
Dr. Chidanand Kulkarni, K12528
ABSTRACT
In this institute, ethical committee approved prospective observational study; nuclei obtained from immature senile cataract cases undergoing manual small incision cataract surgery (MSICS) were measured using a smartphone based micrometer scale of 100 microns accuracy. Preoperative LOCS III grading was recorded. An analysis of thickness and diameter of the nucleus, its relation to LOCS III, lens thickness, ACD and age was carried out. The nuclear thickness increased significantly with higher grades of LOCS III. There was significant relation between nuclear diameter and LOCS III nuclear grading. This study establishes a direct correlation between nuclear thickness and LOCS III classification. Estimating nuclear thickness becomes more important in case of phacoemulsification using ultrasound and more so with laser. Estimation of nuclear diameter helps in deciding the length of MICS tunnel. Thus LOCS III nuclear grading would help in adjusting machine settings during various steps of nuclear removal as it is directly correlated with nuclear size and density.
Introduction:
Nuclear cataract is the most common form of age related cataract in India and worldwide.1,2 It is also the most important category among the morphological types of senile cataract. Present day techniques of extra-capsular cataract extraction mainly aim at removing the nucleus with as small an incision size as possible. Manual small incision cataract surgery (MSICS) takes the approach of creating a sclero-corneal tunnel to reduce incision size. Conventional phacoemulsification technique attempts to remove nucleus by using ultrasound energy while Femto Laser assisted cataract surgery (FLACS) does this by using laser energy. Thus assessing the nuclear characters like density and size preoperatively is imperative for any of these surgical techniques.
The lens opacity classification system III (LOCS III) was introduced in 1993 as a subjective grading system for cataract using slit lamp, with accuracy comparable to objective methods.3 It established a better grading system for age related cataract as compared to LOCS II. It was validated to be highly consistent between users and during follow up comparison. Though the grading of nuclear cataract in this method can be done either using its opacity or its color, both are equally effective. It is common to use nuclear opacity (NO) for grading nuclear cataract in routine clinical practice. The NO is graded from 0.1 to 6.9 from clear lens to very opaque or brunescent nuclear cataract.3
In a study by Gullapalli et al the color of nucleus was compared with hardness and nuclear size. They demonstrated that as the nuclear color increases, its hardness, diameter and central thickness increases.4
Ayaki et al studied the thickness and diameter of nucleus extracted by conventional ECCE. They found the mean nuclear diameter was 6.51 + 0.75 mm and the mean thickness, 2.96 + 0.33 mm.
In another study Smith et al studied a small set of patients (N=16) and observed that there was a significant inverse correlation between NO and antero-posterior linear compressibility of the nucleus. They concluded that the LOCS III grade correlates well with hardness of the nucleus.5 This confirms similar observations by various studies conducted previously.6-10
In conventional phacoemulsification, almost all the energy delivered during the procedure is spent on emulsification of nucleus. Increase in severity of nuclear cataract is associated with excessive use of energy for emulsification of the nucleus. Excessive use of energy is associated with various intraocular complications like endothelial cell loss, increased postoperative uveitis, cystoid macular edema etc.11,12 Though advanced technique like direct chop reduce need for energy as compared to divide and conquer, the energy utilization increases exponentially with increased LOCS III grade of nucleus.
FLACS introduced less than a decade back has increased the accuracy of various steps of cataract surgery by another notch. It allows for precision in size and shape in steps like corneal incision, capsulorhexis and side port. Since its conception this technique is evolving rapidly. Present day machines can be used in the same room and even on same table sequentially to complete all steps of the surgery in same sitting. This system tackles nuclear cataract by creating a grid pattern of laser spots applied from posterior to anterior part of the nucleus to separate the lenticular fibers and facilitate emulsification by ultrasound. This technique can be used for nucleus from grade I to grade V of LOCS III classification. Again, similar to conventional phacoemulsification, the overall energy used increases with increasing LOCS III grade of nucleus.12,13
Our study was planned to answer the question whether nuclear thickness and diameter increases significantly with LOCS III grades of nuclear opacity. In present study, the measurement technique for nuclear size was same for both thickness and diameter. In addition, the number of cases studied was kept sufficiently high to increase the cases in each grade of LOCS III.
