
Dr. Rajiv Kumar Gupta, G10160, Dr. M. Shiraz Ali
INTRODUCTION:
Diabetic retinopathy (DR) is rated as the most important cause of irreversible blindness, posing a serious public health problem worldwide. It is more relevant in India, as it is increasing at such an alarming rate that from 17th place 20 years ago, it has now occupied 6th place in the causation of ocular morbidity and blindness1. WHO has included DR as one of the priority target in India in Its VISION 2020 program2.
India is going to be the diabetic capital of the world very soon. According to WHO survey, about 32 million people were affected by DM in the year 2000, which is reported to rise to about 80 million by 20301. It is estimated that 15-25% of diabetic population will develop DR3. Thus, every case of DM should be regarded as a potential candidate for occurrence of DR. This ocular complication of diabetes mellitus is not only dependent on carbohydrate metabolism, use of little or no Insulin or severity of disease but also depends much more on the duration of the disease. The modern anti-diabetic treatment has greatly enhanced the life expectancy of patients; and the occurrence of diabetes at younger age leads to increased incidence of DR. Further associated diseases like hypertension and renal disease or pregnancy greatly enhances the incidence of retinopathy.
As DR in early stage is a symptomless condition, so regular examination of the eye is necessary to detect it. Visual impairment or loss of vision can be prevented or delayed by timely management of DR, especially by laser photocoagulation. However, due to lack of proper screening and treatment facilities, mainly at the primary level, many of the undiagnosed and uncontrolled patients become blind. It has also been found in majority of DR patients screened at primary level, when referred to secondary or tertiary healthcare centre for treatment, did not reach there4-6. Thus early detection and timely treatment of the patient poses a serious challenge to health care delivery system in our country.
AIM:
To assess the supportive role of Ophthalmic Assistant in management of DR in tribal population of Jharkhand
MATERIAL AND METHODS
Four ophthalmic assistants posted in Ramgarh district of Jharkhand state were given 2 months training for screening and management of DR at Rajendra Institute of Medical Sciences (RIMS), Ranchi, Jharkhand, a tertiary care centre. The training schedule included imparting knowledge and providing literature about diabetes and its complications, especially DR. They were initially taught to do the comprehensive eye examination. They were then trained in direct ophthalmoscopy in dilated pupils and in interpretation of fundus photos. They were trained todifferentiate between normal fundus and DR fundus, so that they could promptly refer the DR cases to RIMS, Ranchi.
After completion of one year of training each OA were sent to one CHC of Ramgarh district respectively to screen the diabetic patients for retinopathy. A total no. of 3642 diabetic patients were screened for DR in different CHCs from June 2015 to September 2016. The screening module encompassed:
I.Clinical history :
Regarding age, sex of the patient, age of onset and duration of diabetes, family history, type of DM, controlled status of DM, associated history of hypertension and renal disease, any visual disturbance like diminution of vision, blurred vision, floaters, double vision etc.
II.Clinical ocular examination
Visual acuity – Distance and near vision tested by Snellen’s chart/Jaeger’s chart
Measurement of intraocular pressure by Schiotz tonometer
Examination of anterior segment by slit lamp
Examination of posterior segment by direct ophthalmoscope
III.General examination including measurement of blood pressure
IV.Investigations
Examination of urine for sugar, albumin etc
Blood sugar estimation – Fasting/Post Prandial/random
Blood urea, serum Creatinine examination
V.Screening for diabetic population for retinopathy
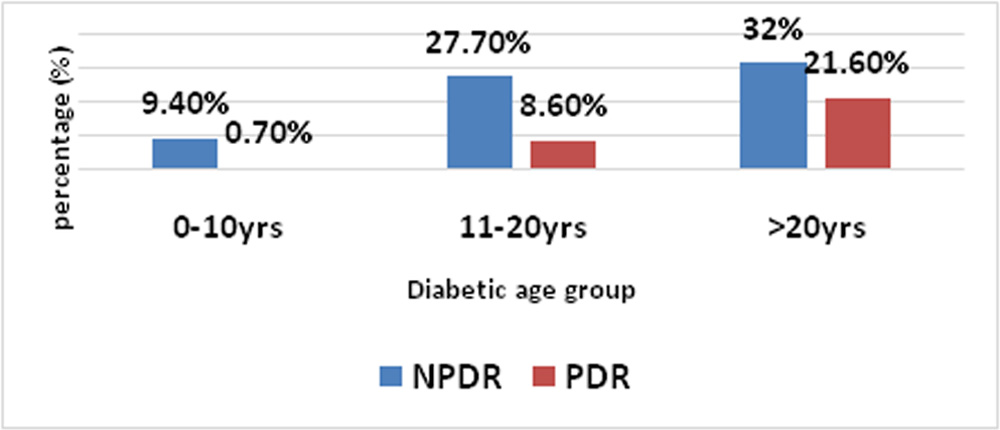
In this study for screening purposes, DR was divided into following groups:
Non – proliferative diabetic Retinopathy (NPDR) : Capillary macroaneurysm, hard exudates, soft exudates, venous changes like dilatation and tortuosity
Proliferative diabetic Retinopathy (PDR) : Neovascularisation, vitreous haemorrhage, and retinal detachment
Associated maculopathy : In the form of macular oedema, either focal or diffuse or ischemic and can occur in any of the above stage
OA were entrusted for the regular check – up, treatment, follow up and counseling of the screened DR patients.
