
Dr. Hiranmoyee Das, D16233
Abstract
AIM-To investigate the independent association between the severity of diabetic retinopathy and glycosylated haemoglobin ( HbA1c) level.
Methods- This observational study was conducted at Diabetic clinic in a tertiary health center, from Jan 2011 to December 2016. Screening for retinopathy (& grading according to diabetic retinopathy disease severity scale) & HbA1c level done in each follow up visit of every patients registered with diabetes.
Results & observation- Patients were divided into 3 groups. HbA1c<7% was considered as controlled, 7-9% as poorly controlled and >9% uncontrolled. In controlled group (<7%) retinopathy was not develop, or developed at a much slower rate than in uncontrolled group (>9%).The progression rate of retinopathy was remarkably less for each (1%) reduction in the HbA1c. In some cases retinopathy was developed despite good HbA1c control, as the control in previous years was poor.
Summary- Dissemination of the above study findings may help in increasing the awareness of DR.
Key Words:Retinopathy, diabetic, HbA1c
Introduction
India is already being termed as the ‘‘diabetic capital of the world’’, with the number of patients with diabetes expected to rise from 40.9 million, at present, to a whopping 60.9 million by 2025.1Changing lifestyle, especially increasing weight caused by nutritional excess and decreasing physical activityplay important role for increasing of diabetes.2Currently, monitoring HbA1c levels is the gold standard forassessing average blood glucose concentration over threemonths 3.
All previous studies have explored the association of duration of diabetes, glycemic control, hypertension,dyslipidemia, obesity, proteinuria, pregnancy and socioeconomicstatus with the occurrence of diabetes retinopathy (DR). But the independentassociation between the severity of diabetic retinopathy and HbA1c level has not been explored in population-based studies.
The aim of the present study was to investigate the independent associations between the severity of diabetic retinopathy and HbA1c levelin Meghalaya, Northeast India.
Methods&materials
This observational study was conducted at Diabetic clinic in a 420 bedded multispecialty mission hospital (Nazareth Hospital, Shillong) tertiary health center, from Jan 2011 to December 2016.
This study employs both cross-sectional and prospective analyses.
In the cross-sectional analysis, data (HbA1c level and fundus finding) from the last examination of 2000 diabetic subjects were used.
In the prospective analysis, 300 diabetic subjects free of retinopathy at their first diabetic examination at which HbA1c was measured, were followed-up.
Screening for retinopathy (& grading according to diabetic retinopathy disease severity scale) & HbA1c level done in each follow up visit of every patients registered with diabetes.
HbA1c was measured (Bio-RadDiaSTATTM HbA1cReagentKit) by the liquid chroma- tography technique.
Results
Among the study population of 2300 patients with diabetes mellitus, those with retinopathy were found to be 989 (43%)Patients were classified into 3 groups.
- Individuals with DM and no evidence of DR(diabetic retinopathy) were classified as no-DR
- Diabetes having NPDR (non proliferative diabetic retinopathy) were classified as non-sight-threatening diabetic retinopathy (non –STDR) 704 (30.6%)
- Subjects withsevere NPDR, PDR(proliferative diabetic retinopathy) and CSME (clinically significant macular edema) as STDR 285 (12.4%)
Patients were divided into 3 groups depending on HbA1c value. HbA1c<7% was considered as controlled, 7-9% as poorly controlled and >9% uncontrolled.
40 %( 920)patients had HbA1c value of <7%, 26%(598) between 7% and 9%, and 34 %( 782) over 9%.
The frequency of diabetic retinopathy (both non-STDR andSTDR) was lowest in the controlled group of diabetes (14.8%, 136 out of 920 patients). In the uncontrolled group it was 52.4% (313 out of 598 patients)and highest (69.1%, 540 out of 782 patients) in the group with HbA1c concentrationsover 9%
As seen by the logistic regressionanalysis, in patients who had HbA1c value of 7%-9% there were significant relationship between DR and HbA1c levels.
Among 300 diabetic subjects without retinopathy at baseline,34 subsequently developed retinopathy duringfollow-up. Of 34 subjects withnew retinopathy, all had non-STDR.
Discussion
The inclusion of HbA1c in the screening protocols has gained significant importance, not only in the diagnosis and management of DM, but also in the onset and progression of DR. 4 It has been seen that compared to themeasurement of glucose levels, HbA1c assay is at least as good in defining the level of hyperglycemia at which the prevalence of DR increases.5,6Even short periods of higher HbA1c could have a sustained effect on worsening of retinopathydespite subsequent improvement in glycemic control .7
Researchers have conclusively proven, in the past, that once the retinopathy develops, there is no relationship between the level of glycemic control and the progression of DR, although the incidence of DR is significantly affected .8 Earlier reports showed that the prevalence of DR significantly increased at a HbA1c value between 6.0% and 7.0% 9. Later, a value of 6.5% was seen to be a cut-off which could detect at least moderate retinopathy 10. HbA1c of 6.5% has now been seen as sufficiently sensitive and specific to identify individuals who are at risk of developing DR.
Conclusion
The findings of our study reinforces the utility of monitoring the consistency in sugar control as it affects retinopathy development.This study probably, hasbeneficial aspects in targeted diabetic retinopathy screening programmes.. During each visit regular ophthalmological examinations with methodical documentation is needed in order to prevent blinding complications of diabetic retinopathy.
