
Dr. Hetal Mehta Khandge,
M16020, Dr. Akshay Kothari, Dr. Kelkar Jai Aditya, Dr. Aditya Kelkar
Acknowledgement: We acknowledge the assistance of Dr.Sabyasachi Sengupta from Sengupta’s Research Academy in statistics and content editing for this manuscript.We also acknowledge the inputs from Dr. Rajesh Fogla and Dr.ShrikantKelkar
Introduction:
The Yamane’s technique of fixating a three-piece IOL to the sclera in a sutureless
manner by creating flanges is a truly novel technique that has the potential to revolutionize
aphakia management.1,2 This transconjunctival technique is independent from scleral flaps, tunnels, sutures and fibrin glue, has short learning curve and faster postoperative recovery. However use of 30-gauge thin wall needle to engage and exteriorize the haptic, as recently described by Yamane et al, is not readily available across the world.1,2 Here, we report our initial experience of modified transconjunctival intrascleral IOL fixation technique using 27 gauge needle for the three piece IOL options available in our country.
Methods:
The study was approved by the Institutional Ethics Committee and adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from all patients. We performed a prospective interventional study of consecutive eyes that received scleral fixation of a three piece IOL in cases of aphakia due to PC Rent or Nucleus Drop and subluxated or dislocated IOL from September 2016 to December 2016. We proceeded with the SFIOL implantation as a secondary procedure, a minimum of one month after the previous cataract surgery. We excluded patients with visually significant coexistent pathology like corneal scars, macular pathology, glaucoma etc.
Prior to recruitment, all patients underwent comprehensive ophthalmic evaluation including Uncorrected and Best Corrected Visual Acuity (UCVA, BCVA), GoldmannApplanation Tonometry (GAT), Slit Lamp Examination (SLE) to determine adequacy of capsular and zonular support, corneal clarity and vitreous in the anterior chamber, fundus examination to rule out peripheral retinal tears, specular Microscopy (SP – 1P Topcon, Japan) and Optical Coherence Tomography (OCT) (DRI OCT 1 Topcon, Japan) of the macula. All IOL powers were calculated by SRK-T formula using the IOL Master 700 apparatus (Carl Zeiss Meditec, XX, USA). The target refraction in all cases was -0.50 dioptres.
Surgical technique:
Under peribulbaranesthesia conjunctival entry spots were marked 180 degrees apart with a marker at 3’o clock and 9’o clock meridians, two mm from the limbus. All patients underwent anterior vitrectomy and those with significant subluxation or dislocation of the nucleus or IOL underwent complete parsplanavitrectomy before SFIOL implantation. Following adequate vitrectomy, the three – piece IOL was either injected with the cartridge and injector into the eye via the limbal incision or in cases with prior IOL explantation, directly with McPherson’s forceps through a sclerocorneal tunnel. Using the previous marking, an angled sclerotomy was made with 27-gauge needle, two mm from the limbus to engage the leading haptic, keeping it tangential with the iris plane to avoid ciliary body injury. A 25G end gripping forceps was introduced from a paracentesis to insert the tip of the leading haptic into the lumen of the 27 gauge needle. The haptic was externalized and the tip was heated with a thermal cautery to create a flange (fig 1), which was pushed back and fixed intrasclerally. The same technique was repeated 180 degrees opposite to fixate the trailing haptic. In case of sclerocorneal tunnel McPherson’s forceps was used to insert the tip of the trailing haptic into the lumen of 27 gauge needle. Viscoelastic material was aspirated and anterior chamber was formed with BSS. If a parsplanavitrectomy was performed, the ports were removed at the end and integrity of the incisions ensured. Following surgery, the patients’ eye was padded and shifted to the recovery room. The eye pad was removed after six hours and topical nepafenac eye drops were given three times a day for two weeks. Topical moxifloxacin eye drops were prescribed three times/day for four weeks and topical prednisolone 1% eye drops were given in tapering dose for six weeks.
