
Dr. Jayasri Kanthalu Narayanamoorthy, J20067, Dr. Kowsalya Akkayasamy, Dr. Mahesh Kumar
Abstract: Metastasis to the Brain is the most feared complication of systemic cancer.It presents with various neuroophthalmic manifestation. Secondaries are the most common intracranial tumor in adults. Common primary tumors are Lung and Breast. Although, Brain metastasis develops after the diagnosis of primary tumor, in 20% it manifests before the primary tumor is found. Hereby reporting a case series of 10 patients with systemic cancer who presented to Neuroophthalmology Department in a tertiary eye care center with various symptoms of headache, defective vision and diplopia. Of these, 8 patients were known cancer patients on treatment. All were subjected to MRI brain, and underlying carcinoma with Brain metastasis was diagnosed, thus paving way to save the life of the patient.
Conclusion: Ocular symptoms may be the chief complaint of Brain metastasis and it should be considered if there is no intraocular cause. Early diagnosis is extremely important for appropriate treatment.
INTRODUCTION
Metastasis to the brain is the most feared complication of systemic cancer. It presents with various neuroophthalmic manifestations. Secondaries are the most common intracranial tumors in adults. Common primary tumors are Lung and Breast.
Brain Metastases in Order of Frequency:
Lung (39%)
Breast(17%)
Melanoma (11%)
Although, Brain metastasis develops after the diagnosis of primary tumor, in 20% it manifests with neuroophthalmic presentation, before the primary tumor is found.
AIM
Analysis of 10 patients with systemic cancer who presented to Neuro ophthalmology department with complaints of Headache, Defective vision and Diplopia.
MATERIALS AND METHODS
Report a case series of 10 patients with systemic cancer .Of these 8 patients were known cancer patients on treatment. Two patients who presented us with Neuroophthalmic manifestation without known primary cancer.
For all patients detailed Neuro ophthalmic examination was done.
- Visual Acuity, Colour vision, Central fields
- Neurological Examination including Cranial nerves examination
- Anterior segment (Pupil) & Fundus examination
- Diplopia &Hess charting (if required)
5.Systemic examination & Neuro Imaging
CASE REPORTS
CASE-1
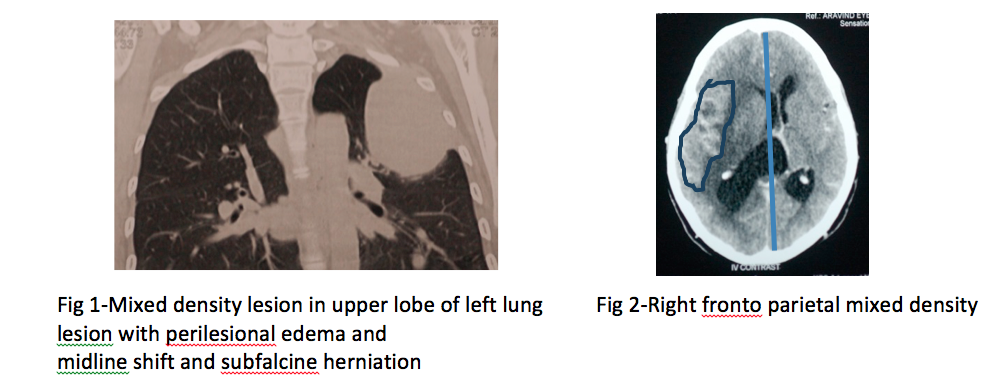
A 28 year old female presented a history of headache one and half years,slowly progressive diminution of vision since 6 months.Her past history revealed that she had consulted elsewhere for headache 2 years back.When old records were checked,she was a known case of bronchogenic carcinoma on treatment with oncologist. CT Chest showed mixed density lesion in upper lobe of left lung 8×5.08 cm in size(Figure 1). On examination her vision was perception of light in both eyes. Pupils were sluggishly reacting to light and fundus showed secondary optic atrophy in both eyes. Patient was advised contrast enhanced MRI Brain which revealed, large mixed density lesion 5×3.8 cm in right fronto-parietal region with intense perilesional edema and midline shift with subfalcine herniation seen towards left side suggestive of brain secondaries(Figure 2).Patient was explained about poor visual prognosis and referred to an Oncologist.
