
Dr. Gitansha Sachdev, S15438, Dr. Ramamurthy D, Dr. Shreyas Ramamurthy
ABSTRACT
Purpose: To compare visual outcomes of SMILE and topoguided LASIK for the treatment of myopia and myopic astigmatism
Methods: This interventional case series included 200 eyes in each group. The following parameters were evaluated preoperatively and up to 3 months postoperatively: uncorrected (UDVA) and corrected distance visual acuity (CDVA), residual refractive error and higher order aberrations.
Results: At 3 months, 76.5% eyes following SMILE and 79.5% in the LASIK group had a UDVA of 20/20, while 12.5% and 10% of the eyes had a UDVA of 20/16 respectively. The safety and efficacy was 98% and 94.5% respectively in the LASIK group and 97% and 91.5% respectively in the SMILE group (P=0.43 and 0.37). The mean residual refractive error was greater in the SMILE group (-0.63D). 6.5% and 1 % eyes in the SMILE and LASIK group respectively lost 1 or more lines of uncorrected visual acuity. The incidence was greater in eyes with a preoperative refractive astigmatism of more than 1 Diopter (p=0.22). A significant decrease in coma and trefoil was noted postoperatively in the LASIK group (P= 0.024 and 0.632). On the contrary, SMILE demonstrated an increase in trefoil, although the results were not statistically significant (p=0.4432). The induced spherical aberrations were significantly lower following SMILE (P=0.0001).
Conclusion: Refractive outcomes following topoguided LASIK were superior to SMILE with a lower induction of trefoil. However, the spherical aberrations induced were lower in the SMILE group. Further studies are needed to validate the superiority of one procedure over the other.
Introduction
Corneal refractive surgery has advanced over the past few decades since its inception in the late 1990’s. With a greater understanding of the optical aberrations of the eye various excimer laser ablation patterns have evolved. Wavefront guided ablation profiles correct both the higher and lower order aberrations. The wavefront optimized approach minimizes the ablation induced spherical aberrations, with virtually no loss of contrast, postoperative glare or haloes. However, it does not address the preexisting optical aberrations. [1] Topography guided customized ablation is the latest modality of excimer treatment. [2-3] As a majority of the ocular aberrations arise from the corneal surface and are more static in nature, topoguided ablation attempts to maintain corneal asphericity while neutralizing abnormalities.
In Small Incision Lenticule Extraction (SMILE) the femtosecond laser creates four sequential photo ablative cuts to fashion an intrastromal lenticule, which is subsequently extracted to offer a refractive correction. Various studies have reported several advantages of SMILE in refractive efficacy and biomechanical stability. [4-5] As the lenticule has an aspheric profile the aberrations induced by SMILE are likely to be lower.
At present the postoperative aberrations following SMILE and topoguided customized ablation profiles have not been compared in literature. This prospective interventional case series was designed to compare the efficacy, refractive predictability and postoperative aberrations in SMILE and topoguided LASIK.
PATIENTS AND METHODS
Four hundred eyes of 200 consecutive patients were included in this prospective, interventional case series conducted at a tertiary eye care hospital in South India. The study received approval from the Ethics Committee of our institute and was conducted in accordance with the tenets of the Declaration of Helsinki. A written informed consent was obtained from all patients prior to the surgical procedure.
STUDY POPULATION
The study was conducted on patients who presented to our Refractive Services during January 2016 to March 2017 seeking refractive correction. The inclusion criteria was age between 18 to 50 years with a documented refractive stability for a minimum period of one year (a change of 0.25 diopters [D] or less) and discontinuation of contact lenses for at least two weeks. Patients with a corrected distance visual acuity (CDVA) of 20/25 or better, a spherical equivalent refraction of up to -10.00 D with a cylindrical correction of up to -5.00 D were included in the study. Exclusion criteria included a central corneal thickness less than 490μm, a residual stromal bed lower than 290μm, topographic evidence of corneal ectasia, previous ocular surgery, history of herpetic eye disease, corneal scarring, collagen vascular disease, pregnancy and lactation.
STUDY DESIGN
Preoperative evaluation included uncorrected (UDVA) and corrected distance visual acuity (CDVA), manifest and cycloplegic refraction, slit lamp biomicroscopy and dilated fundus evaluation. Corneal topography data for topography-guided custom ablation treatment (T-CAT) was obtained from the Vario placido based topography (Wavelight, Erlagen, Germany) and Scheimpflug corneal tomography with Oculyzer II (Wavelight). Higher order abberations were measured using the Oculyzer II.