A smart phone (Micromax Canvas A120) was used at various steps in this study.A Use of smartphone makes various clinical steps easy and accurate. This smartphone had touch screen, display size of 5 inches and pixel density of 294 pixels/inch which works out to 86 microns per pixel. Thus, less than 100 microns accuracy of measurement was possible.
With widespread availability of smartphones having high-density display, the pixel size has become smaller. The physical size of a display and pixel density can be used to calculate distance between two pixels on the display to micrometer accuracy. Many applications (apps) are available on google play website for this purpose. In this study, we used an app named “ON rule” version 2.0. This is a free app, and provides two pairs of lines to assess size of physical objects in both dimensions simultaneously (length and breadth).B In addition it provides measurement values up to 3 decimal points taking accuracy to micrometer level.
Materials and methods:
Ethics approval for this research was obtained from the Institutional ethics committee. This research adhered to the tenets of the Declaration of Helsinki. Successive cases of immature senile cataract undergoing manual cataract extraction were selected for the study. All data remained confidential.
The inclusion criteria were senile cataract undergoing MSICS or extra-large temporal tunnel cataract extraction (ETCE) technique, and uneventful surgery.14 Only cases with intact nuclei after removal, were taken up for further evaluation.
Exclusion criteria were set as incomplete preoperative workup, mainly non-availability of LOCS III grading, poor mydriaisis, complicated cataract, chipped or broken nucleus, previous intraocular surgeries, incomplete hydro delineation, if measurement of nuclear size was not carried out within two hours of removal of nucleus.
The nuclear opacity in immature cataracts was assessed as described in the original article by comparing slit lamp finding to the standard image on mobile screen with 100% brightness.3 The standard image for LOCS III grading was used on full screen mode of the smartphone to assess the NO of the cataract. For the analysis, the grading was rounded off to nearest round number. For example if NO was found to be 2.2 it was graded as NO2 while if it was 2.5 it was graded NO3 and so on. Grades from 6.5 to 6.9 were kept as a separate category of 6.9. Thus, from grade one to grade 6.9 we had seven groups of nuclear densities.
The ocular dimensions were measured using immersion biometry during preoperative intraocular lens calculation. Alcon Ocuscan RxP immersion A-scan machine was used for this purpose. Mean of ten readings was taken and the standard deviation was kept less than 0.05 for accepting the readings. Axial length (AL), anterior chamber depth (ACD) and lens thickness (LT) were thus obtained. The central corneal thickness (CCT) was recorded using same machine by pachymetry.
In this study we used an app named “ON ruler” version 2.0 to measure the nuclear dimensions. This is a free app, and provides two pairs of lines to assess length and breadth of physical objects simultaneously in millimeters.B Also it provides measurement values up to 3 decimal points taking accuracy to micrometer level. The app has to be calibrated once by comparing against a known length. A 2.2 mm keratome (Alcon labs) was used for this purpose and measurement unit of one millimeter was calibrated. This setting was used throughout the experiment. The same procedure was carried out before every measurement.
A simple method was developed to measure the dimensions of the nucleus. After wiping loose lens fibers from surface of the nucleus with gauze piece, the nucleus was rinsed and wiped once more. The relatively dry nucleus was used for measuring diameter and thickness.
Measurement of diameter: The microscope was set at 0.6x magnification with 10x ocular without switching on light. The background illumination of smartphone was set to maximum. The App was launched and four crosshair option was selected. The nucleus was placed in the center of the screen with anterior surface (flatter surface) in contact with the screen. The vertical (Y axis) and horizontal (X axis) pairs of lines were adjusted while observing under microscope with mono-ocular view. Right ocular was used throughout the study to maintain uniformity and to avoid parallax error. Values along x and y axes were recorded up to 3 decimal points. The procedure was repeated 3 times and average was taken as final value. The nucleus was skewered adjacent to its center using a 26G needle on 10cc syringe holding the syringe vertically. This nucleus mounted on 26G needle was placed with its equatorial edge touching the screen so that its thickness could be measured. The measurement was taken similar to measuring diameter but only in one axis. The syringe was rotated 900 on its axis and thickness of nucleus was measured again. Average of these two measurements was taken as thickness of the nucleus.
