
Dr. Natasha Radhakrishnan, R14418, Dr. Gopal S Pillai
Abstract
Anti VEGFs are being increasingly used in Retinopathy of prematurity(ROP).This study prospectively analysed a small group of babies with stage 3 ROP with plus disease in Zone 1 and Zone 2 who were treated with intravitreal antiVEGF injections.The babies were followed up weekly till full vascularisation and laser therapy given in cases of recurrence. The mean age to full vascularisation and the incidence of recurrence and retreatment with laser was computed. It was found that anti VEGF injections are an effective treatment in the management of both zone 1 and zone 2 posterior ROP and these babies require a much longer follow up than others.
Background and rationale.
The gold standard for treatment for ROP is now laser therapy using the indirect ophthalmoscope and is given in type 1 ROP1.However, many adverse events and recurrence have been noted with laser treatment especially in more posterior ROP(zone 1 and posterior zone 2) including destruction of the avascular retina, traction membranes and unprevented vision loss.2 Recent reports suggest that anti VEGF treatment is effective and promotes full vascularisation of the retina3,4,5 Intravitreal anti VEGF can be administered at the bedside in the NICU while laser treatment requires specialised equipment and trained personnel for administration6. Since there is a marked paucity of studies of anti VEGF in ROP from our country, this study attempts to bridge this lacuna.
Aims of the study
Primary-To study the results of intravitreal anti VEGF injection in babies with Zone 1 and Zone 2 stage 3 ROP with plus in terms of ROP regression and recurrence of ROP .
Secondary
- To study the time taken for full vascularisation of the retina after anti VEGF injection.
- To study the recurrence rate requiring laser treatment after anti VEGF injection in these babies.
Materials and Methods
The study was conducted at Amrita Institute of medical sciences in the period 2014 January to 2016 December. All preterm babies <2500g weight and <35 weeks PCA were screened by a retina specialist using the indirect ophthalmoscope and 28D lens after dilatation with diluted tropicamide plus eyedrops(0.8% tropicamide and 5% phenylephrine) at 4 weeks post delivery or 34 weeks PCA whichever was earlier. The ICROP classification was followed for documentation. 31 infants with stage 3 zone 1,stage 2 zone 1 with plus or stage 3 zone 2 posterior were included in the study. All the infants underwent intravitreal injection of Ranibizumab(0.025ml) or Bevacizumab (625 mg in 0.025ml) after obtaining fitness from the treating neonatologist .All injections were given by a single retinal surgeon. The injections were done in the NICU under aseptic precautions and topical anaesthesia with paracain at 1mm from the limbus inferotemporally. The choice of which anti VEGF injection was made by the parents after the pros and cons of each were explained. A written ,informed consent was taken both for the procedure and for the drug used. Ethical and scientific committee clearance was obtained for the study .
The babies were followed up 3 days and 1 week after the procedure for regression and any ocular adverse events and then weekly till full vascularisation by the ROP specialist. They were closely monitored for systemic adverse events by the treating neonatologist .Immediate adverse events(-within 24 hours) and short term adverse events(within 2 weeks) was entered into the protocol sheet.
In case of recurrence(stage 2-3 (as defined by ICROP) any zone), laser treatment was given to the avascular retina using the Nd Yag laser indirect ophthalmoscope. Repeat injections were not given in the study.
Inclusion criteria
All babies with type 1 ROP-Zone 1stage 2 or stage 3 with plus or zone 2 stage 3 with plus disease.
Exclusion criteria
Babies who had stage 3 ROP with plus in Zone 2 anterior retina (close to zone 3)
Babies who were not given systemic fitness for procedure
Statistical methods- Data was entered into an excel sheet and Statistical analysis were done using SPSS Statistics 20. All continuous parameters were represented as mean +/- SD. All categorized parameters were represented either in frequency or in percentage. Pearson correlation coefficient were used for finding the correlation between two continuous parameters. The non-parametric Mann Whitney U test were used for comparing the average parameters between two groups if p<0.05 were considered as statistically significant. Pearson chi square used for comparing two categorized variables.
Results
62 eyes of 31 babies were included in the study. There were 19 females(61.3%) and 12 males(38.7%). 10 babies were singletons(32.3%) and 21(67.7%) were part of multiple pregnancy.