CASE-2
A 60 year old female presented with a history of headache, hearing loss and inability to close the right eye since 7 months. Her past history revealed that she had consulted elsewhere for headache. On examination her best corrected visual acuity in both eyes 6/9. Anterior segment examination of right eye showed lagophthalmos with good bells phenomenon with restriction of abduction movement. Pupils were normal in both eyes. Anterior segment of left eye was normal. In both eyes, fundus was normal. Corneal sensation of right eye was diminished and right sided deafness was present. A probable diagnosis of right multiple cranial nerve palsy was made out and patient was subjected to contrast enhanced MRI/MRA Brain. It showed large expansile and destructive lesion (measuring 6.34×4.40×3.51cm) replacing the right postero lateral clivus, petrous apex, lateral wall of sphenoid sinus and middle cranial fossa with engulfment of structure of cavernous sinus, Meckal”s cave, Dorello”s canal and internal auditory meatus. Suspecting secondaries, a search was done for the primary lesion. Imaging of chest revealed heterogenous mixed density lesion in right lung middle lobe with irregular nodular surface and infiltrating the adjacent pericardium with minimal passive collapse of lung parenchyma measuring 4.7×3.3cm.The final diagnosis was made as primary of Bronchogenic carcinoma with brain secondaries. Patient was advised right eye tapping at night, lubricating eye drops and eye ointment. Finally patient was referred to Oncologist.
CASE-3
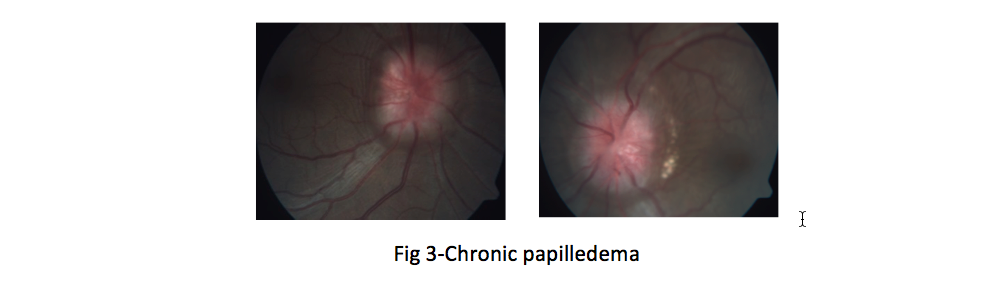
A 36 year old female presented with complaints of sudden diminution of vision for 10 days. Past history revealed that she had consulted locally for headache 5 months back. She underwent series of blood investigation and finally diagnosed as Adenocarcinoma of left lung with brain secondaries. Six cycles of chemotherapy followed by radiotherapy was given. On examination her visual acuity was perception of light in both eyes .Anterior segment examination was normal with sluggishly reacting pupils in both eyes. Fundus examination of both eyes showed chronic papilledema(Figure 3).Patient was advised Neuoimaging which revealed enhancing mixed signal intensity lesion with marginal nodularity in right posterior temporal lobe measuring 4.3×3.4 cm with perilesional edema and compression of adjacent ventricular system and sulci. Final diagnosis was made as primary of bronchogenic carcinoma with right temporal lobe metastasis and papilledema. Poor visual prognosis was explained to the patient. Patient was referred to Oncologist regarding reduction of high intracranial tension for lumbar puncture after getting Neurologist opinion.