Statistical analysis:
Statistical analysis was performed using SPSS software (version 21.0, IBM Inc. Chicago, Illinois). The normality of data was tested using histogram method and Kolmogorov-Smirnov Test. Descriptive statistics was presented as mean and standard deviations. For comparison of between group variations, one way ANOVA was used. The level of significance was set at P<0.05 across all parameters.
Results:
The study enrolled 100 eyes from 100 consecutive patients undergoing MSICS or ETCE over a nine months period in a medical college hospital.
Table 1 summarizes the study population characteristics. Mean age of the patients was 65.5+ 10.3 years. Thus, the age of the study group was fairly advanced. This would indicate presence of a denser nucleus. The mean LOCS III grade of the groups was 4.4+1.4 confirming that most of the patients had denser nuclear cataract.
There were slightly more female patients than males in this study (F:M=54:46).
The average nuclear thickness in this study group was 3.31 mm (range 2.57-4.20). The average nuclear diameter in this study group was 7.29 mm (range 5.15-9.48).
The one way ANOVA test for nuclear thickness at various grades of LOCS III yielded highly significant (p<0.001) difference in nuclear thickness between the LOCS III grades from grade 1 to grade 6.9 (Figure 1). Similarly, there was highly significant (p<0.001) difference in nuclear diameter between the LOCS III grades from grade 1 to grade 6.9(Figure 1). Similar test for age in different grades of LOCS III indicated there were significantly older patients as the nuclear grade increased. These findings reaffirm the fact that with advancing age, the nuclear cataract becomes more severe. There was no significant difference between the groups with respect to ACD, LT and AL.
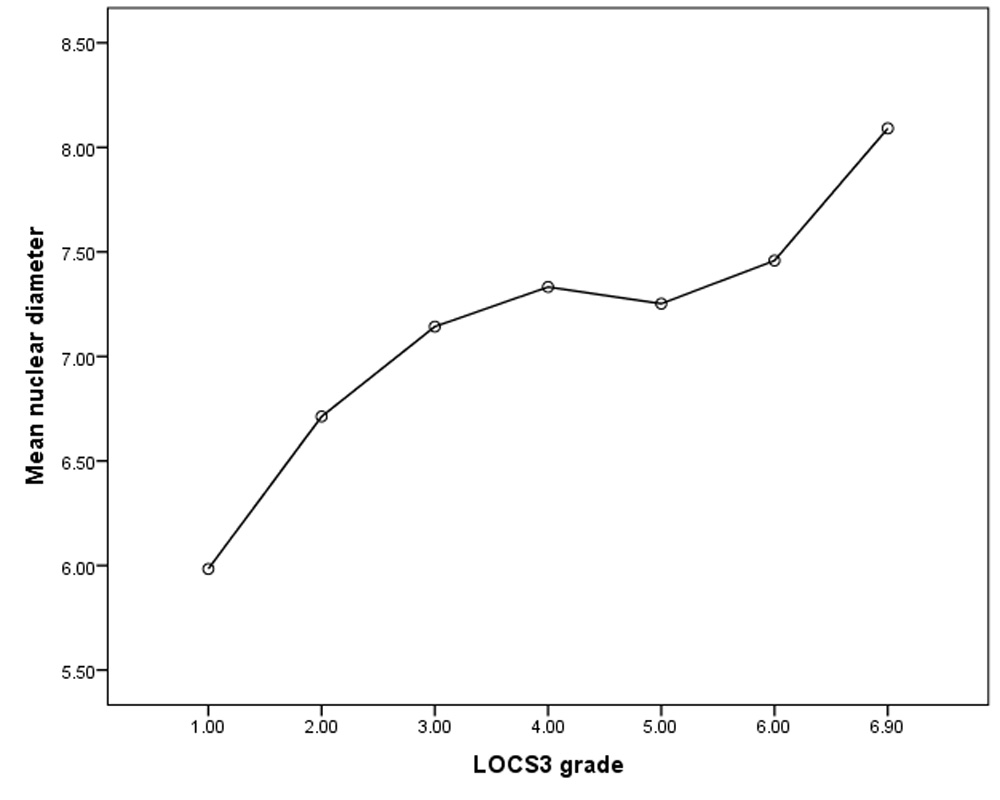
When the mean nuclear thickness was compared between groups, there was progressive increase in thickness from grade 1 to grade 4. The thickness reduced between grade 4 and 5, while it increased steeply from grade 5 to 6.9(Figure 3). The mean nuclear diameter likewise reduced between groups 4 and 5(Figure 4). This indicates there is a period during growth of nuclear cataract during which its density increases without an appreciable increase in its size.