Results:
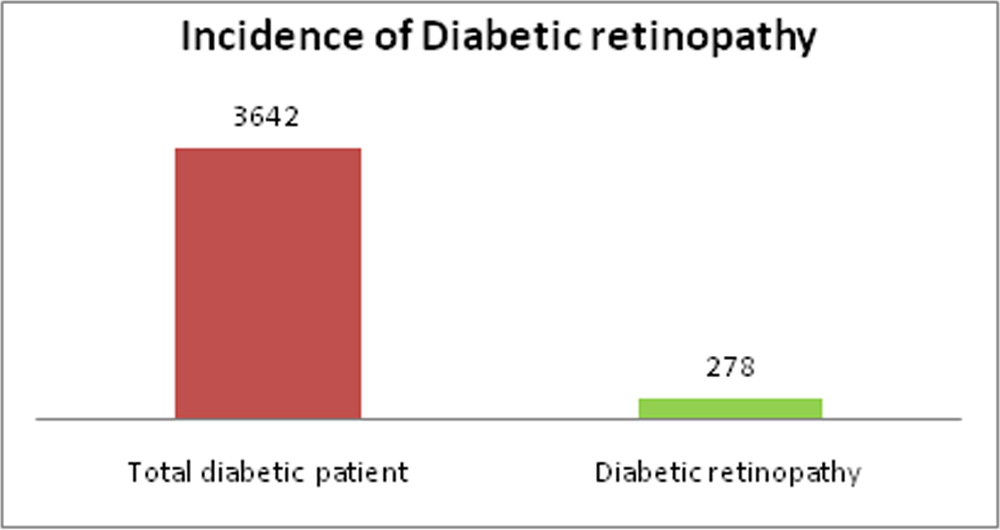
- Incidence of diabetic retinopathy:
Out of 3642 diabetic patients, 278 (7.6%) had retinopathy.
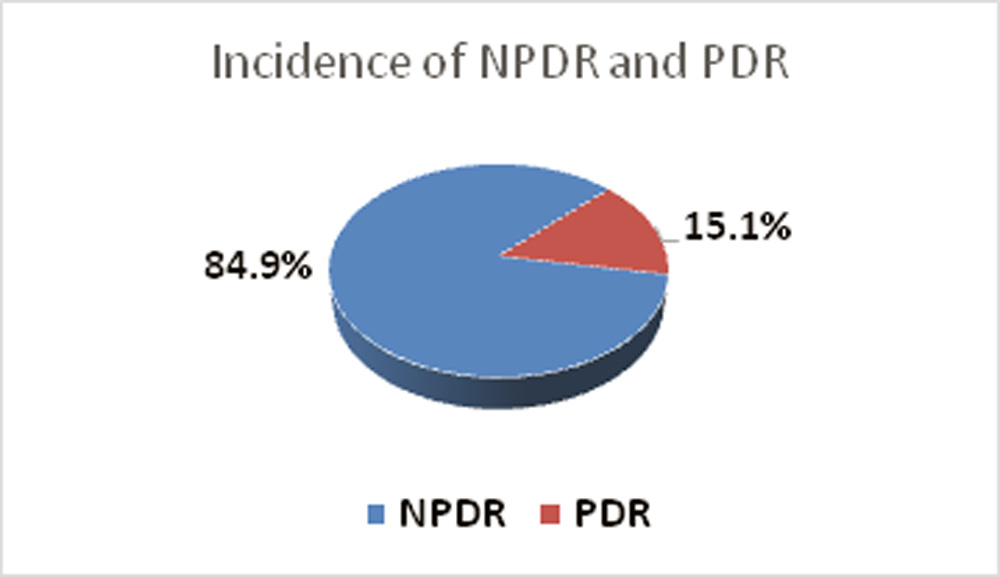
- Incidence of NPDR and PDR:
Out of 278 DR patients, 236 (84.9%) had NPDR and 42 (15.1%) had PDR.