CASE-4
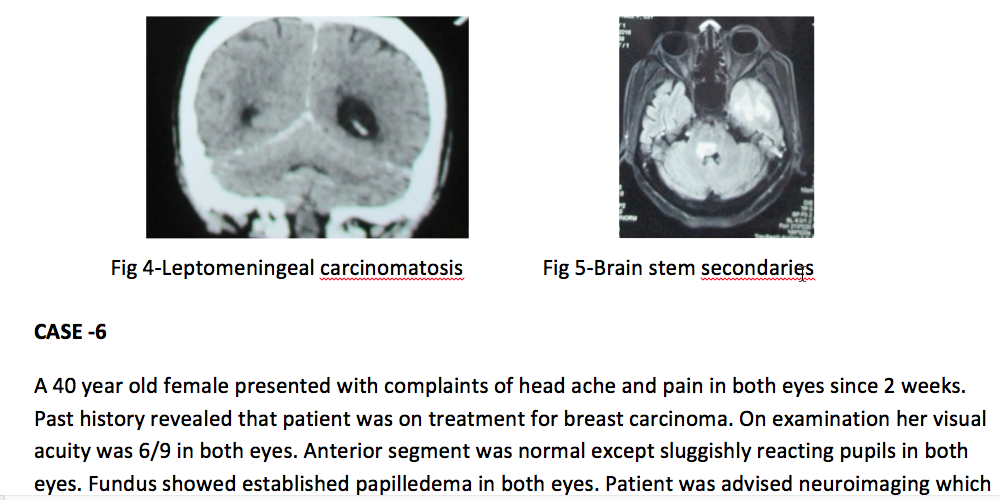
A 32 year old female presented with complaints of sudden diminution of vision since 10 days. Past history revealed that she was a known case of Breast carcinoma operated and treated with chemotherapy and radiotherapy. On examination her visual acuity was hand movements in both eyes.Pupils were sluggishly reacting to light. Fundus showed normal in both eyes. Probable diagnosis of Retro bulbar neuritis was made in both eyes. Patient was advised neuroimaging to rule out brain secondaries which showed Leptomeningeal carcinomatosis of cerebellum with hydrocephalus and coexisting retrobulbar neuritis and sequelae (Figure 4).The patient was explained about poor visual prognosis. Patient was referred to Oncologist and suggested Intravenous Methyl prednisolone 1gm od for 3 days followed by oral steroids under guarded visual prognosis.
CASE-5
A 60 year old female presented with complaints of diplopia for 15 days. History of inability to close the right eye for past 6 months. Past history revealed that patient underwent mastectomy for breast carcinoma followed by chemotherapy and radiotherapy was given for lung and vertebral metastasis. On examination her visual acuity was 6/9 in both eyes. Anterior segment of right eye revealed lagophthalmos with poor bell’s phenomena and restriction of abduction movement. Pupils were normal in both eyes. Anterior segment of left eye was normal. Fundus was normal in both eyes. Patient was advised right eye lubricating eye drops and ointment and temporary lateral tarsorraphy to prevent exposure keratitis. Probable diagnosis of right multiple cranial palsy was made and patient was subjected to neuro imaging for brain secondaries. MRI brain showed multiple cerebral and brain stem secondaries(Figure 5). Patient was referred to oncologist for further treatment.
CASE -6
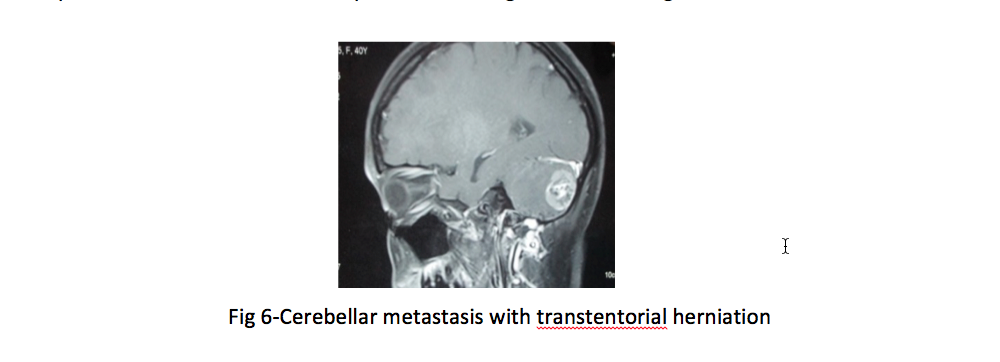
A 40 year old female presented with complaints of head ache and pain in both eyes since 2 weeks. Past history revealed that patient was on treatment for breast carcinoma. On examination her visual acuity was 6/9 in both eyes. Anterior segment was normal except sluggishly reacting pupils in both eyes. Fundus showed established papilledema in both eyes. Patient was advised neuroimaging which showed cerebellar metastasis with transtentorial cerebellar herniation (Figure 6) and mild obstructive hydrocephalus. Patient was referred to neurosurgeon for VP shunt to reduce the intra cranial tension. Patient underwent VP shunt and came for review. Papilledema was resolved in both eyes and patient was advised to follow up with neurosurgeon and oncologist.
