
Dr. Sanitha Sathyan, S12939, Dr. Elizabeth Joseph, Dr. Meena Chembil Kakkitampara
ABSTRACT:
AIM: (1) To determine objective ocular torsion in comitant strabismus without oblique muscle dysfunction (CHS-WOMD). (2) To investigate the relationship of objective ocular torsion with the type and magnitude of comitant horizontal strabismus without oblique muscle dysfunction. (3) To investigate the relationship between objective ocular torsion and binocular status in patients with comitant horizontal strabismus without oblique muscle dysfunction.
MATERIALS AND METHODS: In this case-control study done at a tertiary care eye facility, 304 eyes of 152 subjects were prospectively enrolled. The sample consisted of 53 patients with comitant exotropia with 53 age matched normal controls and 23 patients with comitant esotropia with 23 age matched normal controls, between 4 and 30 years of age. All subjects underwent dilated fundus photography and the disc foveal angle (DFA) was calculated using Image J software. All photographs were also graded according to the presence of torsion as normal, extorsion or intorsion. The magnitude of the DFA was then compared between the respective case and control groups. Analysis was made between DFA and disease severity factors including amount of deviation, TNO near stereoacuity and duration of strabismus.
RESULTS: Mean disc–foveal angles of both exotropia and esotropia groups were significantly larger than those of the normal control groups (6.13 and 5.13 degrees, respectively; P < 0.05). Ocular torsion (either extorsion or intorsion) was seen in 82 (77%) patients in the exotropia group and in 26 (57%) in the esotropia group, whereas it was found in only 16 (13%) and 9 (20%) among their respective control groups (P < 0.05). The size of disc–foveal angle showed significant positive correlation with the amount of exotropia (P < 0.05). No significant correlation was found between the disc foveal angle and the amount of esotropia or with the degree of near stereoacuity (P < 0.05).
CONCLUSION: Significant ocular torsion exists even in patients with comitant horizontal strabismus, without oblique muscle dysfuntion. Both exotropes and esotropes exhibited significant amount of torsion when compared to control groups. The amount of torsion showed a significant correlation with the magnitude of exotropia. Further studies are needed to establish study the role of torsion in esotropia.
INTRODUCTION
Ocular torsion refers to rotation of eyeball about the line of sight which is the imaginary line connecting the eye with the fixation target. In general, the functions of eye movements include 1) the tracking of moving objects (pursuit), 2) the redirection of fixation to points of interest (saccades), 3) the stabilization of the retinal images and 4) the maintenance of correspondence of the image in both eyes. Of these functions, torsional eye movements are potentially important in the last two.1
Torsional alignment makes a substantial contribution to the precise control of the binocular motor correspondence, along with the horizontal and vertical alignment. This 3-dimensional coordination minimizes the retinal disparity of images.2,3,4
Small amounts of ocular torsion that fall within the range of sensory cyclofusion are often not problematic.5 When torsional disparity exceeds the cyclofusional limits, binocular visual function may be adversely affected.4 Up to 15° of torsional disparity can be fused by combining sensory fusion of 8°, (which is allowed by Panum’s peripheral fusional areas), and torsional motor fusion responses of 6 to 8°.6,7,8 Large degrees of monocular or binocular torsion may interfere with single binocular vision but may not yield with excellent stereoacuity.9, 10
Ocular torsion can be measured objectively or subjectively. Subjective torsion depends on the patient’s sensory adaptation the cyclodeviation, whereas objective torsion only demonstrates how far the eye is rotated anatomically away from the normal position itself.6, 11 The various subjective methods of measuring torsion include double Maddox rod test, Bagolini striated glasses test, Synoptophore test and Lancaster Red green test.12,13,14,15 However, subjective tests may be unreliable in measuring the full amount of abnormal torsion of the eyes, because of sensory adaptations which can take place, especially in young individuals. The objective methods are more reliable, as no artifacts are produced during the measurement process.16 These include slit–lamp biomicroscopy, indirect ophthalmoscopy and fundus photography.17,18,19 Out of these, fundus photography is simple, easily applicable and accurate and is the most widely used technique for measuring ocular torsion.19, 20
Certain amount of torsion has been identified even in normal individuals.16, 17, 19,20,21,22 A highest of up to 12.5 degrees of objective fundus torsion have been measured in normal subjects.16, 23 In addition, a number of studies also have been performed on ocular torsion in patients with cyclovertical strabismus.24,25,26,27 The role of ocular torsion in the meticulous control of binocular motor correspondence has been established by various major reports.2-4 The impact of torsion on binocularity, the horizontal fusional amplitudes, and stereopsis have been investigated by some studies.
However, occurrence of ocular torsion in patients with comitant horizontal strabismus has not been much studied. It is generally considered that horizontal strabismus is unrelated to cyclotorsion. The present study looks into the occurrence of ocular torsion in comitant horizontal strabismus including both exotropia and esotropia and its relationship with the disease severity factors.
AIM:
- To determine objective ocular torsion in comitant horizontal strabismus without oblique muscle dysfunction (CHS-WOMD)
- To investigate the relationship of objective ocular torsion with the type and magnitude of comitant horizontal strabismus without oblique muscle dysfunction
- To investigate the relationship between objective ocular torsion and binocular status in patients with comitant horizontal strabismus without oblique muscle dysfunction.
MATERIALS AND METHODS:
In this case control study, 152 patients with comitant horizontal strabismus without oblique muscle dysfunction were compared with normal age and sex matched controls.
Study design: Case control study
Sample size determination: was done based on the study by Shin et al,20 using the
Formula: n= Z 2 x p(1-p)/ M 2, where
n = sample size
Z = Z value (e.g. 1.96 for 95% confidence level)
P = population proportion (expressed as decimal)
M = Margin of Error at 5% (0.05)
The final sample was calculated as 152 patients (53 cases and 53 controls in exotropia ; 23 cases and 23 controls in esotropia)
Sampling technique: Simple random sampling (Random Number Tables)
Operational definitions:
Comitant Exotropia: A heterotropic deviation of the eye such that the visual axes diverge and the magnitude of deviation is the same in all directions of gaze, within physiologic limits and for a given fixation distance.
Comitant Esotropia: A heterotropic deviation of the eye such that the visual axes converge and the magnitude of deviation is the same in all directions of gaze, within physiologic limits and for a given fixation distance.
DFA: Angle formed by a line drawn tangential to the centre of the optic disc and the centre of the fovea.
Inclusion criteria:
For cases: Patients with CHS-WOMD between 4 – 12 years of age, with BCVA of at least 20/200 in the non – dominant eye.
For controls: Age and sex matched orthophoric subjects, without any other ocular abnormality and with best corrected visual acuity (BCVA) of 6/6.
Exclusion criteria:
For cases:
Oblique muscle involvement, vertical strabismus including pattern strabismus, restrictive strabismus, paralytic strabismus, sensory strabismus, any other significant ocular diseases (congenital cataract, history of retinopathy of prematurity, other congenital vitreoretinal disorders, history of ocular surgery, amblyopia, nystagmus, neurologic deficit, developmental delay and systemic/ genetic disorders were excluded.
For controls: Presence of any refractive error or significant ocular pathology.
Ethical concern: The study was approved by the Institutional Human Ethical Committee of Little Flower Hospital and Research Centre, Angamaly. The study followed the tenets of the Declaration of Helsinki and informed consent was obtained from the patients or their legal guardians (in case of children) enrolled in the study.