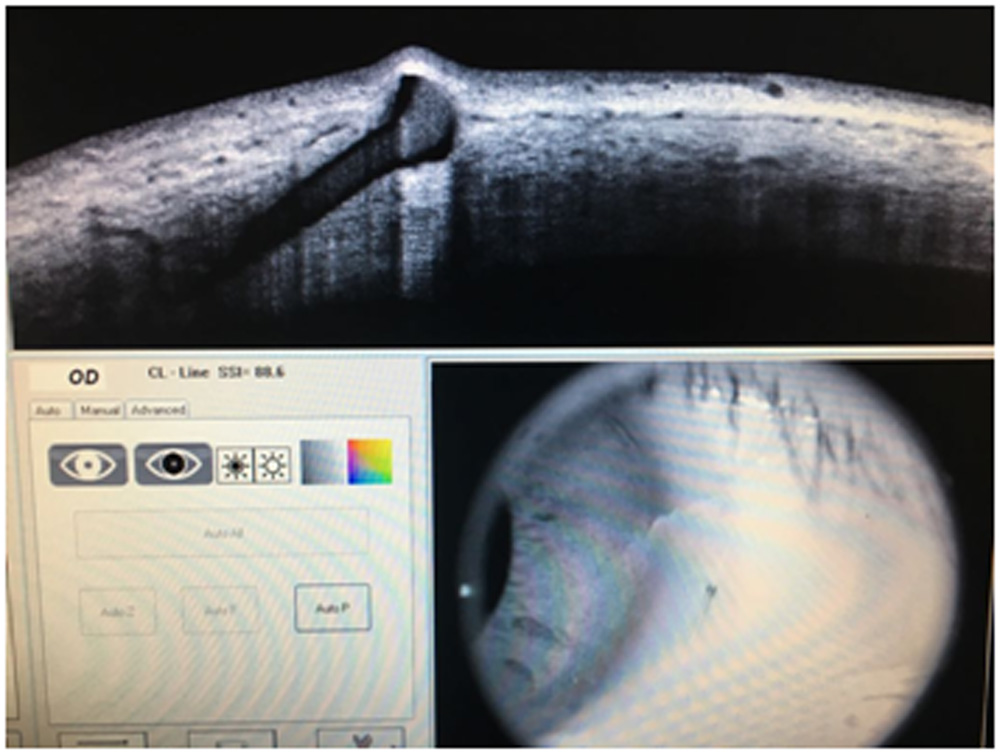
UCVA, BCVA, GAT, SLE, Specular Microscopy, OCT, Serial digital slit lamp images of the eye with full pupillary dilatation (fig 2) and anterior segment OCT (RTVue-100, OptovueInc, USA) to assess the position of the flange were done at one week (fig 3), six week and six month. Descriptive data from patients who lost follow up were utilized to report on the intraoperative experience but were excluded from the postoperative statistical analysis. All the data was entered in Microsoft Excel sheets and were analyzed using STATA 12.0 I/C (Fort worth, Texas).Continuous variables were described as means + standard deviation or median and interquartile range (IQR) and categorical variables were described as proportions. Visual acuity was converted to logarithm of minimum angle of resolution (logMAR) for analysis. Pre and postoperative data was analysed using the paired t test. A p value of <0.05 was considered statistically significant.
Results:
The study comprised of 31 eyes of 31 patients undergoing SFIOL by the modified Yamane’s
technique. Twenty-three (75%) patients returned for follow up at six weeks and 21 (67%) visited at six months follow up.
Demographics and indications: The mean age of subjects was 57+16.9 years (median=60 years, IQR=52-68 years) and 23 were men (74%). SFIOL was performed for aphakia following complicated cataract surgery in 10 eyes (32%), along with lensectomy for subluxated/dislocated cataract in six eyes (19%) and along with IOL explantation for subluxated/dislocated IOL in 15eyes (48%). Overall, 13 eyes (42%) underwent anterior vitrectomy at the time of SFIOL placement and the remaining 18 eyes (58%) underwent parsplanavitrectomy.
Outcome: Uncorrected visual acuity improved from median of 1.48 logMAR units (IQR=1.3 – 2 logMAR) at baseline to 0.6 logMAR (IQR=0.5 – 0.8logMAR) at one week post op (p<0.001) period and improved further to 0.3 logMAR (IQR=0.2 – 0.4 logMAR) at six weeks (p<0.001 compared to baseline, p=0.002compared to one week) and was maintained at three and six months follow up. The best-corrected vision was 0.3 logMAR (IQR=0.2-0.6) preoperatively and was maintained at six weeks (median=0.2 logMAR, IQR=0.2-0.4) and six months (p=0.83).