CASE-7
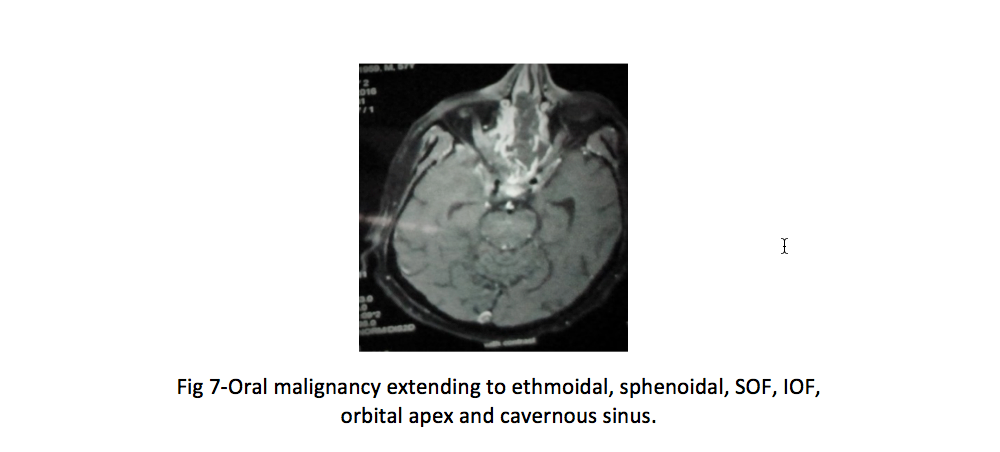
A 57 year old male presented with complaints of binocular diplopia on left gaze since 4 days. Patient was on treatment for oral carcinoma since 1 year. On examination his visual acuity was 6/6 in both eye. Anterior segment of both eyes were normal except abduction restriction in left eye. Fundus was normal in both eyes. Probable diagnosis of left eye 6th nerve palsy was made. Patient was advised neuroimaging to rule out secondaries. Patient lost follow up. After 2 months he came with complaints of sudden diminution of vision in both eyes. His visual acuity was perception of light. Fundus was normal in both eyes. Neuroimaging revealed recurrent oral malignancy extending to nasal cavity, ethmoidal and sphenoidal sinuses, SOF, IOF, orbital apex and cavernous sinus(Figure 7). Patient was referred to oncologist for further treatment.
CASE-8
A 50 year old male with no systemic illness presented with complaints of diplopia associated with headache since 1 week. History of slurring of speech was present. On examination his visual acuity of both eyes 6/9. Anterior segment examination was normal in both eyes except restricted abduction in left eye. Fundus was normal in both eyes. Probable diagnosis of left eye 6th nerve palsy was made. Patient was advised neuroimaging which showed large expansile destructive lesions measuring 5.6 x 5.3 x 5.1 cm involving sphenoidal sinus, clivus and encroaching retro clival space, prepotine space and diagnosed as sphenoethmoidal malignancy with skull base extension(Figure 8). Patient was referred to Oncologist.
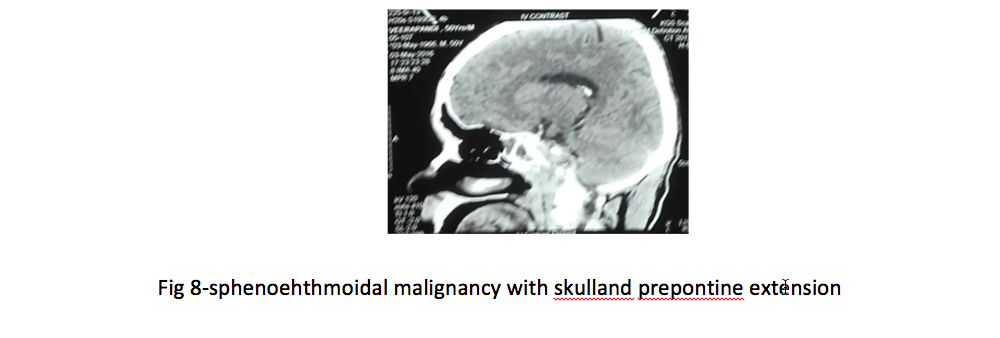
Fig 8-sphenoehthmoidal malignancy with skulland prepontine extension
CASE-9
A 43 year old female presented with complaints of head ache and giddiness since 20 days. Past history revealed that patient had thyroid malignancy on treatment. On examination her visual acuity was 6/6 in both eyes. Anterior segment examination of both eyes were normal. Fundus showed established papilledema in both eyes. Patient was advised neuroimaging which revealed multiple necrotic and haemorrhagic secondaries in both cerebral hemispheres with intense edema with compression of ventricular system. Patient was referred to Oncologist.