Figure 1 shows the distribution of the infants according to the gestational age at birth. The maximum number of babies were in the <30 weeks(21) with 10 <27 weeks of gestation .The mean gestational age at birth was 28.26(+- 2.24) weeks. Minimum age of those in the study was 24 weeks and maximum 33 weeks.
Figure 1
Figure 2 shows the distribution of babies according to birthweight.
The maximum number of babies were in the <1kg group(17) and the mean birthweight was 1.01(+/- 0.25) kg.
Acc to mode of delivery-23 babies(74.2%) were delivered by LSCS and 8 babies (24.8 %) by normal delivery.
Most of the babies had (56 eyes) (90.3%)had zone2 posterior disease and only 6 eyes(9.7%) had zone 1 disease(APROP). All zone 1 disease was APROP and all (100% )babies had plus disease.
Table 1
| AGE AT TIME OF INJECTION (weeks) | |||||
| Age of the baby | Frequency | Percent | |||
| 0-4 | 6 | 19.4 | |||
| 5-8 | 13 | 41.9 | |||
| 9-12 | 12 | 38.7 | |||
| Total | 31 | 100.0 | |||
Table 1 shows the age distribution of the babies at the time of intravitreal injection. The mean age at time of injection was 7.39 weeks(+/- 2.552) with a minimum age of 3 weeks and maximum 12 weeks.
Table 2
| Post conceptual age | Frequency | Percent | |
| 32-34 | 14 | 45.2 | |
| 35-36 | 9 | 29.0 | |
| 37-38 | 5 | 16.1 | |
| 39-40 | 3 | 9.7 | |
| Total | 31 | 100.0 | |
45.2 % of the babies underwent injection at a PCA of 32-34 weeks with a mean age of 35.35(+/- 2.02) weeks at the time of injection.
Of the 62 eyes, 6 eyes underwent injection Ranibizumab and 56 eyes underwent Bevacizumab injection.
None of the babies had any immediate or short term adverse effects attributable to the injection in the follow up period.
100 % of eyes had regression of plus disease and complete regression of stage 3 ROP at first week follow up.
4 eyes(6.5 %) required laser treatment for recurrence of the disease while 93.5% vascularised to periphery without recurrence. All the four eyes had zone 2 stage 3 with plus.There was no recurrence in the zone 1 disease.
Ranibizumab had a higher rate of recurrence of ROP(33.3 %) requiring laser treatment compared to bevacizumab (3.5%) and this difference was statistically significant(p=0.005) Figure 3 shows the comparison
Fig 3
The mean time taken for full vascularisation was 16.035 (+/- 4.476) weeks and the babies had a mean post conceptual age of 51.46 (+/- 3.986) weeks at full vascularisation as shown in table3. This value was calculated after excluding the babies who underwent laser(n=29).
Table 3
| Laser | N | Mean | Std. Deviation | Std. Error Mean | |
| TIME TAKEN FOR VASCULARISATION | |||||
| 29 | 16.0357 | 4.47613 | .84591 | ||
| AGE AT FULL VASCULARISATION (weeks) | |||||
| 29 | 51.46 | 3.986 | .753 | ||
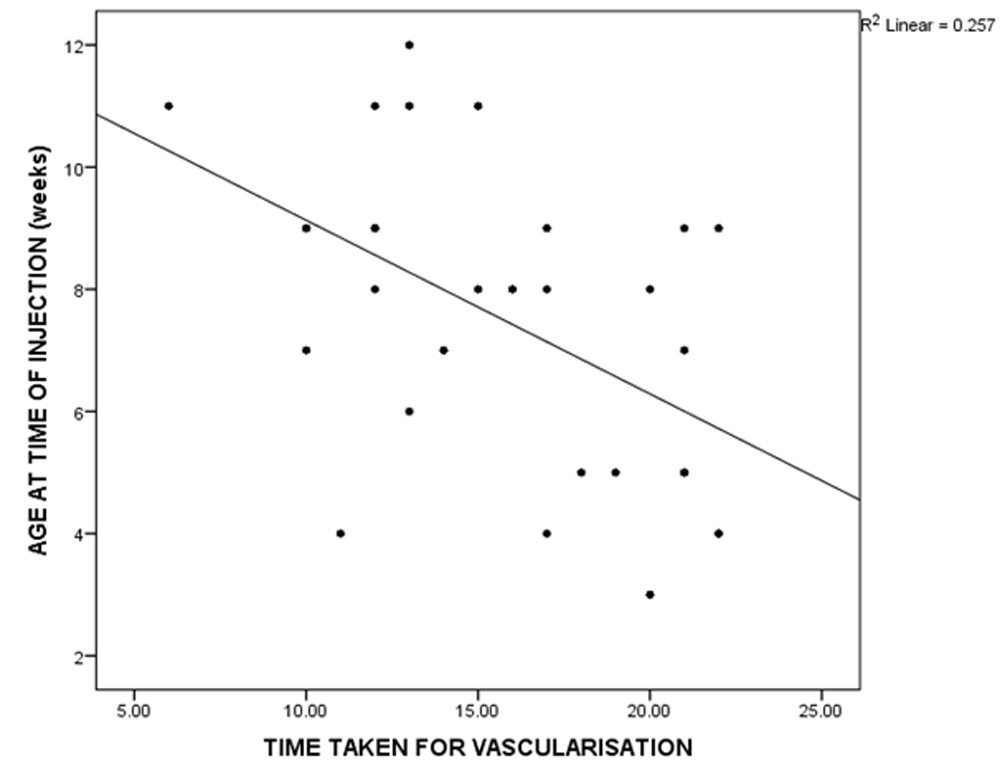