Reference
- Sicree R, Shaw J, Zimmet P. Diabetes and impaired glucose tolerance. In: Gan D, editor. Diabetes Atlas. International Diabetes Federation. 3rd ed., Belgium: International Diabetes Federation; 2006. p. 15–103.
- American Diabetes Association. Postprandial blood glucose. DiabetesCare 2001; 24: 775-8.
- Little RR. Recent progress in, HbA1c testing. Diabetes Care 2000; 23:265-6.
- Krishnamurty U, Steffes MW. Glycohemoglobin: a primarypredictor of the development or reversal of complicationsof diabetes mellitus. Clin Chem 2001;47:1157–65.
- Tapp RJ, Tikellis G, Wong TY, Harper C, Zimmet PZ, ShawJE. Longitudinal association of glucose metabolism withretinopathy. Diabetes Care 2008;31:1349–54.
- Sabanayagam C, Liew G, Tai ES, Shankar A, Lim SC,Subramaniam T, et al. Relationship between glycatedhaemoglobin and microvascular complications: is there anatural cut-off point for the diagnosis of diabetes.Diabetologia 2009 [Epub ahead of print]
- Hietala K, Waden J, Forsblom C, et al.HbA1c variability is associated with anincreased risk of retinopathy requiringlaser treatment in type 1 diabetes.Diabetologia 2013; 56: 737–745.
- Engerman RL, Kern TS. Progression of incipient diabetic retinopathy during good glycemic control. Diabetes 1987;36:808–12.
- The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183–97.
- Vistisen D, Colagiuri S, Borch-Johnsen K, the DETECT-2 Collaboration. Bimodal distribution of glucose is not universally useful for diagnosing diabetes. Diabetes Care 2009;32:397–403.

Figure 1 : CLASSIFICATION OF PATIENTS DEPENDING ON PRESENCE OF DR
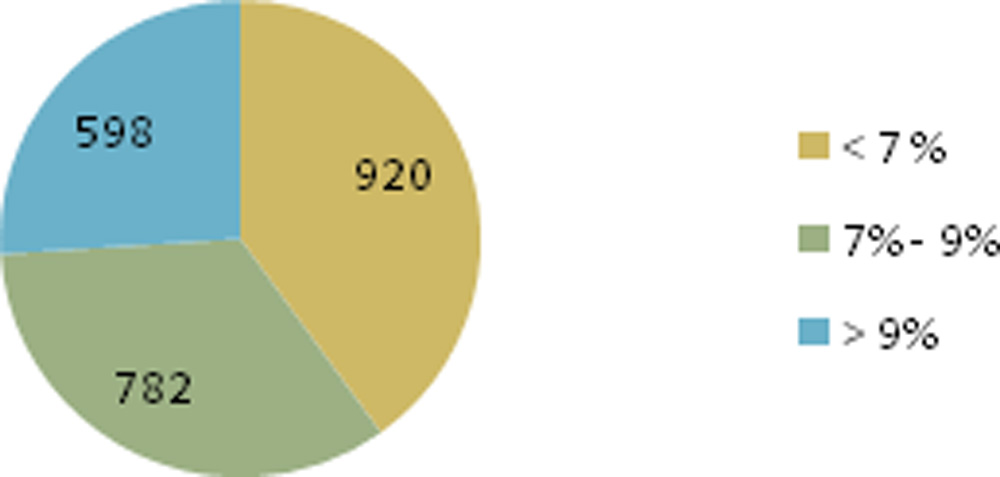
Figure 2: CLASSIFICATION OF PATIENTS DEPENDING ON HBA1C LEVEL
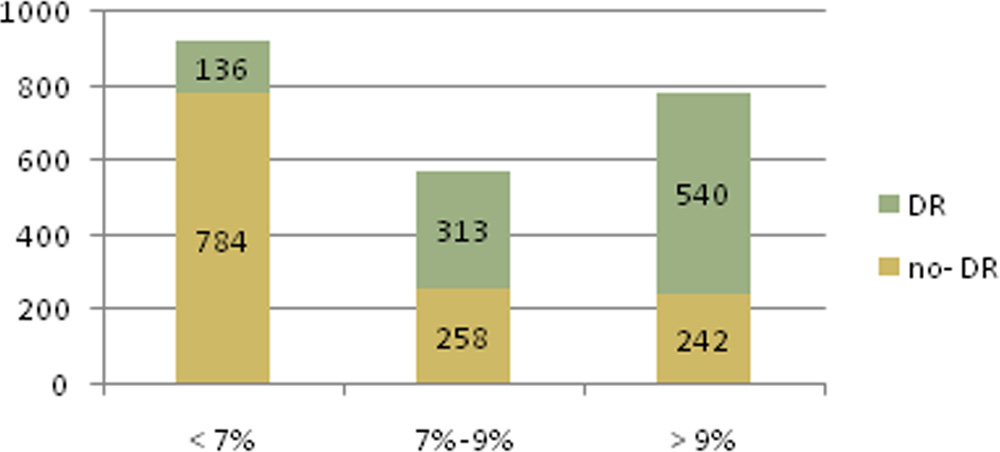
Figure 3: PRESENCE OF DR IN RELATION TO HBA1C LEVEL
Leave a Comment