
Dr. Deepak Bhojwani, B13467, Dr. Vasavada Abhaykumar Raghukant, Dr. Viraj Abhayakumar Vasavada, Dr. Shail
Abstract:
Aim: To report the short-term safety profile and clinical outcomes of scleral fixation of intraocular lenses (SFIOL) using Gore-Tex suture.
Methods:
Retrospective, interventional case series of 35 eyes(31patients)undergoing 4point scleral fixation technique using Gore-Tex suture. Primary outcome measures were occurrence of intraoperative and postoperative complications with minimum follow-up of 90 days.
Results: Posteriorly dislocated IOLs in vitreous was the commonest indication(18Eyes) followed by dislocated nucleus(6eyes). No major intraoperative complications were noted. SFIOL was decently centered in all cases. 7 patients had rise in IOP postoperatively managed with medical therapy, 2 of them underwent glaucoma surgery.Other postoperative complications noted were vitreous haemorrhage in 2 eyes, hyphema in 1 eye, cystoid macular oedema in 2eyes. All of them resolved with observation. 1 eye with pre-existing chronic macular hole developed retinal detachment requiring reintervention. Mean visual acuity improved from 1.52logmar preoperatively to 0.64; 0.44logmar postoperatively at 3 and 6 months(p<0.001). Mean follow-up was 12 months 17days(range 3months–3years). There were no cases of postoperative goretex suture related complications (erosion/ breakage/granuloma)in the entire follow-up period.
Conclusions : 4 point scleral fixation of IOLs with Gore-Tex suture was well tolerated in all cases. All eyes had well centered IOLs and no suture-related complications were encountered. This procedure led to improvement in visual acuity and was not associated with significant postoperative complications.
Introduction:
Surgical techniques for secondary IOL implantation have expanded over the past several years.1 Options for IOL placement include anterior chamber intraocular lenses (ACIOLs), iris-fixated posterior chamber intraocular lenses (PCIOLs) and scleral-fixated PCIOLs. The choice of surgical technique depends on many factors, including patient age, comorbid ocular conditions, anatomic considerations and surgeon preference.2 The scleral-fixated PCIOL technique may be preferred when a PCIOL is anatomically desired, such as in patients with corneal decompensation, or when iris anatomy is not amenable to iris fixation or an ACIOL.3 Scleral flaps and rotation of the suture knot have improved outcomes with the ab externo scleral sutured PCIOL surgical technique. However, suture erosion and breakage remain significant concerns. In one study, suture breakage was observed in 27.9% of cases at a mean of 6 years follow-up using 10-0 polypropylene suture.4
Gore-Tex (W.L. Gore & Associates, Elkton,Maryland, USA) suture is a non-absorbable, polytetrafluoroethylene monofilament suture with greater tensile strength than the more commonly used PROLENE (polypropylene; Ethicon,Somerville, New Jersey, USA) suture. Currently, Gore-Tex is commonly used for heart valve and vascular procedures underscoring the resiliency of the suture material.5 6 Ophthalmic surgeons are currently using Gore-Tex suture given a presumed decreased risk of suture breakage7 but clinical outcomes using this suture material in ophthalmic surgery have not been well described.
The purpose of this study is to review the clinical outcomes and safety profile of a trans-scleral sutured IOL technique using Gore-Tex suture.
Materials & methods:
Charts of all patients who underwent scleral fixation of a Aurolab PMMA scleral fixation IOL using CV-8 (USP 7-0) Gore-Tex suture (W.L. Gore & Associates) at Raghudeep Eye Hospital between October2014 till October 2016 were retrospectively reviewed.
Patient records were reviewed and the following data were collected: age, gender, preoperative and postoperative Snellen visual acuity (VA), preoperative and postoperative tonometry for intraocular pressure (IOP), surgical indications, keratometry values, and intraoperative and postoperative outcomes.
In each case, ab externo scleral fixation of an Aurolab SFIOL was performed using Gore-Tex CV-8 sutures. In every case anterior vitrectomy was performed before finishing the procedure.
Conventional biometry was used for IOL calculations. If trauma or other anatomic factors precluded this, biometry of the fellow eye was used for IOL power calculations. Ocular examination with Snellen VA, tonometry and slit-lamp biomicroscopy was performed on all patients at the 1 day, 1 week ,1 month, and all subsequent postoperative visits. Further follow-up was determined on a case-by-case basis. All postoperative complications were recorded.