The time taken for vascularisation and age at full vascularisation was correlated with gestational age at birth,age at time of injection, birth weight and zone of the ROP. There was a statistically significant negative correlation between time taken for vascularisation with age of the at time of injection . (r= -0.384, p=0.033) Others were not found to be significant. That is to say, the older the baby at the time of injection, the less time it took to full vascularisation.(Figure 4 )
Figure 4
Discussion
62 eyes of 31 babies were included in the study. 56 eyes had zone 2 and 6 eyes had zone 1 disease and all eyes had stage 3 with plus disease. Our study showed that intravitreal antivegf injection is an effective treatment for zone 1 and zone 2 ROP stage 3 with plus.
The rate of recurrence for zone 1 and 2 combined was 6.5% which is comparable with the results of the BEAT ROP study(6% in zone 1 and 2 combined)6 while our rate of recurrence for zone 1 disease was 0 which is a better result compared to BEAT ROPs rate of 6% for zone 1 disease also6. The BEATROP however came under widespread criticism because of the higher recurrence rates for laser treatment in their trial compared to other studies and personal experiences.7,8,9
The BEAT ROP also gave a mean recurrence time of 16 weeks +- 4.6 weeks and our mean time for full vascularisation was 16.035+-4.4 weeks which retiterates that these babies need to be followed up for a much a longer period that usual. The BEAT ROP followed up the babies till 54 weeks and our mean age at full vascularisation was 51.46 +/- 3.9.6.This clearly shows that these babies who are treated by anti VEGF injections need to be followed up to atleast 52 weeks PCA or full vascularisation whichever is earlier.
Looking at other studies, In a case series by Wu et al, they included 49 eyes of 27 patients and they had a recurrence of rate of 10% and a mean injection time of 36.8 weeks compared to our 6.5% and 35.5 weeks5 while a small series of 12 eyes by Dorta et al showed no recurrence at all.3We also found a statistically significant negative correlation with age at time of injection which should be taken into account while following up these babies-those who had injection done earlier in the period after birth required followed up for a longer period and took more time to vascularise fully.
Comparing the recurrence rate of ranibizumab and bevacizumab we found a much higher rate for the former. We had in our study a 33.3 % recurrence rate in the ranibizumab treated eyes compared to 3.5% in the bevacizumab group. Although the numbers are small, this difference was found to be statistically significant. This compares well with other studies by Wong et al(5 out of 6 eyes)10 and also by Erol Mk et al 11(6 out of 15 eyes).A 50 % recurrence rate in ranibizumab treated rop eyes have been reported in the study by Gunay et al 12.This evidence suggests that although bevacizumab use is off label it maybe a better choice for treatment of ROP than ranibizumab. This gives the added advantage of being cost effective and can bring down the treatment costs significantly compared to conventional laser treatment also.