Procedure:
A total of 152 individuals were prospectively enrolled in the study. The enrolment of cases was performed using simple random sampling using random number tables. Simultaneous selection of an equal number of age and sex matched orthophoric controls was performed from the outpatients attending the centre during the study period.
After selection, participants were grouped as follows
Group A: Exotropia cases (n = 53)
Group B: Orthophoric controls (n = 53)
Group C: Esotropia cases (n = 23)
Group D: Orthophoric controls (n = 23)
Demographic details of all the subjects including medical records number, age and gender was recorded. All the groups were subjected to a complete ophthalmic examination according to the standard protocols in the following order:
The amount of deviation (angle of strabismus) was assessed using corneal reflex test and prism and cover test according to the standard protocols. To perform prism and cover test, a cover was placed alternately in front of each eye while the patient maintained fixation. The uncovered eye made a movement of redress in the direction opposite that of the deviation. The amount of the deviation was grossly estimated, and a prism of one strength lower than the estimated deviation was placed in the appropriate direction in front of one eye. To measure esotropia, the prism was placed base-out and for an exotropia it was placed base-in. The prism strength was progressively increased until the movement was neutralised. This was confirmed by adding the next higher prism to look for movement in the opposite direction. Extraocular movements were assessed in all the nine gaze positions.
Near stereoacuity was assessed by using TNO stereo-acuity test card (TNO Random dot stereo acuity test chart (Lam’eris Ootech 19th edition) at a distance of 40 cms. This test was done using a pair of red-green goggles and a test booklet. Each test plate in the booklet consists of a stereogram in which the half-images have been superimposed and printed in complementary colors (anaglyphs). The test plates, when viewed binocularly with red green spectacles by a normal subject, will elicit perception of an image in depth.
Best Corrected Visual Acuity (BCVA) was assessed using Log MAR chart (ETDRS Chart, Precision vision, USA. CAT No.2110, 2111). Anterior segment evaluation was done using a slit lamp biomicrosope and posterior segment evaluation by means of indirect ophthalmoscopy to rule out any ocular pathology.
Objective ocular torsion in both eyes was assessed using Zeiss Visucam Pro NM mydriatic retinal camera (Carl Zeiss Meditech, Dublin) by measuring the disc foveal angle.4 Patients were asked to fixate at an internal target to allow their eyes to be aligned in the primary position. The eyes were aligned with the side marks on the fundus camera to prevent inadvertent tilting of head and the fundus photos of both eyes of were taken by a single observer.
Measurement of Disc Foveal Angle (DFA): In the Powerpoint Presentation Software for Windows (Microsoft Corp, Redmond, WA) the insert tool was used to insert a circular shape (without any fill) and two lines (default thickness, 0.75 pt). These lines were oriented at 90˚ to each other within the circle. Precise orientation of the lines within the circle was facilitated by the marker dots on the circle. The horizontal line was then stretched along its length. (Figure: 1).
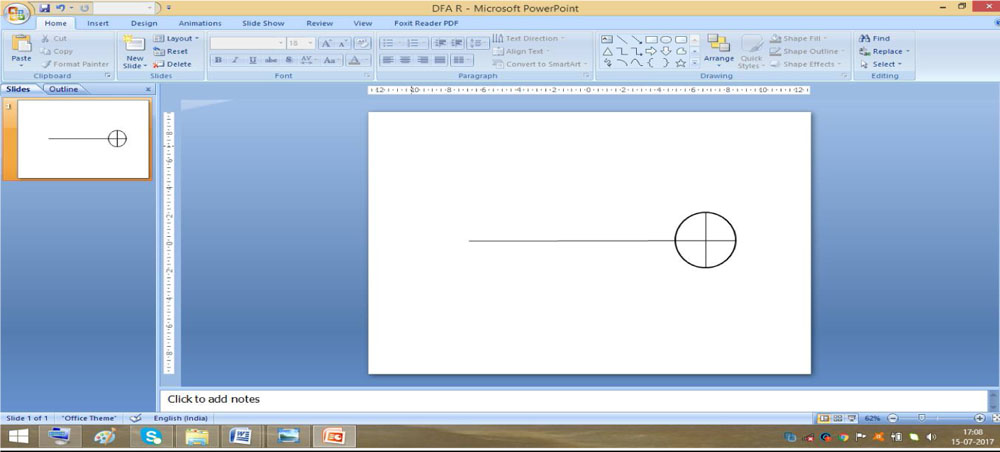
Figure:1 Powerpoint slide showing the circle with an extended horizontal line
After this, the fundus photograph was inserted into the slide and the circle was positioned on the optic disc such that the dimensions of the optic disc aligned exactly with that of the circle. In case of tilted discs, the circle was adjusted to match the tilt. A line was inserted and was made to pass through the center of the fovea and the center of the optic disc and the slide was then saved as a JPEG file. The image thus saved was then opened in the Image J Software (Laboratory for Optical and Computational Instrumentation, University of Wisconsin-Madison) and the angle measurement tool was used to measure the DFA (Figure:2).
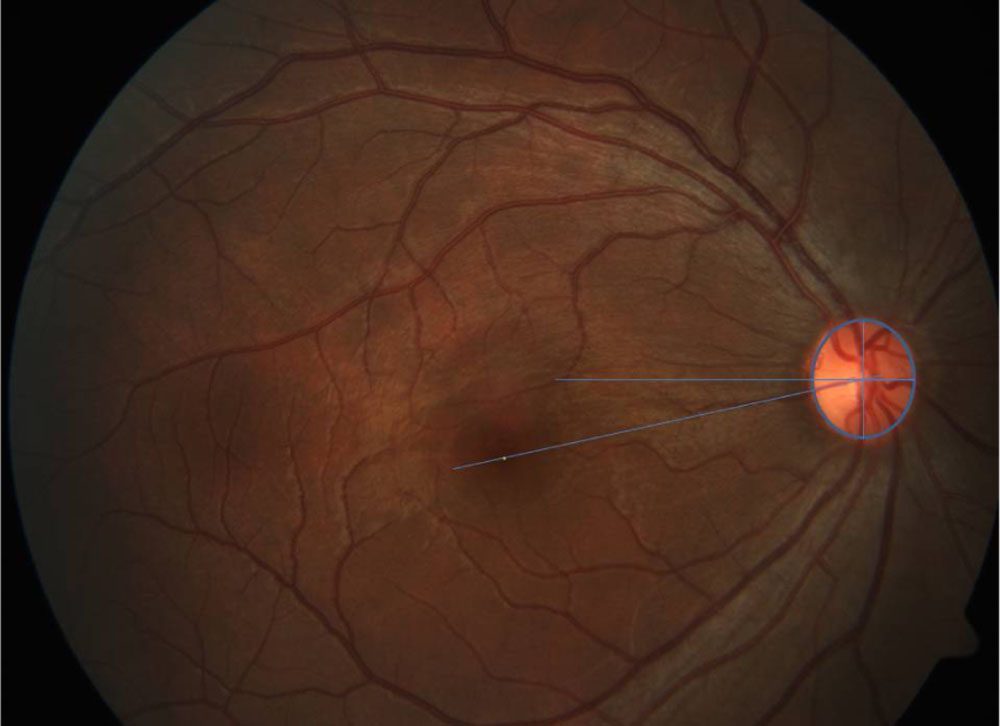
Figure 2: Image showing the ideal position of the circular shape for DFA measurement
Qualitative assessment of ocular torsion was also performed based on the location of fovea with respect to that of the optic disc and then the eyes were categorized as having extorsion, intorsion or normal. The eye was categorized as having intorsion when the fovea was located above the geometric center of the optic disc (figure 3), as extorsion when it was located below the inferior margin of the optic disc (figure 4) and as normal when the fovea was located in an area between the geometric center and inferior margin of the disc (figure 5).