Primary outcome measures were occurrence of intraoperative and postoperative complications with minimum follow-up of 180 days. Secondary outcomes were improvement in visual acuity.
Results:
A total of 35 eyes of 31 patients were identified. Indications for scleral-fixated IOL included dislocated IOL
(18 eyes), subluxed or dislocated crystalline lens (6 eyes),aphakia with poor capsular support (3 eyes) , malpositioned ACIOL (2 eyes) and uveitis–glaucoma–hyphema syndrome (1 eye).
Twenty-six eyes underwent concurrent complete pars plana vitrectomy.
No major intraoperative complications were noted.
SFIOL was decently centered in all cases.
7 patients had rise in IOP postoperatively managed with medical therapy, 2 of them underwent glaucoma surgery. Other postoperative complications noted were vitreous haemorrhage in 2 eyes, hyphema in 1 eye, cystoid macular oedema in 2eyes.
All patients with hyphema, hypotony, cystoid macular oedema or ocular hypertension were managed medically. There were no cases of postoperative endophthalmitis, suture breakage, conjunctival or scleral inflammation, suture granuloma formation, IOL dislocation, IOL capture within iris, IOL tilt, suprachoroidal haemorrhage, uveitis–glaucoma–hyphema syndrome or persistent postoperative inflammation in the follow-up period..
1 eye with pre-existing chronic macular hole developed retinal detachment requiring reintervention.
Mean visual acuity improved from 1.52logmar preoperatively to 0.64; 0.44logmar postoperatively at 3 and 6 months(p<0.001). Mean follow-up was 12 months 17days(range 3months–3years).
Discussion
Polypropylene suture, a monofilament polymer composed of propene, has been the most commonly used suture material for scleral-fixated IOL techniques.4 9–13 However, concerns regarding suture breakage and degradation are of special interest, especially in younger patients.9 10 Rates of suture-related complications have varied in the literature. Vote et al 4 reported outcomes and complication rates in 61 eyes that underwent combined PPV and trans-scleral sutured PCIOL with a mean follow-up of 6 years. Overall, 17 (27.9%) eyes experienced breakage of 10-0 polypropylene suture at one point in the study period, requiring reoperations in all cases to address this complication. In a report describing outcomes of scleral-fixated IOLs in a paediatric population also using 10-0 polypropylene suture, Asadi and Kheirkhah10 reported late suture breakage in 6 of 25 eyes (24%) with mean follow-up of 6.75 years, with breakage occurring 7–10 years post implantation. The mechanism of polypropylene suture breakage has been attributed to both suture cutting by haptic positioning holes14 and degradation of the polypropylene material itself.9 15
The authors have suggested using sutureless scleral fixation techniques16–18 as well as alternative suture materials, such asGore-Tex or larger diameter (9-0) polypropylene,7 9 12 in order to minimise this risk of suture-related complications.
To our knowledge, this is the largest series evaluating the visual outcomes and short-term safety profile of Gore-Tex suture in a scleral-fixated IOL technique and, in general, use of Gore-Tex suture for an ophthalmic indication. While common in nonophthalmic surgery, use of Gore-Tex suture in the eye is currently off-label. Advantages of this suture include high tensile strength, high visibility due to its white colour, minimal inflammatory response and minimal memory, which makes it exceptionally easy to manipulate. To date, no reports of suture degradation have been reported in the ophthalmic or nonophthalmic literature.
In this series, overall VA improved in a statistically significant manner with gains observed for all surgical indications. Complications were consistent with prior studies evaluating short-term outcomes of scleral-fixated IOLs.2 4 11 19 In regards to suture-related complications, no cases of IOL dislocation, IOL decentration, IOL tilt or suture breakage were observed in this series, including the 34 eyes with >1 year of follow-up. Formal evaluation of IOL tilt with ultrasound biomicroscopy and anterior segment optical coherence tomography was not completed, however, as such tests were not deemed necessary by the examining physicians. Subsequent study with longer duration of follow-up and use of these diagnostic tests will be important to further establish IOL stability and use of this suture material for scleral fixation. The goal of the present study was to evaluate short-term outcomes of Gore-Tex suture in a scleral-fixated IOL technique. Thus far, no finding from this short-term retrospective review (mean follow-up of 325 days) suggests that use of Gore-Tex is associated with a unique, negative outcome or complication, and may be used effectively with concurrent PPV, DSEK or PK surgery.