Discussion:
LOCS III grading clearly establishes that the color or opacity of nucleus can predict density and hardness of the nucleus. But the size of nucleus is also a determinant factor for deciding type of surgical method, incision size, the amount of energy used and even the complication rates.
It has been common experience to find nuclear size increasing with nuclear density. But in some cases of nuclear cataract the nucleus can be large without being dense on one hand while a sclerosed nucleus can be very dense but small in size. Establishing a relation between LOCS III and nuclear size by direct measurement makes it possible to consistently predict the nuclear size preoperatively. This would help the cataract surgeon take better decisions pre- and peroperatively.
We used a simple method of smartphone screen under operating microscope to record micrometer measurements. Use of a mobile phone and app for measuring the nuclear size made it highly accurate, easily repeatable and possible for the technician to assess nuclear size rapidly and accurately under microscope. This is the first instance where a smart phone is used to measure nuclear size to micrometer level of accuracy.
The range of thickness between different NO grades in this study varies from 2.75 mm to 4.20 mm. The safe zone of nuclear emulsification can be decided depending on this information and LOCS III grade. In nucleus removal by various trenching techniques the estimation of NO should give direct evidence about thickness of nucleus preoperatively. Thus, the trench depth can be decided by knowing LOCS III grading for the case.
During phacochop technique of nuclear removal a chopper with sharp edge is used for chopping. Due to concerns of chopper damaging posterior capsule the usual length of sharp chopper is kept 1-1.5 mm. But with additional safety of 1.5 mm in case of denser cataracts the chopper length need not be uniform for all grades of NO. While a grade 3 nucleus can be chopped by a short chopper, even 2.5 mm chopper may be safe in denser NO cases without compromising safety. Longer tip designs may be helpful in harder cataracts and may make the chopping more convenient.
In developing countries where bulk of the cataract load exists, MSICS has become quite popular.13 This surgery is fast, effective and safe. But for denser cataracts, the intraoperative complication rate increases while removing the nucleus.15 The major hurdle is removing the nucleus through a smaller tunnel and may cause many complications like endothelial cell damage, stretching of tunnel and bleeding from tunnel. Knowledge of nuclear diameter as indicated by LOCS III grading can guide the decision about the tunnel length and make the nuclear removal safer even in grade 6 to 6.9 nuclei.
In FLACS technique of cataract removal, femto second pulsed laser is applied in a grid of laser spots to create separation of nuclear fibres to facilitate later removal with or without emulsification. The grid pattern leaves a safe margin of 500 microns from anterior and posterior capsules of lens to prevent damage to the capsule (the Anterior/posterior capsule safety zone). As LOCS III grading is routinely done before surgery, this can guide the creation of grid by predicting the nuclear size in addition to intraoperative OCT. This safety zone is highest in case of lower nuclear grades and it reduces with progress in LOCS III grade as nuclear thickness increases. NO grade thus can be utilized for adjusting grid volume, making it more flexible so that both laser energy delivery and efficiency of the procedure can be adjusted for optimal performance. Further studies are necessary in this regard.