CASE-10
A 78 year old male presented with complaints of diplopia associated with head ache since 4 days. Patient was on treatment for hepatocellular carcinoma. On examination his visual acuity was 6/9 in both eyes. Anterior segment was normal in both eyes except restriction of abduction in left eye. Probable diagnosis of left eye 6thnerve palsy was made and patient was subjected to neuroimaging. It showed destructive lesion involving left side clivus with infiltration of Dorello’s canal and invasion of left cavernous sinus and Meckel’s cave causing 6th nerve palsy. Patient was referred to Oncologist for further treatment.
DISCUSSION
Metastasis to the brain is the most feared complication of systemic Carcinoma. Secondaries are the commonest intracranial tumor in adults. Cerebral metastasis occurs in 15% ofpatients with cancer. In 15% of the patients, primary site remains unknown (1).Multiple, large autopsy series suggest that, in order of decreasing frequency lung, breast, melanoma, renal, and colon cancers are the most common primary tumor to metastasize to the brain. The metastases to the brain accounts for 20%of cancer deaths annually, a rate that can be traced to an increase in the median survival of patients with cancer because of modern therapies, increased availability of advanced imaging techniques for early detection (2).
In adults, the most common primary tumor responsible for intracranial metastasis is lung. Although in the majority of patients (80%), brain metastasis develops after the diagnosis of primary tumor, in some patients it manifests before the primary tumor is found. For patients who present with brain metastasis without a known primary, the lung should be the primary focus of evaluation. Sixty percent of these patients will have a primary lesion in the lung (3). Among the symptoms, headache occurs in 40-50% of patients with brain metastasis (4).
Metastatic brain tumor have been reported to be at least four times as common as primary brain tumor, and breast cancer is known to be the second most common cause of brain metastasis (5,6).Yen et al (7) reported that the incidence of brainstem involvement in patients with breast cancer metastasis to the brain was as high as 12.4%, higher than that in patients with any other type of cancer. Lee et al (8) reported that 28% of cases of brain metastasis in breast cancer showed a single metastatic lesion, supporting the idea that a single brain lesion does not necessarily suggest a primary tumor. Metastatic breast carcinoma is the most common primary tumor to metastasize to ocular structures. The incidence of ocular structures among patients with breast carcinoma in clinical series has been reported to vary between 8 and 10% (9).
Metastasis to the brain is a devastating and common consequence for patients with malignant melanoma. Cranial nerve palsies and visual deficits are the common presenting clinical features in these patients. Malignant sino nasal tumor have a reported incidence of 1 in 100000 individuals yearly with only about 9% of these originating in the ethmoidal sinus (10). Reported ophthalmic manifestation of sinonasal undifferentiated Carcinoma include periocular swelling, pain, variable Nerve palsies, Visual field loss, Compressive optic Neuropathy. Paraneoplastic syndromes are complexes of signs and symptoms incancer-bearing patients resulting from dysfunction of tissues remote from the site of a malignant neoplasm orits metastases. Paraneoplastic optic neuropathy may produce subacute, progressive, painless bilateral visual loss.
Metastatic brain tumor spread by haematogenous route either to the skull bones from where it may spread to the subarachnoid space, brain or both or it may metastasize directly to the brain parenchyma or to the subarachnoid space as well as to the orbit. Tumor cells reach the brain through arterial circulation, most commonly from the lung, by either a primary lung cancer or a lung metastasis. They most commonly involve the grey-white junction (11). The location of metastases in the brain roughly correlates with the blood flow to that area. Metastases are found in the cerebral hemispheres (80%), in the cerebellum (15%), and 5% in the brain stem (12).When brain metastases are discovered, 29% are found at the time of diagnosis of the primary tumor (synchronous) and in 80% of cases after the primary diagnosis of the cancer (metachronous presentation). Headache, giddiness, new onset seizures, visual disturbances, should warrant Imaging of Brain.
New onset of seizures in a patient older than35 years is highly suggestive of primary or metastatic disease. Contrast Gadolinium enhanced MRI is more sensitive than CT scan. It detects small brain metastasis, particularly lesions situated in the posterior fossa. Metastases are seen radiologically as ring enhancing lesions located at the grey white matter junction followed usually by significant edema. A variety of neuroophthalmological features including midbrain syndromes, nuclear third nerve palsies, defects in tracking and saccades are known to occur.