This study has several limitations, however, many of which are inherent to its retrospective nature. Finally, because of the relatively short follow-up duration in the current study, long-term complications cannot be addressed.
In summary, we report the clinical outcomes and short-term safety profile of scleral-fixated IOLs using Gore-Tex suture. Use of Gore-Tex appears to be safe and effective. Patients experienced positive visual outcomes with a low rate of adverse events. Ultimately, long-term evaluation of outcomes and complications will be necessary to determine the advantages of using Gore-Tex suture compared with other suture materials for scleral fixation. Similarly, prospective, comparative trials would be necessary to determine superiority of this technique compared with alternative IOL implantation strategies.
REFERENCES
1 Holt DG, Young J, Stagg B, et al. Anterior chamber intraocular lens, suturedposterior chamber intraocular lens, or glued intraocular lens: where do we stand?Curr Opin Ophthalmol 2012;23:62–7.
2 Wagoner MD, Cox TA, Ariyasu RG, et al. Intraocular lens implantation in theabsence of capsular support: a report by the American Academy of Ophthalmology.Ophthalmology 2003;110:840–59.
3 Hannush SB. Sutured posterior chamber intraocular lenses: indications andprocedure. Curr Opin Ophthalmol 2000;11:233–40.
4 Vote BJ, Tranos P, Bunce C, et al. Long-term outcome of combined pars planavitrectomy and scleral fixated sutured posterior chamber intraocular lens implantation. Am J Ophthalmol 2006;141:308–12.
5 Rim Y, Laing ST, McPherson DD, et al. Mitral valve repair using ePTFE sutures for ruptured mitral chordae tendineae: a computational simulation study. Ann Biomed Eng 2014;42:139–48.
6 Shimamoto T, Komiya T, Sakaguchi G. Half-leaflet suspension with a thin Gore-Tex suture for aortic leaflet prolapse. Ann Thorac Surg 2011;91:907–8.
7 Nottage JM, Bhasin V, Nirankari VS. Long-term safety and visual outcomes of transscleral sutured posterior chamber IOLs and penetrating keratoplasty combined with transscleral sutured posterior chamber IOLs. Trans Am Ophthalmol Soc 2009;107:242–50.
8 Khan MA, Gerstenblith AT, Dollin ML, et al. Scleral fixation of posterior chamber intraocular lenses using gore-tex suture with concurrent 23-gauge pars plana vitrectomy. Retina Phila Pa 2014;34:1477–80.
9 Price MO, Price FW Jr, Werner L, et al. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg 2005;31:1320–6.
10 Asadi R, Kheirkhah A. Long-term results of scleral fixation of posterior chamber intraocular lenses in children. Ophthalmology 2008;115:67–72.
11 Bading G, Hillenkamp J, Sachs HG, et al. Long-term safety and functional outcome of combined pars plana vitrectomy and scleral-fixated sutured posterior chamber lens implantation. Am J Ophthalmol 2007;144:371–7.
12 McAllister AS, Hirst LW. Visual outcomes and complications of scleral-fixated posterior chamber intraocular lenses. J Cataract Refract Surg 2011;37:1263–9.
13 Mimura T, Amano S, Sugiura T, et al. 10-year follow-up study of secondary transscleral ciliary sulcus fixated posterior chamber intraocular lenses. Am J Ophthalmol 2003;136:931–3.
14 Parekh P, Green WR, Stark WJ, et al. Subluxation of suture-fixated posterior chamber intraocular lenses a clinicopathologic study. Ophthalmology 2007;114:232–7.
15 Drews RC. Polypropylene in the human eye. J Am Intra-Ocul Implant Soc 1983;9:137–42.
16 Prenner JL, Feiner L, Wheatley HM, et al. A novel approach for posterior chamber intraocular lens placement or rescue via a sutureless scleral fixation technique. Retina Phila Pa 2012;32:853–5.