Finally, an unexpected outcome in this study was the relatively similar thickness and diameter of NO grades 4 and 5. Another study comparing lens thickness assessment using OCT and A-scan has reported a high degree of correlation between the two techniques in all LOCS III grades of nucleus except for grade 5.16 A possible explanation for this observation could be increase in density of the nucleus without change in nuclear thickness.
To summarize, this study provides a statistical support to what the experienced surgeon has realized over past two decades; that the nuclear thickness and diameter increase with increasing LOCS III grade of nuclear cataract. This knowledge can be utilized to improve and adjust the finer aspects of respective surgical techniques.
One important shortcoming of this study is that the surgeon was not blinded to LOCS III grading. This limitation was partly overcome by blinding the analysis of data.
Conclusions:
A simple method is described in this presentation for measuring nuclear thickness and diameter with minimal technical expertise. The analysis shows that LOCS III grading of nuclear opacity can predict nuclear thickness and diameter accurately. Between grades 4 and 5 the nuclear density increases out of proportion to its size. From grade 5 onwards the nuclear size increases sharply.
References:
- Barbara E.K, Klein R, Kristine E.Lee. Incidence of age-related cataract over a 10-year interval: the Beaver Dam Eye Study. Ophthalmology 2002; 109: 2052-2057.
- Vashist P, Talwar B, Gogoi M. Prevalence of Cataract in an Older Population in India: The India Study of Age-related Eye Disease.
- Chylack LT Jr, Wolfe JK, Singer DM, Leske MC,Bullimore MA, Bailey IL et al. The Lens Opacities Classification System III. Arch Ophthalmol 1993; 111: 831–836.
- Gullapalli VK, Murthy PR, Murthy KR. Colour of the nucleus as a marker of nuclear hardness, diameter and central thickness. Ind J Ophthalmol 1995; 43: 181–184.
- Ayaki M, Ohde H, Yokoyama N. Size of the lens nucleus separated by hydrodissection. Ophthalmic Surg Lasers 1993; 24: 492–493.
- The relationship between….
- Heyworth P, Thompson GM, Tabandeh H, McGuigan S.The relationship between clinical classification of cataract and lens hardness. Eye 1993; 7: 726–730.
- Tabandeh H, Thompson GM, Heyworth P. Lens hardness in mature cataracts. Eye 1994; 8: 453–455.
- Assia EI, Medan I, Rosner M. Correlation between clinical, physical and histopathological characteristics of the cataractous lens. Graefes Arch Clin Exp Ophthalmol 1997; 235: 745–748.
- Czygan G, Hartung C. On the correlation of mechanical and optical properties of cataractous eye lens nuclei.Biomed Tech 1997; 42: 2–6.
- Storr-Paulsen A, Norregaard JC, Ahmed S, Storr-Paulsen T, Pedersen TH. Endothelial cell damage after cataract surgery:divide-and-conquer versus phaco-chop technique. J Cataract Refract Surg 2008;34(6):996–1000.
- Abell RG, Kerr NM, Vote BJ. Toward zero effective phacoemulsification time using femtosecond laser pretreatment. Ophthalmology 2013;120(5):942–948.
- Khanna RC, Kaza S, Palamaner Subash Shantha G, et al . Comparative outcomes of manual small incision cataract surgery and phacoemulsification performed by ophthalmology trainees in a tertiary eye care hospital in India: a retrospective cohort design. BMJ Open 2012;2.
- Kulkarni C, Vivekananda U. Extra Large Temporal Tunnel Cataract Extraction [ETCE]. J Clin Diagn Res 2014;8(9):VC01-4.
- Mearza, A.A., Ramanathan, S., Bidgood, P., and Horgan, S. Visual outcome in cataract surgery complicated by vitreous loss in a district general hospital. Int Ophthalmol. 2009; 29: 157–160.
- Hamzeh N, Moghimi S, Latifi G, Mohammadi M, Khatibi N, Lin SC. Lens thickness assessment: anterior segment optical coherence tomography versus A-scan ultrasonography. Int J Ophthalmol. 2015; 8: 1151–1155.