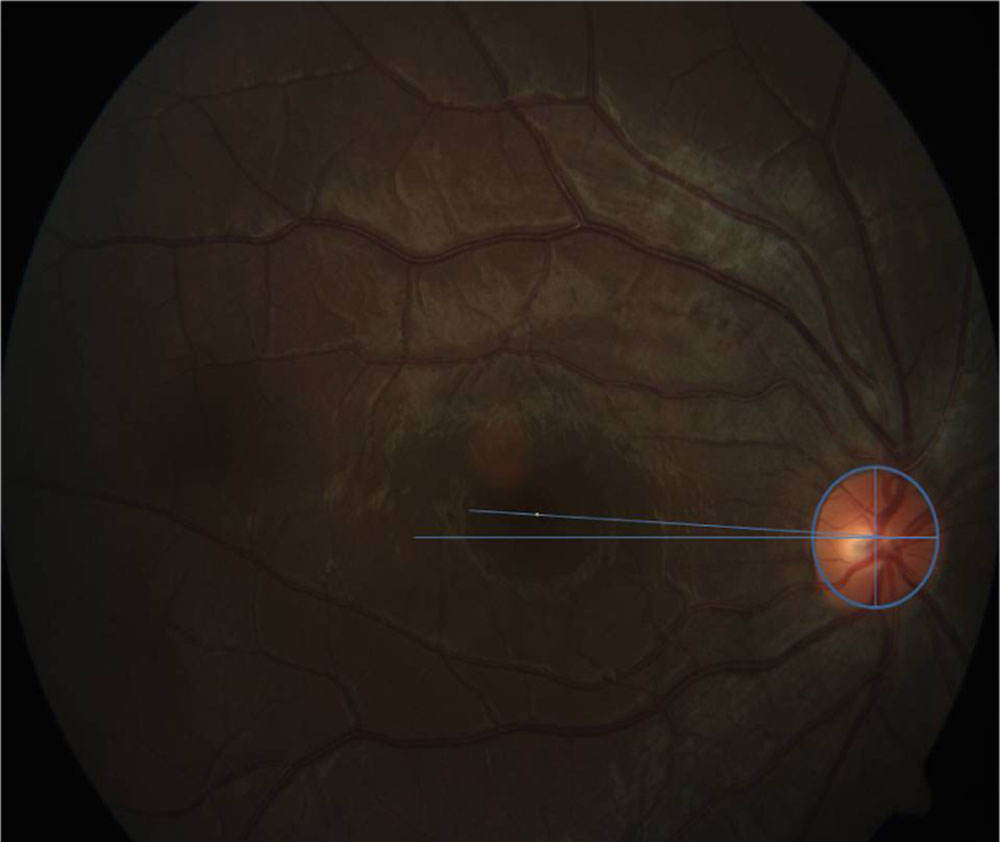
Figure 3: Right eye with intorsion
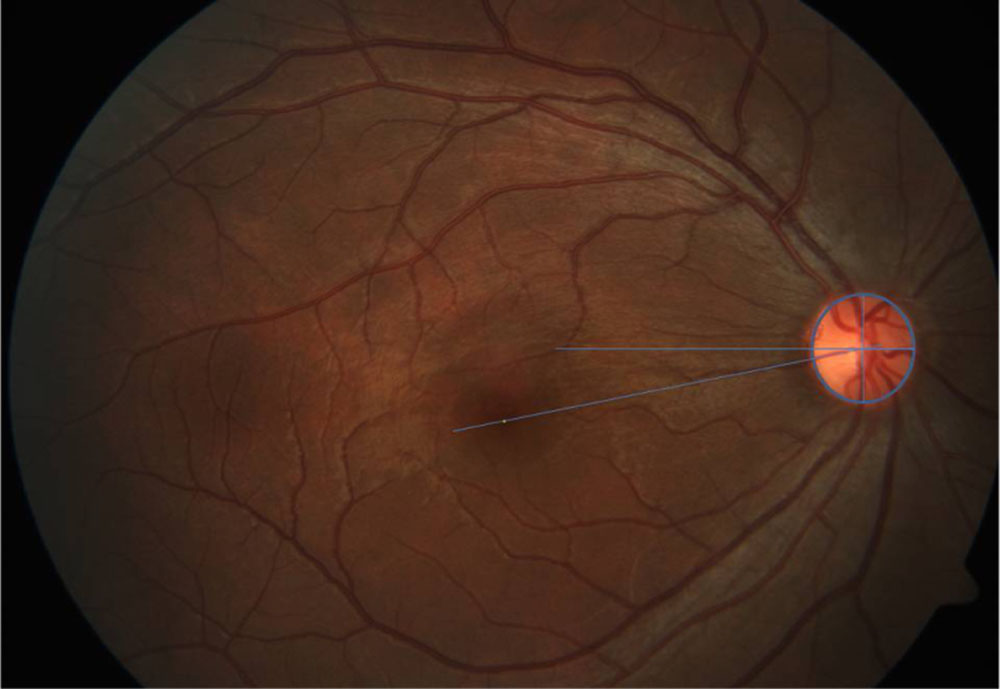
Figure 4: Right eye with extorsion
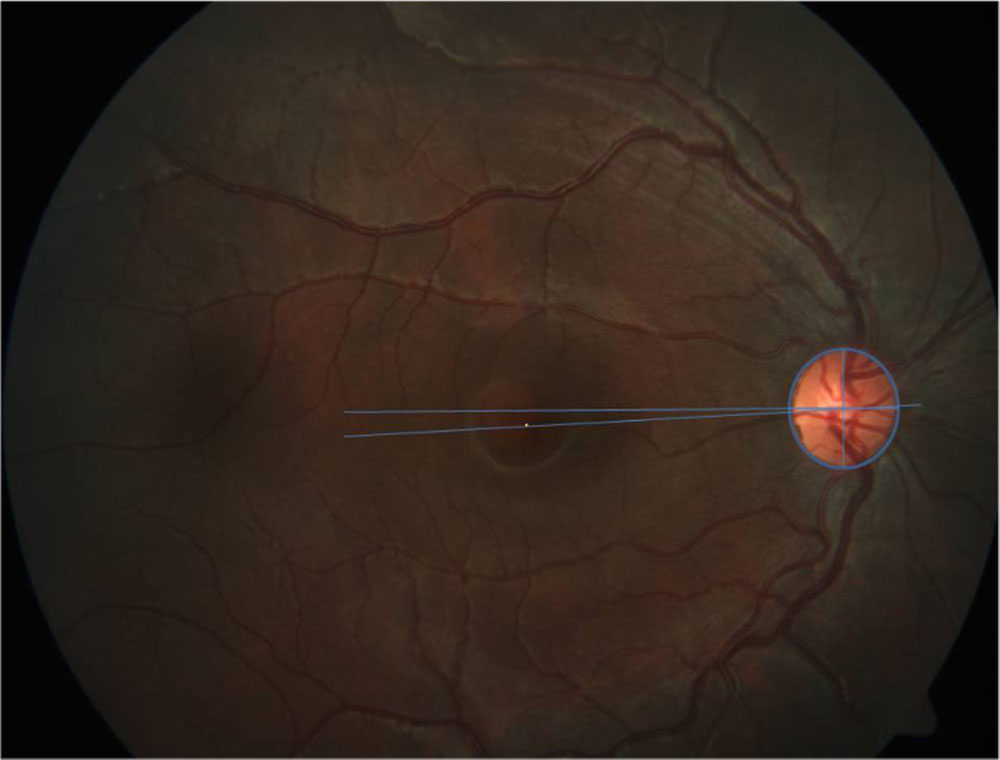
Figure 5: Right eye with normal alignment
STATISTICAL ANALYSIS:
Ocular torsion was compared between the cases and control groups and also between the subgroups of cases (exotropia and esotropia groups) using unpaired t-test and Chi Square test. Correlations were assessed between the amount of torsion and severity of strabismus in both the exotropia and esotropia case groups using Pearson correlation coefficient. All statistical analyses were performed using SPSS software for Windows version 20.0 (SPSS Inc, Chicago, Illinois, USA), and p value < 0.05 was considered significant.