Neoplasm is known to be one of the causes of abducens nerve palsy and internuclear ophthalmoplegia. Horner’s syndrome may be seen when the posterior fossa is involved. Involvement of the visual pathway may result in visual field defects, loss of colour vision, visual agnosia, and loss of acuity (13-14). The pineal gland may be the site of metastases, presenting with parinaud’s syndrome. The most common source is both small and non-small- cell carcinoma of the lung (15,16 ). The best diagnostic test for brain metastases is contrast enhanced MRI (17,18 ).If the clinical history is typical and lesions are multiple, usually there is little doubt regarding the diagnosis. It is important that metastases be distinguished carefully from primary brain tumours(benign or malignant), abscesses, cerebral infarction, and haemorrhages. One study (19) has shown that false positive scan be upto 11%. The treatment for metastatic intraparenchymal brain tumours depend on the nature and extent of the primary process, the nature and severity of the neurological or visual symptoms and signs, and the life expectancy of the patient. Radiation therapy, stereotactic radiosurgery, chemotherapy, and surgical therapy all may play a role both individually or in combination (20,21 ).
CONCLUSION
Brain metastasis presents with various Neuroophthalmic manifestation. It manifests as nerve palsy, optic neuritis, papilledema and optic atrophy depending on the severity of primary cancer and site of metastases. It may be the initial presentation, which lead to the diagnosis of a primary cancer elsewhere, explaining the importance of thorough evaluation.
References
- Patchell RA. The management of brain metastases. Cancer Treat Rev 2003;29:533–540
- Russell DC, Rubinstein LJ. Pathology of Tumours of the Nervous System. Ed 5. Baltimore, Williams & Wilkins, 1989:352–360.|
- Delattre JY, Krol G, Thaler HT, et al. Distribution of brain metastases. Arch Neurol 1988; 45: 741–744.
- Posner JB. Clinical manifestations of brain metastases. In: Weiss L, Gilbert HA, Posner JB (eds.), Brain Metastases. GK Hall: Boston, 1980; 189–207.
- Kaal EC, Vecht CJ. CNS complications of breast cancer: current and emerging treatment options. CNS Drugs 2007;21:559-79.
- Zimm S, Wampler GL, Stablein D, et al. Intracerebral metastases in solid-tumor patients: natural history and results of treatment. Cancer 1981;48:384-94.
- Yen CP, Sheehan J, Patterson G, Steiner L. Gamma knife surgery for metastatic brainstem tumors. J Neurosurg 2006;105: 213-9.
- Lee SS, Ahn JH, Kim MK, et al. Brain metastases in breast cancer: prognostic factors and management. Breast CancerRes Treat 2008;111:523-30.
- BULLOCK jd, Yanes B.Ophthalmic manifestations of metastatic brain cancer. Ophthalmlogy 1980;87:961-73.
- Shao W, Vasanth A.eMedicine from WebMD: Malignant Tumours of the Nasal cavity,2006.
- Hwang T, Close TP, Grego JM, et al. Predilection of brain metastasis in grey and white matter junction and vascular border zones.Cancer 1996;77:1551–55.
- Delattre JL, Krol G, Thaler HT, et al. Distribution of brain metastases. Arch Neurol 1988;45:741–44.
- Stevenson GC, Hoyt WF. Metastasis to midbrain from mammary carcinoma: Cause of bilateral ptosis and ophthalmoplegia. JAMA 1963;186:514–16.
- Growdon JH, Winkler GF, Wray SH. Midbrain ptosis: A case with clinicopathologic correlation. Arch Neurol 1974;30:179–81.
- Tan E, Can U, Kansu T, et al. Parinaud syndrome due to solitary pineal metastasis.Eur Neurol 1990;30:200–202.
- Weber P, Shepard KV, Vijayakumar S, Metastases to the pineal gland. Cancer 1989;63:164–65.
- Sze G, Milano E, Johnson C, et al. Detection of brain metastases: comparison of contrast- enhanced MR with unenhanced MR andenhanced CT.AJNR 1990; 11:785–91.
- Davis PC, Hudgins PA, Peterman SB, et al. Diagnosis of cerebral metastases: double dose delayed CT vs contrast enhanced MR imaging. AJNR 1991; 12: 293–300.
- Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases to the brain.N Engl J Med 1990; 322: 494–500.
- Buckner J. Surgery, radiotherapy, and chemotherapy for metastatic tumors of the brain. Curr Opin Oncol 1992;4:518–24.
- Black PM. Solitary brain metastases: Radiation, resection, or radiosurgery? Chest 1993;10:367S– 369S.
Leave a Comment