STUDY TREATMENTS AND PROCEDURES
All surgeries were performed by experienced surgeons under topical anaesthesia and aseptic conditions. Small Incision Lenticule Extraction (SMILE) procedure was performed using the VisuMax femtosecond laser (Carl Zeiss Meditec, Jena, Germany) with an intended cap thickness of 120 microns and optical zone of 6.5 mm. The posterior cut was fashioned first from the periphery to centre followed by the anterior cap cut in a spiral out fashion. This was followed by a superior side cut of 90-degree angulation and 50 degrees cordal length.
LASIK flaps were fashioned using the VisuMax system with an intended thickness of 100 microns and a flap diameter of 8.5mm. Following blunt dissection and flap lift, the stromal bed was ablated with excimer laser (EX 500 Wavelight). The corneal pachymetry and topographic data was imported from the Oculyzer II and Vario topolyzer.
Postoperatively, both groups received treatment with topical steroids (loteprednol etabonate 0.5% ophthalmic suspension) in tapering dose and lubricating drops (carboxymethylcellulose 0.5% ophthalmic drops). Follow-up visits included postoperative day one, six weeks and three months.
STATISTICAL ANALYSIS
Data analysis was done with the help of a computer using SPSS software (version 17.0; SPSS, Inc., Chicago, IL) for Windows. Using this software, range, frequencies, percentages, means, standard deviations, and P values were calculated. A paired t test was used to test the significance of difference between quantitative variables. A P value of less than .05 denoted a significant relationship.
RESULTS
This study included 126 females and 74 males with a mean age of 24.28 years and 23.49 years in the T-CAT (Group 1) and SMILE (Group 2) respectively. The preoperative patient demographics are listed in Table 1 demonstrating age and spherical equivalent matched groups.
At the 3 months’ postoperative visit, 79.5% and 10% of the eyes demonstrated a UDVA of 20/20 and 20/16 respectively in group 1. Whereas in the SMILE group, 76.5% and 12.5% of the eyes presented with a UDVA of 20/20 and 20/16 respectively.
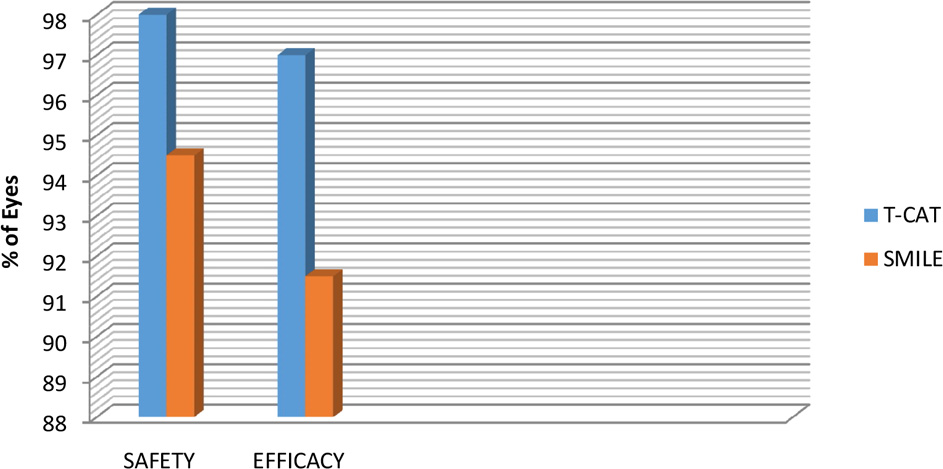
SAFETY AND EFFICACY PROFILE
The safety profile (preoperative CDVA versus postoperative CDVA) for group 1 was 98% (196 eyes out of 200) compared to 94.5% (189 eyes out of 200) for group 2. There was no statistically significant difference in safety profile of two groups (p=0.43). The efficacy (preoperative CDVA versus postoperative UDVA) for group A was 97% (194 eyes out of 200) compared to 91.5% (183 eyes out of 200) for group 2, which was not statistically significant (p=0.37). Both groups demonstrated comparable results, with slightly better outcomes in group 1. [Table 2 and 3]
Two eyes in group 1 had a residual error with a mean spherical equivalent of -0.44D (range -0.37D to -0.50D), whereas 8 eyes in group 2 showed a residual error with a mean spherical equivalent of -0.63D (range -0.25D to -1.25D). [Table 4]
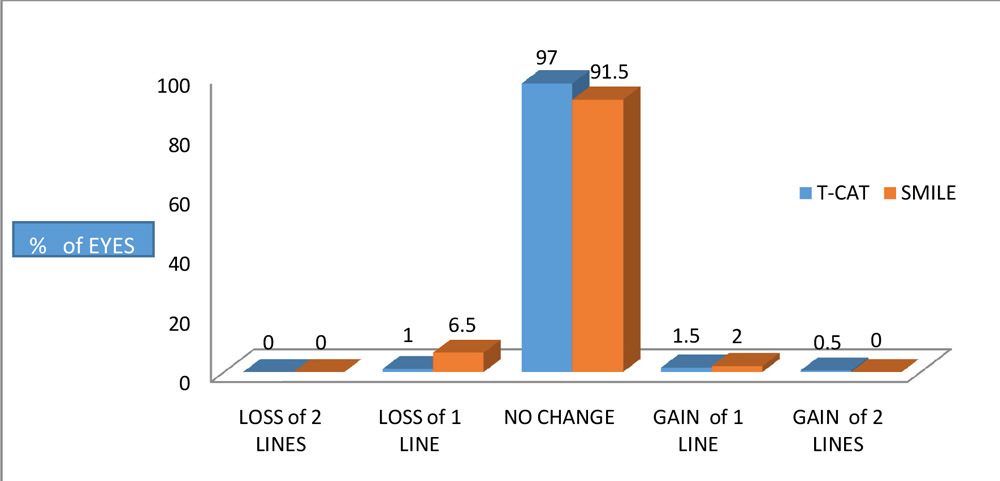
GAIN OR LOSS IN LINES