Other referances:
- Micromax 2 colors smartphone features. https://www.gsmarena.com/micromax_a120_canvas_2_colors-6363.php accessed on 1/10/2017
- ON ruler, version 2.0 https://play.google.com/store/apps/details?id=com.potatotree.onruler last accessed on 7/6/2015
Tables and figures
Table 1. Baseline characters of the study group
| Parameter | Average | Minimum | Maximum |
| Age | 65.55 | 40 | 90 |
| Male:Female patients | 46:54 | ||
| Lens thickness (mm) | 4.25 | 3.18 | 5.58 |
| ACD (mm) | 3.33 | 2.34 | 4.02 |
| LOCS III grade | 4.41 | 1 | 6.9 |
| Nuclear thickness (mm) | 3.31 | 2.57 | 4.2 |
| Nuclear diameter (mm) | 7.14 | 3.39 | 9.48 |
Figure 1. One way ANOVA test among different LOCS III grades of nuclear opacity
| Parameter tested | F | Sig. |
| Nuclear thickness | 6.766 | .000 |
| Nuclear diameter | 6.875 | .000 |
Figure 2. Nuclear thickness and LOCS III grading
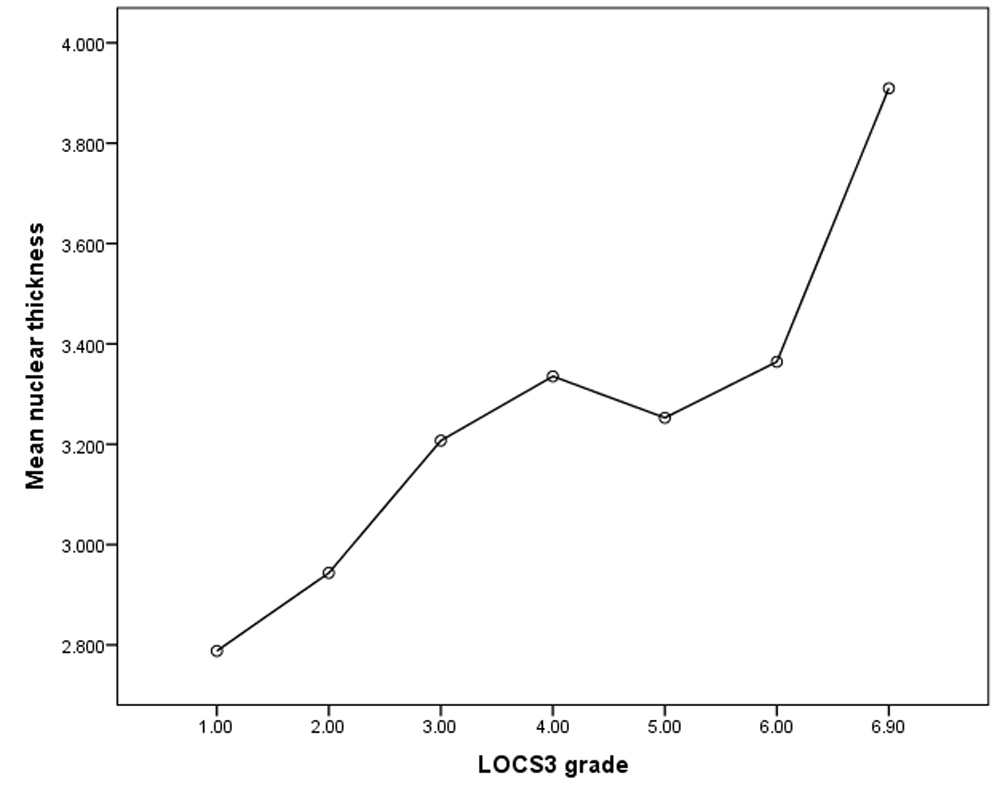
Figure 3. Nuclear diameter and LOCS III grading
Leave a Comment