17 Ohta T, Toshida H, Murakami A. Simplified and safe method of sutureless intrascleral posterior chamber intraocular lens fixation: Y-fixation technique. J Cataract Refract Surg 2014;40:2–7.
18 Yamane S, Inoue M, Arakawa A, et al. Sutureless 27-gauge needle-guided intrascleral intraocular lens implantation with lamellar scleral dissection. Ophthalmology 2014;121:61–6.
19 Johnston RL, Charteris DG, Horgan SE, et al. Combined pars plana vitrectomy and sutured posterior chamber implant. Arch Ophthalmol 2000;118:905–10.
20 Soiberman U, Pan Q, Daoud Y, et al. Iris suture fixation of subluxated intraocular lenses. Am J Ophthalmol 2015;159:353–9.
21 Wilgucki JD, Wheatley HM, Feiner L, et al. One-year outcomes of eyes treated with a sutureless scleral fixation technique for intraocular lens placement or rescue. Retina 2015;35:1036–40.
22 McKee Y, Price FW, Feng MT, et al. Implementation of the posterior chamber intraocular lens intrascleral haptic fixation technique (glued intraocular lens) in a United States practice: Outcomes and insights. J Cataract Refract Surg 2014;40:2099–105.
23 Chan TCY, Lam JKM, Jhanji V, et al. Comparison of outcomes of primary anterior chamber versus secondary scleral-fixated intraocular lens implantation in complicated cataract surgeries. Am J Ophthalmol 2015;159:221–6.e2.
24 Sawada T, Kakinoki M, Sawada O, et al. Closure of sclerotomies after 25- and 23-gauge transconjunctival sutureless pars plana vitrectomy evaluated by optical coherence tomography. Ophthalmic Res 2011;45:122–8.
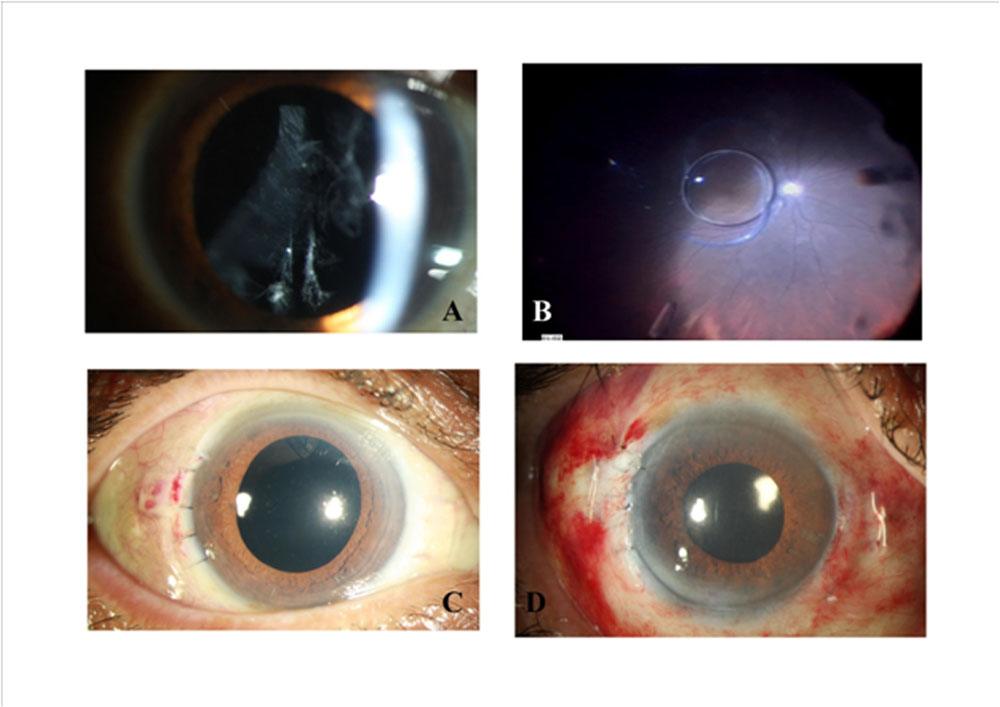
1: Case 3 with dislocated IOL (A&B). C&D showing well centred SFIOL at 3 and 6 months.
Leave a Comment