The gain-loss data at 3 months’ follow-up (preoperative CDVA versus post-operative UDVA, Table 5) demonstrated a gain of 1 or more lines in 2% (4 eyes) in each group. 1% (2 eyes) in Group 1 lost 1 line of UDVA as compared to 6.5% (13 eyes) in the SMILE group.
ACCURACY OF ASTIGMATISM CORRECTION
Patients with a preoperative refractive astigmatism of greater than 1.00D were analysed for comparing cylindrical correction outcomes. The sub groups included 105 eyes and 114 eyes in group 1 and 2 respectively. Two eyes in T-CAT group versus 8 eyes in the SMILE group, showed a loss in CDVA postoperatively (p=0.22). [Table 6]
HIGHER ORDER ABERRATIONS (HOAs)
The higher order aberrations evaluated included trefoil, coma 180, coma 90 and spherical aberrations. The preoperative and postoperative comparison of each group is shown in Table 7.
There was a significant decrease in the trefoil (p=0.632), coma 180 (p=0.0247) and coma 90 (p=0.0001) postoperatively in the T-CAT group. The increase in the postoperative spherical aberrations was statistically significant (p=0.0001).
On the contrary, in the SMILE group a postoperative increase was noted in trefoil, although the results were not statistically significant (p=0.4432). A statistically significant decrease in coma 90 (p=0.0001) and coma 180 (p=0.0004) and an increase in spherical aberrations was noted (p=0.001).
Postoperative HOAs comparison between two groups showed no statistically significant difference in trefoil (p=0.117) and coma 180 (p=0.248). However, a significant difference between the two groups in coma 90 (p=0.0001) and spherical aberrations (p=0.0001) was achieved. Postoperatively, at the end of 3 months the spherical aberration induction was significantly greater (p=0.0001) in the T-CAT group (1.97 ± 0.48) as compared to the SMILE group (1.72 ± 0.39). [Table 8]
STROMAL TISSUE CONSUMPTION
The stromal tissue ablation depth of 57.19 ± 22.05μm in group 1was significantly lower than the extracted lenticular thickness of 86.38 ± 19.75μm in group 2 (p=0.04).
DISCUSSION
Both SMILE and topo-guided customised ablation demonstrated adequate stability and efficacy for the treatment of myopia and myopic astigmatism. Previous studies have demonstrated similar outcomes following SMILE and wavefront optimised LASIK.[5-10] A contralateral eye study comparing topo-guided and wavefront optimised profiles reported similar visual outcomes.[11] However, in our study we reported slightly better results following topo-guided LASIK as compared to SMILE.
Kanellopoulus et al published data comparing SMILE and topo-guided LASIK in a contralateral eye study demonstrating superior results with the latter treatment. [12] Similar results were seen in our study with better refractive accuracy for the correction of astigmatism greater than 1 Diopter. This is probably attributed to the customisation of the laser profile, intraoperative cyclotorsion compensation and a more effective centration of the excimer platforms as compared to a manual centration by the surgeon in SMILE.