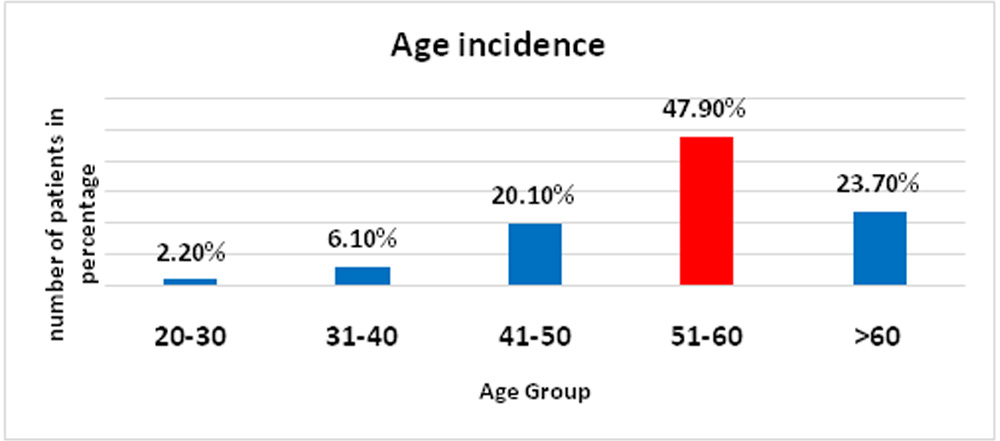
- Age incidence:
Majority of DR patients 133 (47.9 %) were in the age group of 51-60yrs
- Sex incidence:
Males 169 (60.8%) predominated females 109 (39.2%).
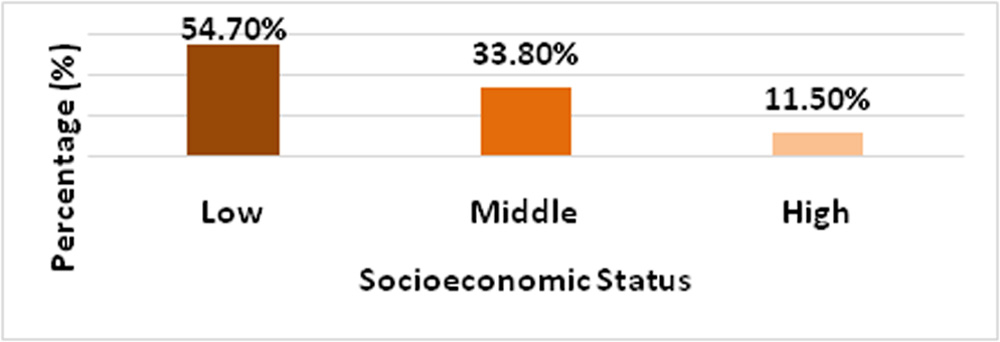
- Socioeconomic status:
Majority(54.70 %) of the patients belonged to low socioeconomic group.
- Presenting symptoms:
Majority of the patients came with gross diminution of vision, while few complaint of total loss of vision.
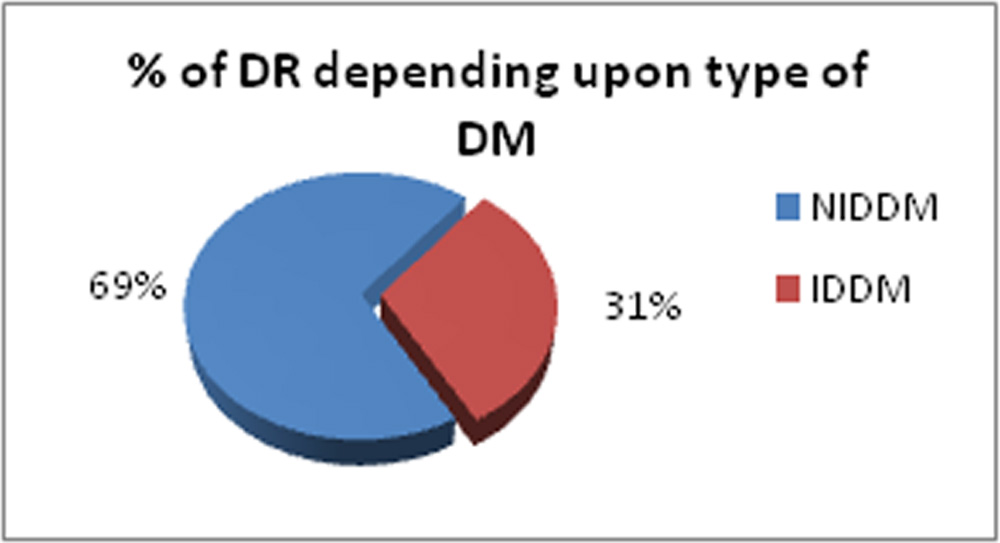
- Number of DR patients depending upon the type of DM :
Majority (69 %) of patients belonged to NIDM group.