RESULTS
A total of 152 subjects (304 eyes) were included in the final analysis. 76 strabismus patients (152 eyes) were enrolled as cases of which 53 (106 eyes) had comitant exotropia (XT) and twenty three (46 eyes) had comitant esotropia (ET). 152 (304 eyes) healthy age-matched individuals without any ocular – misalignment were recruited as controls for comparing with the respective case groups.
Age of the patients ranged from 4 to 30 years in the XT cases and their controls and 5 to 21 years in the ET cases and their controls. Demographic characteristics of the population are given in Table: 1.
Table 1: Demographic characteristics of the population
| Parameter | Exotropia cases | Exotropia controls | p value | Esotropia cases | Esotropia controls | p value |
| No: patients | 53 | 53 | – | 23 | 23 | – |
| Age (years) | 11.45±6.52 | 11.53±6.52 | 0.93 (t-test) | 9.65±4.81 | 9.72±4.62 | 0.87 (t-test) |
| Males | 21 (13.8%) | 26 (17.1%) | 0.72 (X2 test) | 8(5.3%) | 14 (9.2%) | 0.68 (X2 test) |
| Females | 32 (21%) | 27 (17.8%) | 0.66 (X2 test) | 15(9.9 %) | 9 (5.9%) | 0.57 (X2 test) |
| Spherical Equivalent (D) | -0.47±0.84 | -0.23±0.54 | 0.59 (t-test) | -0.39±0.11 | -0.15±0.45 | 0.34 (t-test) |
| PBCT deviation (PD) | 27.64±9.63 | – | – | 33.15±14.47 | – | – |
| Duration of strabismus (years) | 7.18 ± 6.81 | – | – | 6.23 ± 5.18 | – | – |
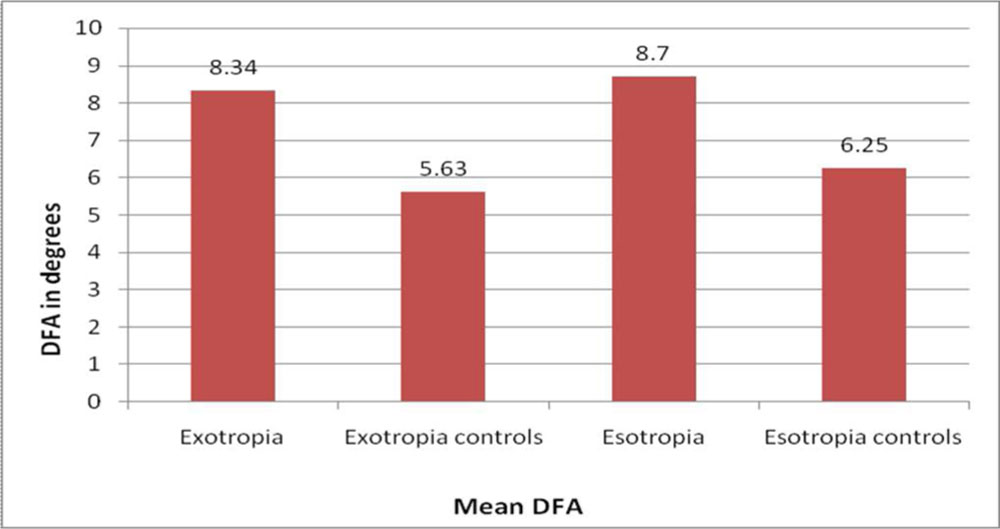
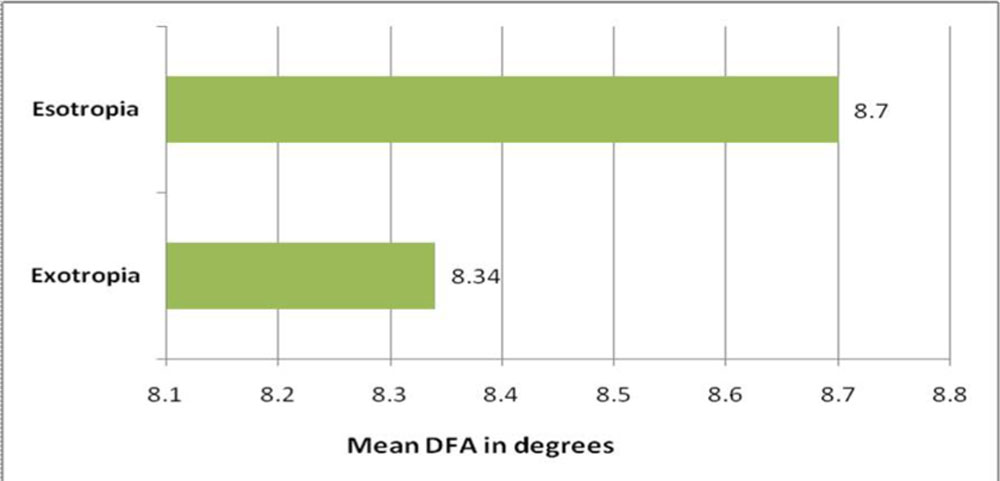
Distribution of DFA among patients and controls is given in table:2 and fig:6
Table 2: Distribution of disc-foveal angle among the groups
| Disc Foveal Angle (degrees) | |||||
| Group | n | Mean | S.D | Min | Max |
| Exotropia | 53 | 8.34 | 5.7 | -14.833 | 25.073 |
| Exotropia controls | 53 | 5.63 | 3.95 | -4.863 | 16.681 |
| Esotropia | 23 | 8.7 | 6.3 | -14.855 | 20.059 |
| Esotropia controls | 23 | 6.25 | 5.13 | -4.856 | 19.422 |
Figure 6: Distribution of disc-foveal angle among the groups
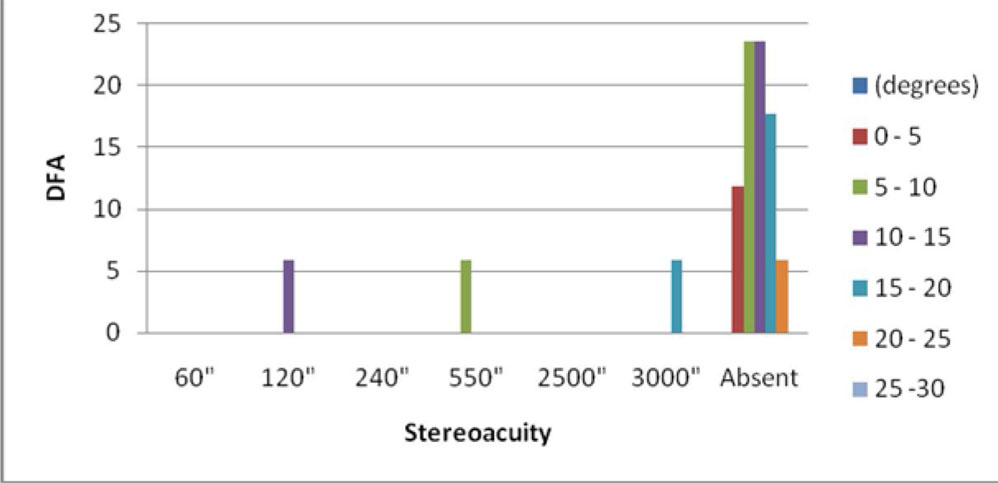
Near stereopsis was analyzed as a function of DFA among the exotropes and esotropes. This is depicted in the tables: 3, 4 and the figures: 7, 8.