However, the earlier study did not compare the postoperative HOAs induced by the treatment. Induction of aberrations post refractive surgery can lead to glare and halos with resultant suboptimal visual quality. [13-14] Our study demonstrated a significantly lower induction of spherical aberrations in the SMILE group (1.72 ± 0.39) as compared to the LASIK group (1.97 ± 0.48) at 3 months’ postoperative visit. This could be attributed to the aspheric profile of the lenticule extracted in the SMILE procedure. An optimal aspheric corneal profile reduces ocular aberrations thereby enhancing visual quality. Lower induction of spherical aberrations has been noted following topo-guided customised ablation as compared to conventional LASIK and wavefront optimised profiles. [15]
The limitation of our study is the lack of a contralateral treatment protocol. Nevertheless, our study demonstrates results in a significantly larger sample size than has been previously described. Moreover, we compared the postoperative HOAs induced by SMILE and topo-guided ablation, which has not been reported previously to the best of our knowledge.
CONCLUSION
Topo-guided customised ablation profile offers greater accuracy of refractive treatment compared to early results of SMILE for myopia and myopic astigmatism. A customised ablation profile, intraoperative cyclotorsion compensation and an active centration are the likely causes. However, the spherical aberrations induced by SMILE are lower. Further studies are required to validate the superiority of one modality over the other.
REFERENCES:
- El Awady HE, Ghanem AA, Saleh SM. Wavefront-optimized ablation versus topography-guided customized ablation in myopic LASIK: comparative study of higher order aberrations. Ophthalmic Surg Lasers Imaging. 2011;42:314-320.
- Pasquali T, Krueger R. Topography-guided laser refractive surgery. Curr Opin Ophthalmol. 2012;23:264-268.
- Tan J, Simon D, Mrochen M, Por YM. Clinical results of topography-based customized ablations for myopia and myopic astigmatism. J Refract Surg. 2012;28:S829-S836.
- Shah R, Shah S, Sengupta S. Results of small incision lenticule extraction: All-in-one femtosecond laser refractive surgery. J Cataract Refract Surg. 2011;37:127–137.
- Sekundo W, Gertnere J, Bertelmann T, Solomatin I. One-year refractive results, contrast sensitivity, high-order aberrations and complications after myopic small-incision lenticule extraction (ReLEx SMILE). Graefes Arch Clin Exp Ophthalmol. 2014;252:837-843.
- Shen Z, Shi K, Yu Y, Yu X, Lin Y, Yao K. Small incision lenticule extraction (SMILE) versus femtosecond laser-assisted in situ keratomileusis (FS-LASIK) for myopia: a systematic review and meta-analysis. PLoS One. 2016;11:e0158176.
- Zhang J, Wang Y, Chen X. Comparison of moderate- to high-astigmatism corrections using wavefront-guided laser in situ keratomileusis and small-incision lenticule extraction. Cornea. 2016;35:523-530.
- Reinstein DZ, Archer TJ, Gobbe M. Small incision lenticule extraction (SMILE) history, fundamentals of a new refractive surgery technique and clinical outcomes. Eye Vis. 2014;1:3.
- Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol. 2011;95:335-339.
- Pedersen IB, Ivarsen A, Hjortdal J. Three-year results of small incision lenticule extraction for high myopia: refractive outcomes and aberrations. J Refract Surg. 2015;31:719-724.
- Farooqui MA, Al-Muammar AR. Topography-guided CATz versus conventional LASIK for myopia with the NIDEK EC-5000: a bilateral eye study. J Refract Surg. 2006;22:741-745.
- Kanellopoulos AJ. Topography-guided LASIK versus small incision lenticule extraction (SMILE) for myopia and myopic astigmatism: a randomized, prospective, contralateral eye study. J Refract Surg. 2017;33:306-312.
- Mrochen M, Kaemmerer M, Mierdel P, Seiler T. Increased higher-order optical aberrations after laser refractive surgery: a problem of subclinical decentration. J Cataract Refract Surg. 2001;27:362-369.
- Oliver KM, Hemenger RP, Corbett MC, et al. Corneal optical aberrations induced by photorefractive keratectomy. J Refract Surg. 1997;13:246-254.
- Shetty R, Shroff R, Deshpande K, Gowda R, Lahane S, Jayadev C. A prospective study to compare visual outcomes between wavefront-optimized and topography-guided ablation profiles in contralateral eyes with myopia. J Refract Surg. 2017; 33:6-10.