Eyes with IOL explantation at time of SFIOL had greater refractive error (astigmatism) but this was not significantly different from those without IOL explantation(p=0.24). These eyes had comparatively lower vision (0.6+0.5 logMAR) at six weeks, three months and six months compared to those without IOL explantation (0.33+0.2 logMAR), though this difference was not statistically significant (p=0.08). Overall, refractive median error at the end of six weeks was -0.75 D sphere (IQR=-0.5 to -1.00 Dsphere) and median cylinder was -1.3 D sphere at 80 degrees (IQR= -1.00 to -1.8D). There was no appreciable change in spherical and cylindrical correction between six weeks and six months follow up. Mean preoperative IOP was 17.6+7.1 mmHg and it rose to 21.2+9.1 mmHg at one week (p=0.06) but returned to normal levels at six weeks follow up (14.9+4.2, p=0.16).. There was no significant change in endothelial cell density (preop=2734+571 cells/mm3vs. postop=2491+904 cells/mm3, p=0.34) and macular thickness on OCT (preop=241+39 microns vs. 248+46 microns, p=0.31) at six month follow up. None of the eyes developed clinical or OCT based cystoid macular edema at six months.
Complications: None of the eyes experienced any intraoperative complications. Transient IOP rise above 21 mmHg was seen in 12 eyes (39%) but all these were managed conservatively with topical anti-glaucoma medications. Two eyes had mildly decentered SFIOL but were managed with appropriate refractive correction. One eye had persistent postoperative vitreous hemorrhage and underwent parsplanavitrectomy at six weeks with excellent visual recovery.
Discussion:
Many techniques have evolved over the decades ranging from anterior chamber IOL implantation, either supported on the anterior iris surface or the anterior chamber angle,[3,4] scleral fixated IOLs (SFIOL) anchored either using sutures[5-7] or by sutureless methods[8] and retropupillary iris claw IOL fixation.[9] Each technique has its merits and demerits, however, scleral fixated IOL are the most preferred technique in view of their long term safety and efficacy.[10] Compared to sutured SFIOL, performing sutureless SFIOL fixation as described by Scharioth is relatively simple where the exteriorized haptics of a regular three-piece IOL are fixated into scleral pockets.[11] Sindal has shown comparable results using sutured SFIOL and sutureless SFIOL for post-cataract and post-traumatic aphakia. [12] Similarly, Agarwal’s technique of glued SFIOL exteriorizes the IOL haptic under a partial thickness scleral flap, which is then secured using fibrin glue.[13,14] Though technically less challenging than sutured SFIOL, these techniques of sutureless SFIOL involve conjunctival dissection and related patient discomfort. Additionally, it is always challenging to ensure adequate length of haptic fixation inside the scleral tunnels or under scleral flaps. Long term impact of the exteriorized IOL haptic and fibrin glue on the scleral integrity and stability of IOL fixation is unknown at present.
To address these concerns, Yamane described the elegant use of a 30-gauge thin wall needle to
externalize the haptics of a 3-piece haptic IOL before using heat from a cautery to create a flanged haptic tip that permits intrascleral fixation without slippage.[12] He termed it the transconjunctival Intrascleral IOL fixation with the double-needle technique using flanged haptics. Its ease of performance and many advantages over the conventional SFIOL techniques make it the most attractive choice for both, anterior and posterior segment surgeons. However, the haptics of routinely used lenses like Tecnis ZA9003 [Abbott Medical Optics, Santa Ana, CA] and Sensar AR40e[Abbott Medical Optics, Santa Ana, CA] cannot be negotiated through routine 30 gauge needle.Since the thin walled 30 g needle is not freely available in our setting, we used 27 gauge needles to exteriorize the haptics of these IOLs. Even while using the 27g needle, we found that it took efforts to thread the trailing haptic into the needle lumen. In view of this, we recommend using a 26g needle for beginners so that the procedure is completed without haptic related complications such as breakage and slippage in the initial cases. We did not encounter any intraoperative complications related to the surgical technique.
We modified the Yamane technique where we exteriorized and fixed the leading haptic entirely before manipulating the lagging haptic, contrary to Yamane’s description of exteriorizing both haptics simultaneously because we believe that if the needle is made to hang inside after engaging the leading haptic then there is a probable risk of iris, ciliary body and retinal damage. IOP fluctuations, which are inevitable during insertion of the lagging haptic, enhance risk of intraocular tissue damage and disengagement. In our experience, though it is little difficult to manipulate the lagging haptic tip into the 27 g lumen once the leading haptic is outside the eye, we found that using an end gripping forceps and inserting the lagging haptic from the side port lead to successful completion of surgery without too much difficulty, one can use even a McPherson’s forceps through the main incision to introduce the lagging haptic tip into the 27 G lumen if scleral tunnel is used. The drawback of fixing the leading haptic first is that it becomes difficult to explant the IOL in toto if the trailing haptic gets damaged. However, we did not experience this in our series of 31 cases. If at all it happens, since anyway the trailing haptic is damaged we cant use the same lens so one has to cut the externalised haptic and remove the IOL. Complications were comparable to the previously described techniques of SFIOL (Table 1) except transient IOP elevation (39%) which was possibly due to retained viscoelastic following inadequate AC wash. We had a significant number of eyes with IOL explantation coupled with the SFIOL procedure, leading to significant astigmatism after surgery and reduced vision due to scarring induced by two back to back surgeries. Despite this, there was excellent visual recovery at the end of 6 weeks, which was maintained at 6 months. Similarly, we did not see any significant reduction in endothelial cell count and none of the eyes developed cystoid macular edema.