Table 3: Distribution of exotopes according to the status of Binocular single vision
| DFA
(degrees) |
60″ | 120″ | 240″ | 550″ | 2500″ | Absent |
| 0 – 5 | 2
(4.17%) |
1 (2.08%) | 1 (2.08%) | nil | nil | nil |
| 5 – 10 | 4
(8.33%) |
4 (8.33%) | nil | 3 (6.25%) | 1 (2.08%) | 3
(6.25%) |
| 10 – 15 | 7 (14.58%) | 2 (4.17%) | nil | 1 (2.08%) | nil | 7 (14.58%) |
| 15 – 20 | 4
(8.33%) |
2 (4.17%) | nil | 1 (2.08%) | nil | 2
(4.17%) |
| 20 – 25 | 2
(4.17%) |
1 (2.08%) | nil | nil | nil | nil |
Figure7: Distribution of exotopes according to the status of Binocular single vision
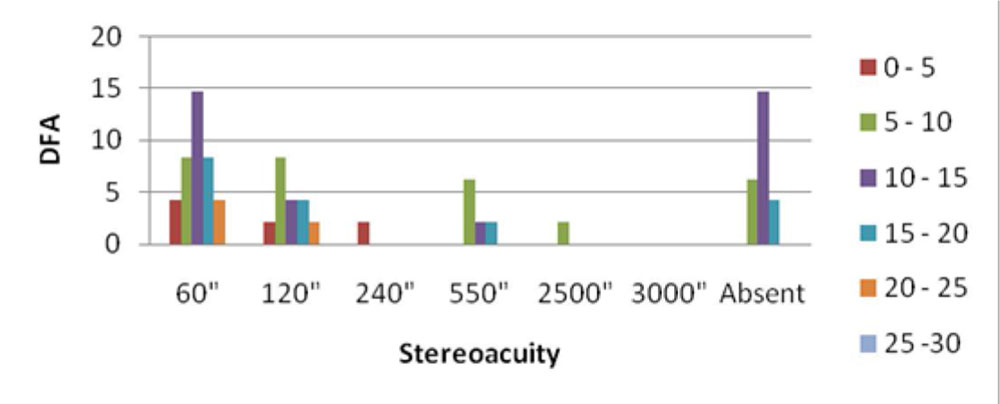
Table 4: Distribution of esotopes according to the status of Binocular single vision
| DFA
(degrees) |
60″ | 120″ | 240″ | 550″ | 3000″ | Absent |
| 0 – 5 | nil | nil | nil | nil | nil | 2 (11.76%) |
| 5 – 10 | nil | nil | nil | 1 (5.88%) | nil | 4 (23.53%) |
| 10 – 15 | nil | 1 (5.88%) | nil | nil | nil | 4 (23.53%) |
| 15 – 20 | nil | nil | nil | nil | 1 (5.88%) | 3 (17.65%) |
| 20 – 25 | nil | nil | nil | nil | nil | 1 (5.88%) |
Figure 8: Distribution of esotopes according to the status of Binocular single vision
Comparison of mean DFA between Exotropia cases and controls:
The mean DFA of exotropia cases was 8.34±5.7 degrees and that of the exotropia controls was 5.63±3.95 degrees. The result of analysis using unpaired t-test is shown in table: 5.
Table 5: Comparison of DFA between Exotropia cases and Exotropia Controls
| Group | Mean | S.D. | n | Mean
Difference |
df | t | p-value |
| Exotropia | 8.34 | 5.7 | 106 | 2.71 | 210 | 4.07 | p < 0.05* |
| Exotropia Controls | 5.63 | 3.95 |
There was a significant difference in the mean DFA of exotropia cases and controls (p<0.05), with higher DFA among the exotropia cases.
Comparison of mean DFA of Esotropia cases and controls:
The mean DFA of esotropia cases was 8.7±6.3 degrees and that of esotropia controls was 6.25±5.13 degrees.(Table:6)
Table 6: Comparison of DFA between Esotropia cases and Esotropia Controls
| Group | Mean | S.D. | n | Mean
Difference |
df | t | p-value |
| Esotropia | 8.7 | 6.3 | 46 | 2.4 | 90 | 2.05 | p < 0.05* |
| Esotropia Controls | 6.25 | 5.13 |
There was a significant difference in the mean DFA of esotropia cases and controls (p<0.05), with higher DFA among the esotropia cases.
The mean DFA of esotropia cases was 0.36 degrees higher than that of exotropia cases. However, this was not statistically significant (p=0.75). Table: 7 and Fig: 9 depict the mean disc-foveal angle measurements among exotropia and esotropia cases.
Table 7: Comparison of DFA between exotropia ande esotropia cases
| Group | Mean | S.D. | N | Mean
Difference |
df | t | p-value |
| Exotropia | 8.34 | 5.7 | 152 | 0.36 | 150 | 0.32 | 0.753 |
| Esotropia | 8.7 | 6.3 |
Fig 9: Comparison of mean DFA between exotropia and esotopia cases
Ocular torsion was compared between the groups and classified as normal, excyclotorsion and incyclotorsion depending upon the position of the macula in relation to the optic disc, analyzed using Image J software from fundus photographs.