Table Legends:
| Table 1. Preoperative baseline data | |||
| T-CAT (n = 200)
mean ± SD |
SMILE (n = 200)
mean ± SD |
Pa value | |
| Age(years) | 24.28 ± 4.63 | 23.49 ± 4.06 | 0.07 |
| Sphere(D) | -3.49 ± 1.88 | -3.78 ± 1.70 | 0.32 |
| Cylinder(D) | -1.08 ± 0.82 | -1.02 ± 0.63 | 0.43 |
| MRSE(D) | -3.98 ± 1.90 | -4.16 ± 1.85 | 0.51 |
| T-CAT -topography-guided custom ablation treatment, SMILE –small incision lenticule extraction, D- diopters, MRSE – Mean Refractive Spherical Equivalent, aA P value < .05 was considered statistically significant. | |||
| Table 2. Safety and Efficacy profile | |||
| T-CAT (n = 200)% | SMILE (n = 200)% | Pa value | |
| Safety | 98% (196/200) | 94.5% (189/200) | 0.4273 |
| Efficacy | 97% (194/200) | 91.5% (183/200) | 0.3689 |
| T-CAT -topography-guided custom ablation treatment, SMILE – small incision lenticule extraction. aA P value < .05 was considered statistically significant. | |||
Table 3: Safety and Efficacy profile of two groups
| Table 4. Residual error | |||
| n | Mean(D) | Range(D) | |
| T-CAT | 2 | – 0.44 | – 0.37 to – 0.5 |
| SMILE | 8 | – 0.63 | – 0.25 to – 1.25 |
| T-CAT -topography-guided custom ablation treatment, D – diopters, SMILE – Small incision lenticule extraction. | |||
Table 5: Distribution of change in Snellen lines of Uncorrected distance visual acuity (UDVA).
| Table 6. Astigmatism correction | |||
| T-CAT(n=200) | SMILE (n =200) | Pa value | |
| n > 1 D Cylinder | 105 | 114 | 0.67 |
| Drop in CDVA (n) | 2 | 8 | 0.22 |
| Residual cylindrical error (n) | 0 | 5 | 0.06 |
| CDVA – corrected distance visual acuity, D – diopters, T-CAT -topography-guided custom ablation treatment, SMILE – Small incision lenticule extraction. aA P value < .05 was considered statistically significant. | |||
| Table 7. HOAs | ||||
| Procedure | Preoperative
(mean ± SD) |
Postoperative (mean ± SD) | Pa value | |
| TREFOIL | T-CAT | 0.0018 ± 0.18 | – 0.0096 ± 0.22 | 0.6328 |
| SMILE
|
0.0176 ± 0.15 | 0.0347 ± 0.19 | 0.4432 | |
| COMA 180 | T-CAT | 0.0311 ± 0.32 | – 0.0843 ± 0.52 | 0.0247 |
|
SMILE |
0.0458 ± 0.30 | – 0.1617 ± 0.55 | 0.0004 | |
| COMA 90 | T-CAT | – 0.0696 ±0.33 | – 0.2752± 0.43 | 0.0001 |
|
SMILE |
– 0.1152 ± 0.32 | – 0.5432 ± 0.58 | 0.0001 | |
| SPHERICAL ABERRATIONS | T-CAT | 1.1460 ± 0.21 | 1.9651 ± 0.48 | 0.0001 |
|
SMILE |
1.1603 ± 0.20 | 1.7260 ± 0.39 | 0.001 | |
| HOAs – Higher order aberrations, T-CAT -topography-guided custom ablation treatment, SMILE –Small incision lenticule extraction, SD – Standard deviation. aA P value < .05 was considered statistically significant. | ||||
| Table 8. Intergroup HOAs comparison | ||||||
| HOAs | Preoperative | Postoperative | ||||
| T-CAT
(mean ± SD)
|
SMILE
(mean ± SD) |
P value
|
T-CAT
(mean ± SD) |
SMILE
(mean ± SD) |
Pa value | |
| Trefoil | 0.0140 ± 0.16 | 0.0176 ± 0.15 | 0.8596 | – 0.0096 ± 0.22 | 0.0347 ± 0.19 | 0.1179 |
| Coma 180 | 0.0313 ± 0.32 | 0.0458 ± 0.31 | 0.7225 | – 0.0843 ± 0.53 | – 0.1617 ± 0.55 | 0.2484 |
| Coma 90 | -0.0649 ± 0.34 | -0.1152 ± 0.32 | 0.2406 | – 0.2742 ± 0.43 | – 0.5432 ± 0.58 | 0.0001 |
| Spherical Aberrations | 1.1460 ± 0.21 | 1.1603 ± 0.19 | 0.5905 | 1.9651 ± 0.48 | 1.7260 ± 0.39 | 0.0001 |
| HOA s– Higher order aberrations, T-CAT -topography-guided custom ablation treatment, SMILE –small incision lenticule extraction, SD – Standard deviation. . aA P value < .05 was considered statistically significant. | ||||||
Leave a Comment