Our sample size was too small to assess for adverse events but no infant developed any ocular or systemic adverse event that was attributable to the injection or the drug used which means that anti VEGf injections are relatively safe in these infants.
Table 4 shows the comparison of our study with various other international studies.
References
- 1. Early Treatment For Retinopathy Of Prematurity Cooperative Group. Revised indications for the treatment of retinopathy of
prematurity: results of the early treatment for retinopathy of prematurity randomized trial. Arch. Ophthalmol. (Chicago, Ill. 1960)
121, 1684–94 (2003)
- Repka MX, Tung B, Good WV, et al. Outcome of eyes developing retinal detachment during the Early Treatment for Retinopathy of Prematurity Study (ETROP). Arch Ophthalmol. 2006; 124:24–30. [PubMed: 16401781]
- Dorta P, Kychenthal A. Treatment of type 1 retinopathy of prematurity with intravitrealbevacizumab (Avastin). Retina. 2010; 30(Suppl):S24–S31. [PubMed: 20224475]
- Ahmed AE, Channa R, Durrani J, Ali A, Ahmad K. Early experience with intravitrealbevacizumab combined with laser treatment for retinopathy of prematurity. Middle East Afr JOphthalmol. 2010; 17:264–7. [PubMed: 20844684]
- Wu W-C, Yeh P-T, Chen S-N, Yang C-M, Lai C-C, Kuo H-K. Effects and complications of bevacizumab use in patients with retinopathy of prematurity: a multicenter study in Taiwan.Ophthalmology. 2011; 118:176–83. [PubMed: 20673589]
- Efficacy of Intravitreal Bevacizumab for Stage 3+ Retinopathy of Prematurity Helen A. Mintz-Hittner, M.D., Kathleen A. Kennedy, M.D., M.P.H., and Alice Z. Chuang, Ph.D.N Engl J Med. 2011 February 17; 364(7): 603–615. doi:10.1056/NEJMoa1007374
- Raizada S,Al Kandari J,Al Sabti K.Will the BEAT-ROP study results really beat ROP? Invest Ophthalmol Vis Sci.2011;52:9288-9289
- Moshfeghi DM, Berrocal AM. Retinopathy of prematurity in the time of bevacizumab:incorporating the BEAT-ROP results into clinical practice.Ophthalmology.2011;118:1227-1228
- Azad R. use of intravitreal anti-VEGF:Retinopathy of prematurity surgeons’ in Hamlet’s dilemma? Indian J Ophthalmol.2011;59;421-422.
10..RWong, R. K., Hubschman, S. & Tsui, I. Reactivation of retinopathy of prematurity after ranibizumab treatment. Retina 35, 675–80(2015)
11.Erol, M. K. et al. Comparison of intravitreal ranibizumab and bevacizumab treatment for retinopathy of prematurity. Arq. Bras. Oftalmol. 78, 340–3 (2015).
- Gunay M1, Sukgen EA2, Celik G1, Kocluk Y2 Comparison of Bevacizumab, Ranibizumab, and Laser Photocoagulation in the Treatment of Retinopathy of Prematurity in Turkey. Current eye research ,2017;issue 42
13Castellanos, M. A. M., Schwartz, S., García-Aguirre, G. & Quiroz-Mercado, H. Short-term outcome after intravitreal ranibizumab injections for the treatment of retinopathy of prematurity. Br. J. Ophthalmol. 97, 816–9 (2013)
- Chen, S.-N. et al. Intravitreal anti-vascular endothelial growth factor treatment for retinopathy of prematurity: comparison between Ranibizumab and Bevacizumab. Retina 35, 667–74 (2015).
- Lin, C.-J., Chen, S.-N. & Hwang, J.-F. Intravitreal ranibizumab as salvage therapy in an extremely low-birth-weight infant with rush type retinopathy of prematurity. Oman J. Ophthalmol. 5, 184–6 (2012).
- Jang, S. Y., Choi, K. S. & Lee, S. J. Delayed-onset retinal detachment after an intravitreal injection of ranibizumab for zone 1 plus retinopathy of prematurity. J. AAPOS 14, 457–9 (2010).
- Chan, J. J. T. et al. Risk of recurrence of retinopathy of prematurity after initial
intravitreal ranibizumab therapy. Sci. Rep. 6, 27082; doi: 10.1038/srep27082 (2016).
Leave a Comment