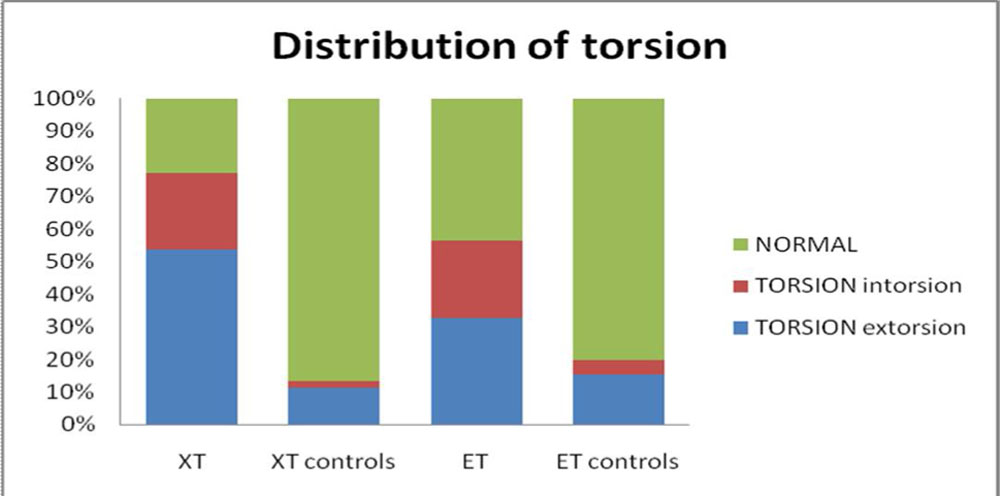
The distribution of eyes according to torsion is given in Table: 8 and Figure:10.
Table 8: The distribution of eyes according to the torsion measured
| Category | XT | XT controls | ET | ET controls |
| Normal | 24 (22.64%) | 92 (86.79%) | 20 (43.48%) | 37 (80.43%) |
| Intorsion | 25 (23.58%) | 2 (1.89%) | 11 (23.91%) | 2 (4.35%) |
| Extorsion | 57 (53.77%) | 12 (11.32%) | 15 (32.61%) | 7 (15.22%) |
Figure 10: The distribution of eyes according to the torsion measured
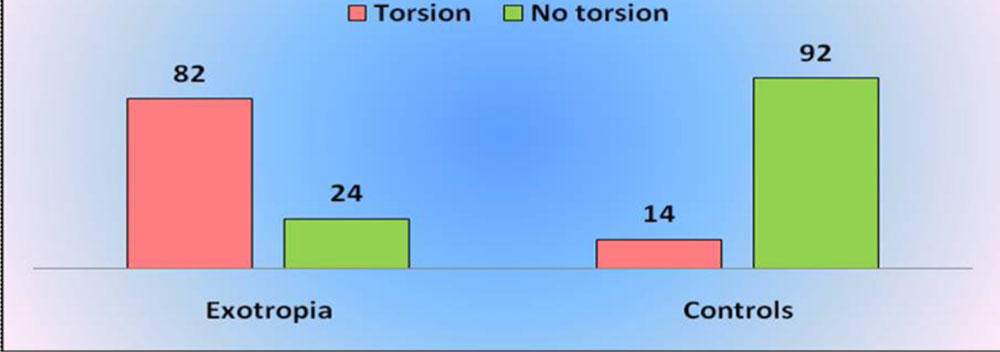
Chi Square test indicated significant torsion in exotropia cases when compared to controls (p<0.05) (Table: 9, Figure: 11)
Table 9: The distribution of eyes among exotropia cases and controls according to the torsion measured
| Torsion | No torsion | Total | c2 | df | p-value | |
| Exotropia | 82 | 24 | 106 | 88.03 | 1 | < 0.05* |
| Controls | 14 | 92 | 106 | |||
| Total | 96 | 116 | 212 |
Figure 11: The distribution of eyes among exotropia cases and controls
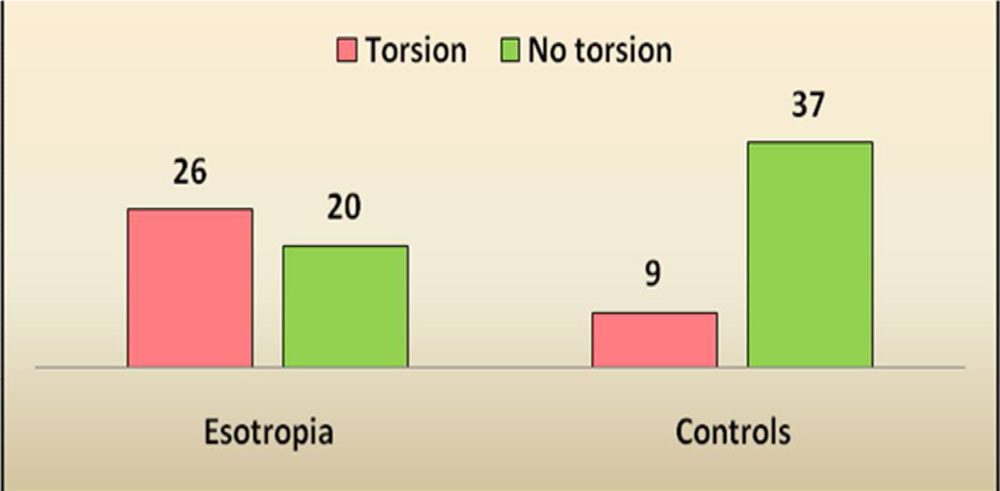
Chi Square test indicated significant torsion in esotropia cases when compared to controls (p<0.05) (Table: 10, Figure: 12)
Table 10: The distribution of eyes among esotropia cases and controls according to the torsion measured
| Torsion | No torsion | Total | c2 | df | p-value | |
| Esotropia | 26 | 20 | 46 | 13.33 | 1 | < 0.05* |
| Controls | 9 | 37 | 46 | |||
| Total | 35 | 57 | 92 |
Figure 12: The distribution of eyes among esotropia cases and controls
cases using Pearson correlation coefficient. Average of the DFA of the two eyes and average of distance and near deviation was used for the analysis. (Table: 11, Figure: 13).
Table 11: Correlation between average DFA and deviation in exotropia cases
| Variables | n | Pearson Correlation | Significance
(p-value) |
| Average DFA and devaiation | 53 | 0.59 | < 0.05* |
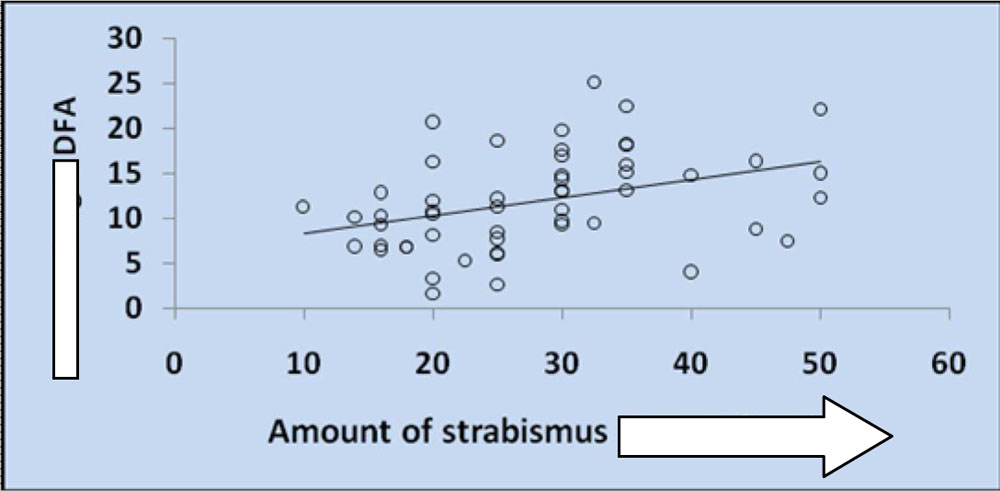
This indicates that there is a significant positive correlation between average DFA and average deviation measured using PBCT in the exotropia cases.
