucoma and nonneovascular refractory glaucoma .\
- Ayyala RS, Zurakowski D, Monshizadeh R, Hong CH, Richards D, Layden WE, et al. Comparison of double-plate Molteno and Ahmed glaucoma valve in patients with advanced uncontrolled glaucoma. Ophthalmic Surg Lasers 2002;33:94–101.
- Panda A, Prakash VJ, Dada T, Gupta AK, Khokhar S, Vanathi M. Ahmed glaucoma valve in post-penetrating-keratoplasty glaucoma: a critically evaluated prospective clinical study. Indian J Ophthalmol 2011;59:185–9.
- Y. S. Byun, N. Y. Lee, and C. K. Park, “Risk factors of implant exposure outside the conjunctiva after Ahmed glaucoma valve implantation,” Japanese Journal of Ophthalmology, vol. 53, no. 2, pp. 114–119, 2009
Leave a Comment