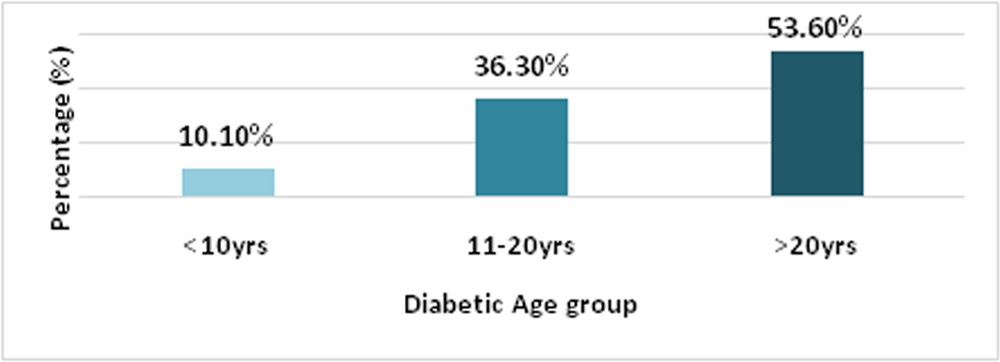
- Incidence of Diabetic retinopathy depending upon diabetic age :
Majority of patients who had DR were suffering from DM for more than 20 years.
The incidence of DR in less than 10years of diabetic age was 10.1%, which increased to 53.6% in above 20years. Between 11-20 years, the incidence was 36.3%.
Compliance of DR patients, supervised by O.A. :
As far as regular check up, treatment and follow – up was concerned, the compliance was 79.5%.
- Reasons for better compliance :
- Regular comprehensive eye examination and screening of diabetic patients for retinopathy at primary level
- Providing assistance in getting treatment at district and tertiary eye care centres
- Regular follow up
- Repeated counseling and persuasion of the patients
- Better interaction as they always remain in touch with patients
DISCUSSION
DR is going to be a major cause of blindness in India, as in the near future it will have highest number of diabetic population in the world. Early detection and timely management of DR is necessary to safeguard the vision. But detection and treatment of DR at primary level in rural or semi urban area is a major public health problem, due to poor infrastructure, paucity of trained personnel and expensive treatment. So, timely referral and management of DR patients at secondary or tertiary eye care centres is of utmost importance.
This study was undertaken in the Adivasi dominated region of Jharkhand, most of whomlives below poverty line. Ophthalmic assistants trained for screening, regular check up, treatment and follow – up of diabetic persons for retinopathy were involved at primary level.
Out of 3642 diabetic patients screened by OA, at different CHCs, 278 (7.6%), had retinopathy. The DR patients were explained about progression of disease and warned about losing vision if not properly treated and when not under regular follow – up. It was found that compliance rate as far as regular check up, getting treatment and follow up of DR patients were concerned, it was 79.5%. It was very encouraging as the author in his previous study, had found compliance rate at of only 46.1%, when not supervised by OA. The reason for better compliance may be attributed to screening of DR by OAs. Furthermore, OAs were involved at every step, starting from diagnosis, treatment and follow up. The patients were counseled well by repeated persuasion and providing literature about DR.
CONCLUSION
OAs after a brief training became good resource persons in screening and management of DR, as in the present study compliance rate was 79.5%. This can be adopted as role model for different states.
TAKE HOME MESSAGE
OA may become a key player in war against DR.
Abbreviations:
OA: Ophthalmic Assistant
DR: Diabetic Retinopathy
DM: Diabetes Mellitus
NPDR: Non proliferative Diabetes Mellitus
PDR: Non proliferative Diabetes Mellitus
REFERENCES
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27:1047-53.
- Ackland P. The accomplishments of the global initiative VISION 2020: The Right to Sight and the focus for the next 8 years of the campaign. Indian Journal of Ophthalmology. 2012;60(5):380-386.
- Gadkari SS, Maskati QB, Nayak BK. Prevalence of diabetic retinopathy in India: The All India Ophthalmological Society Diabetic Retinopathy Eye Screening Study 2014. Indian J Ophthalmol 2016;64:38-44
- Misra V, Vashist P, Malhotra S, Gupta SK. Models for Primary Eye Care Services in India. Indian J Community Med 2015;40:79-84
- Khan MA, Soni M, Khan MD. Development of primary eye care as an integrated part of comprehensive health care. Community Eye Health 1998;11:24-6
- Gilbert CE, Babu RG, Gudlavalleti AS, Anchala R, Shukla R, Ballabh PH, et al. Eye care infrastructure and human resources for managing diabetic retinopathy in India: The India 11-city 9-state study. Indian J EndocrMetab 2016;20:3-10.
Leave a Comment