Fig 13: Correlation between average DFA and deviation in exotropia cases
Similarly, correlation between the DFA and the amount of deviation was analyzed among the esotropia cases (Table: 12, Figure: 14).
Table 12: Correlation between average DFA and deviation in esotropia cases
| Variables | n | Pearson Correlation | Significance
(p-value) |
| Average DFA & deviation | 23 | 0.06 | 0.786 |
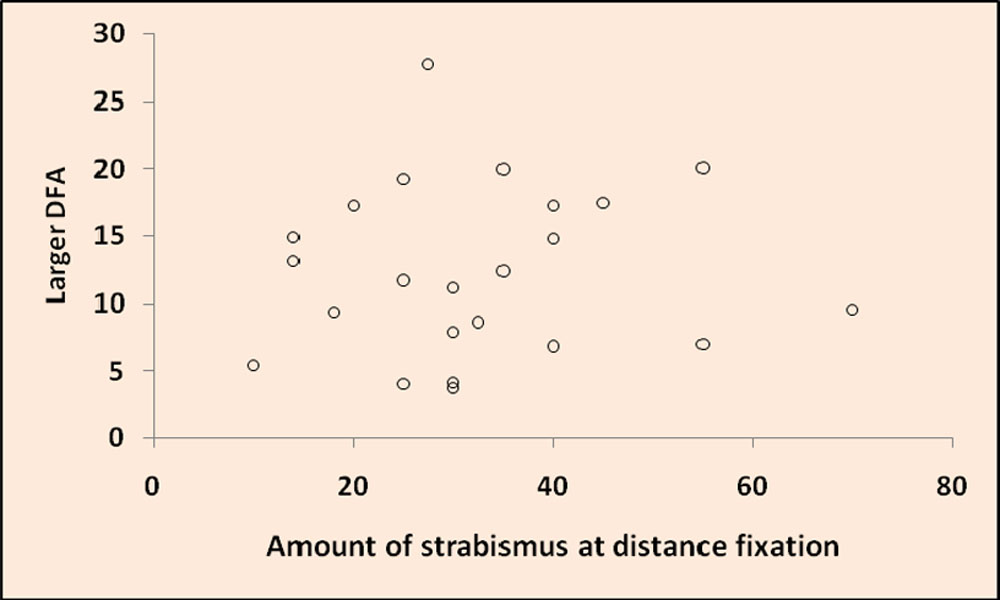
This indicates that there was no significant correlation between average DFA and average deviation measured using PBCT in the Esotropia cases (p=0.79).
Figure 14: Correlation between average DFA and deviation in esotropia cases
There was no significant correlation between average DFA and stereopsis among exotropes (p=0.84) or esotropes (p= 0.70), with duration of strabismus (p= 0.6 )
DISCUSSION:
Ocular torsion in normal individuals has been variably reported previously.28, 29, 30, 31, 32 The findings in some of the studies are as follows:
| Study | Degree of torsion in normal individuals |
| Bixenman WW & von Noorden GK28 | 6.1 |
| Kothari MT et al 29 | 7.030 |
| Jethani J et al 30 (5-15 years) | 12.5 |
| Lee DH et al 31 | 6.39 |
| Lee HJ & Lim KH 32 | 6.50 |
Besides, several studies have been performed on patients with strabismus, mostly in cases of cyclovertical strabismus.24,25,26,27
The mean DFA obtained in our XT and ET control groups were 5.63 ± 3.95 degrees and 6.25 ± 5.13 degrees respectively and matched with the observations made in previous studies.16,28 A study conducted by Shin et al20 noted the presence of significant ocular torsion in patients with intermittent exotropia. Also, the amount of ocular torsion was found to positively correlate with the stereoacuity. Nevertheless, no probe has so far been made regarding the role of ocular torsion in esotropia.
Shin et al20 had documented that ocular torsion was present in one third of the subjects with intermittent XT. To the best of our knowledge, there are no previous studies describing the presence of torsion and its role in CHS-WOD comprising of esotropias and exotropias. Our study proves the occurrence of significant ocular torsion even in esotropes and exotropes without oblique muscle dysfunction. In contrast to the results of Shin et al,20 torsion was present in three fourth of the patients with comitant XT in our sample and in more than half of the patients with comitant ET. This difference could be due to the inclusion of patients with all forms of comitant strabismus irrespective of their degree of fusional control, whereas Shin et al20 had recruited only intermittent exotropes.
The average disc foveal angle of our patients with comitant XT was 8.34 ± 5.7 degrees which was significantly larger than that of the control group. Also, the 23 patients with comitant ET had a significantly higher average DFA of 8.7 ± 6.3 degrees than that of their normal controls. Our data showed high variability in terms of DFA, especially in the groups with strabismus (-14.83 to 25.07 degrees in XT and -14.86 to 20.06 degrees in ET), which could be attributed to the variable degree of fusional control present in patients with intermittent strabismus.
An explanation for the presence of torsion in horizontal strabismus may be derived from the mechanical aspects of the oblique muscles. When the eye adopts a markedly exotropic or esotropic position, the oblique muscles become slack. Over time, they may become shortened, causing tonic imbalance of the oblique muscles, which eventually leads to ocular torsion in primary position, even in horizontal strabismus without clinical oblique overaction.33
To evaluate the relationship of torsion with the severity of strabismus, correlation was checked between the amount of ocular torsion and stereopsis as well as between the former and the duration of strabismus. However there was no correlation between them in our study both in exotropes and in esotropes. Several studies have reported an association between amount of ocular torsion and stereopsis among normal subjects.4,20,34 This was not reflected in our sample of CHS-WOD. But an interesting observation seen in our sample was that patients with good stereoacuity had large disc foveal angles and vice versa. This could be attributed to the fact that stereopsis largely depends on the highly variable fusional control in patients. As expected, among esotropes, stereopsis was poor in more than three fourth of the patients in spite of good visual acuity and exotropes had better stereoacuity. This result could be explained by the better fusional control present in exotropes when compared to esotropes. On the other hand, an increased tendency to fuse (irrespective of the magnitude of fusional control) during the testing procedure, presence of any subtle suppression associated and the higher age range could also have confounded our results.
In addition to stereopsis, correlation between the duration of strabismus and disc foveal angle was also analyzed to assess the effect of the torsion on the severity of the disease. There was no significant correlation even in these parameters. One possible explanation for this finding could be the lack of accuracy in the recorded duration of strabismus as they were mainly based on recall.
The magnitude of deviation of strabismus among exotropia cases showed a positive correlation with the average disc foveal angle. However, there was no such correlation among esotropia cases. A plausible explanation for this difference could be ascribed to the direct relationship between the amount of deviation of strabismus and age. The range of presenting age among esotropia cases was lower (5 to 21 years) as compared to that of the exotropia cases (4 to 30). So a significant positive correlation between the magnitude of deviation of strabismus for both distance and near and the larger disc foveal angle among esotropia cases could not be made out.
Our study needs to be viewed in light of its limitations too. First, we did not measure subjective ocular torsion. Objective measurement of torsion is regarded to be more valid and reliable compared to subjective torsional measurement because subjective torsion is affected by fixational or fusional cyclovergence stimuli.17 Comparison of objective and subjective torsion may give additional information, especially in patients with fusion. However, we could not do so because our enrolled subjects were mostly children and were uncooperative for the subjective torsion testing. Secondly, we were unable to attain the desired sample size for the esotropia case group. This was due to the fact that most of the patients with esotropia either presented before the age of four years or had already undergone surgical correction. Finally, in our study, the duration of strabismus was determined based on recall, which was prone to error.
Inspite of its limitations, our study proves that significant ocular torsion exist even in comitant horizontal strabismus, without oblique muscle dysfunction. This is contradicts the general notion that torsion in strabismus occurs only in the presence of oblique muscle involvement, pattern strabismus or associated refractive errors. However, we could not prove an association between near stereoacuity and torsion in the present study. The reasons behind this have been discussed previously. This calls for more standardised designs considering fusional control in intermittent deviations and inclusion of subjective torsion inorder to elucidate fully the significance of our observations.
CONCLUSION:
Significant ocular torsion is present in patients with comitant horizontal strabismus, without clinical oblique muscle dysfunction. Both exotropes and esotropes exhibit considerable amount of torsion as compared to age and sex matched controls. More studies need to be performed to establish any correlation between the amount of torsion and the clinical severity in horizontal strabismus.
REFERENCES:
1. L.J. van Rijn, Torsional Eye Movements in Humans, Foundation for Eyelids, The Rotterdam Association of Interests, The Prof. Dr. H.J. Flieringa Stichting Foundation, The Prof. Dr FIieringa-Houet Foundation and Skalar Medical B.V.2.
2. Guyton DL. Ocular torsion reveals the mechanisms of cyclovertical strabismus. Invest Ophthalmol Vis Sci 2008;49(3): 847–857.3.
3.Tweed D. Visual-motor optimization in binocular control. Vision Res 1997;37(14):1939–1951.4.
4.Georgievski Z, Sleep M, Koklanis K. Simulated torsional disparity disrupts horizontal fusion and stereopsis. J AAPOS 2007;11(2):120–124.5.
5.von Noorden GK: Binocular Vision and Ocular Motility. Theory and Management of Strabismus. 5th ed. St Louis: C.V. Mosby; 1996. p. 370.6.
6.Guyton DL. Ocular torsion: sensorimotor principles. Am Orthopt J 1987;37:13-20.7.
7.Crone RA, Everhard-Halm Y (1975) Optically induced eye torsion. I. Fusional cyclovergence. Graefe’s Arch Clin Exp Ophthalmol 195 :231-2398.
8.Kertesz AE, Sullivan MJ (1978) The effect of stimulus size on human cyclofusional response. Vision Res 18:567-571.9.
9.Brodsky MC: Do you really need your oblique muscles? Adaptations and exaptations. Arch Ophthalmol 2002; 120:820–828.10.
10.Porrill J, Ivins JP, Frisby JP: The variation of torsion with vergence and elevation. Vis Res 1999; 39:3934–3950.11.
11.Morton GV, Lucchese NJ, Kushner BJ. The role of fundoscopy and fundus photography in strabismus diagnosis. Ophthalmology 1983;90(10):1186–119112.
12.Kushner BJ, Hariharan L. Observations about objective and subjective ocular torsion. Ophthalmology 2009;116(10): 2001–2010.13.
13.Ruttum M, von Noorden GK. The Bagolini striated lens test for cyclotropia. Doc Ophthalmol 1984; 58:131.14.
14.Sood GC, Sen DK. Measurement and diagnosis of cyclodeviation by after-image method. Br J Ophthalmol. 1970;54:340–1.
15..Arthur L. Rosenbaum, Alvina Pauline Santiago. Clinical Strabismus Management: Principles and Surgical Techniques. W. B. Saunders Company, Philadelphia, 60-62.
16. Lee HJ, Lim KH. The range of ocular torsion in mass screening. J Korean Ophthalmol Soc 2005;46(10):1684–1689.17.
17.Kushner BJ. Effect of ocular torsion on A and V patterns and apparent oblique muscle overaction. Arch Ophthalmol 2010; 128(6):712–718.18.
18.Kraft SP, O’Reilly C, Quigley PL, Allan K, Eustis HS. Cyclotorsion in unilateral and bilateral superior oblique paresis. J Pediatr Ophthalmol Strabismus 1993;30(6): 361–367.19.
19. Roh YR, Hwang JM. Comparison of subjective and objective torsion in patients with acquired unilateral superior oblique muscle palsy. Br J Ophthalmol 2011;95(11):1583–1587.20.
20. Shin K H, Lee H J, Lim H T. Ocular Torsion Among Patients With Intermittent Exotropia: Relationships With Disease Severity Factors. Am J Ophthalmol, 2013; 155 (1): 177-182.21.
21.Sharma P, Prasad K, Khokhar S. Cyclofusion in normal and superior oblique palsy subjects. J Pediatr Ophthalmol Strabismus 1999; 36:264-70.22.
22.Yagasaki Y, Konda N, Nonura H. Stereoscopic perception in the background of cyclofusional stimuli. Invest Ophthalmol Vis Sci 1994;35(Suppl):2109.
23.Yagasaki Y, Konda N, Nonura H. Stereoscopic perception in the background of cyclofusional stimuli. Invest Ophthalmol Vis Sci 1994;35(Suppl):2109.
24. Kushner BJ. Effect of ocular torsion on A and V patterns and apparent oblique muscle overaction. Arch Ophthalmol 2010; 128(6):712–718.25.
25.Kraft SP, O’Reilly C, Quigley PL, Allan K, Eustis HS. Cyclotorsion in unilateral and bilateral superior oblique paresis. J Pediatr Ophthalmol Strabismus 1993;30(6): 361–367.
26. Roh YR, Hwang JM. Comparison of subjective and objective torsion in patients with acquired unilateral superior oblique muscle palsy. Br J Ophthalmol 2011;95(11):1583–1587.
27.Sharma P, Prasad K, Khokhar S. Cyclofusion in normal and superior oblique palsy subjects. J Pediatr Ophthalmol Strabismus 1999; 36:264-70.
28.Bixenman WW, von Noorden GK. Apparent foveal displacement in normal subjects and in cyclotropia. Ophthalmology 1982;89(1):58–62. Yagasaki Y, Konda N, Nonura H. Stereoscopic perception in the background of cyclofusional stimuli. Invest Ophthalmol Vis Sci 1994;35(Suppl):2109.
29. Kothari MT, Venkatesan G, Shah JP, Kothari K, Nirmalan PK. Can ocular torsion be measured using the slitlamp biomicroscope? Indian J Ophthalmol. 2005; 53:43–7.
30. Jethani J, Seethapathy G, Purohit J, Shah D. Measuring normal ocular torsion and its variation by fundus photography in children between 5–15 years of age. Indian J Ophthalmol 2010;58(5): 417–419.
31. Lee DH, Lee SJ, Park SH. Ocular torsion in normal Korean population. J Korean Ophthalmol Soc 2004;45(5):797–802. 32. Lee HJ, Lim KH. The range of ocular torsion in mass screening. J Korean Ophthalmol Soc 2005;46(10):1684–1689.
33.Jampolsky A. Surgical leashes, reverse leashes in strabismus surgical management. In: Symposium on Strabismus: Transactions of the New Orleans Academy of Ophthalmology. St. Louis, MO: CV Mosby; 1978: 244 –245.
34.Brodsky M. Torsion and stereopsis. Am Orthopt J 2002;52:89-94
Leave a Comment