The main drawback of our study is the lack of a conventional control group. Future studies are required with larger sample, longer duration of follow up with a control group to understand the long term implications and stability of this surgical technique.
In conclusion, our initial experience spanning the intraoperative and six month postoperative course suggests that this technique of SFIOL fixation is relatively easy to perform, is independent of scleral flaps, tunnels, sutures and fibrin glue and has great potential in simplifying surgical correction of aphakia.
References:
- Shin Y, Shimpei S, Maiko MI, Kazuaki K. Flanged Intrascleral Intraocular Lens Fixation with Double-Needle Technique. Ophthalmology 2017;124(8):1136-4.
- Yamane S. Transconjunctival Intrascleral IOL Fixation with Double-Needle Technique. Available at https://ascrs2016.conferencefilms.com/acover.wcs?entryid=0082&bp=1, last accessed 9th September 2017.
- Dadeya S, Kamlesh, KumariSodhi P. Secondary intraocular lens implantation: anterior
chamber versus sclera fixation long term comparative evaluation. Eur J Ophthalmol 2003;13:627-33.
- Hoh H, Ruprecht K, Nikoloudakis N, Palmowski A. Preliminary results following
implantation of iris-suture fixated posterior chamber lenses. Ger J Ophthalmol 1993;2:70-75.
- Zhang ZD, Shen LJ, Liu XQ, Chen YQ, Qu J. Injection and suturing technique for scleral fixation foldable lens in the vitrectomized eye. Retina. 2010;30:353–6.
- Hoffman RS, Fine IH, Packer M, Rozenberg I. Scleral fixation using suture retrieval through a scleral tunnel. J Cataract Refract Surg. 2006;32:1259–63.
- Lin C-P, Han-Yi T. Suture fixation technique for posterior chamber intraocular lenses. J Cataract Refract Surg. 2004;30:1401–4.
- Gabor SG, Pavlidis MM. Suturelessintrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg 2007;33:1851–4.
- Mohr A, Hengerer F, Eckardt C. Retropupillary fixation of the iris claw lens in aphakia, 1 year outcome of a new implantation technique. Ophthalmology 2002; 99:580-3.
- Takayama K, Akimoto M, Taguchi H, Nakagawa S, Hiroi K. Transconjunctivalsuturelessintrascleral intraocular lens fixation using intrascleraltunnelsguided with catheter and 30-gauge needles. Br J Ophthalmol. 2015;99:1457-9.
- Scharioth GB, Prasad S, Georgalas I, Tataru C, Pavlidis M. Intermediate results of suturelessintrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg 2010;36:254–9.
- Sindal MD, NakhwaCP, SenguptaS. Comparison of sutured versus suturelessscleralfixatedintraocularlenses.J Cataract Refract Surg 2016;42:27–34.
- Agarwal A, Kumar DA, Jacob S, Baid C, Agarwal A, Srinivasan S. Fibrin glue assisted sutureless posterior chamber intraocular lens implantation in eyes with deficient posterior capsules. J Cataract Refractive Surg. 2008;34:1433-38.
- Kumar DA, Agarwal A, Prakash G, Jacob S, Saravanan Y, Agarwal A. Glued posterior chamber IOL in eyes with deficient capsular support: a retrospective analysis of 1-year post- operative outcomes. Eye 2010; 24:1143–1148
| Complication | Scharioth et al[11](Sutureless SFIOL, n=63) | Agarwal[14]?(Glued SFIOL, n=53) | Yamane[1](Flanged SFIOL. n=100) | Our study (Modified Yamane, n=31) |
| Temporary corneal edema | 5 (7.94%) | 1(1%) | Nil | |
| IOP elevation | 2 (3.17%) | 0 (0.0%) | 2 (2%) | 12(39%) |
| Hyphema | 2 (3.7%) | Nil | ||
| Hypotony | 1(1.59%) | 2(2%) | Nil |
Table 1 -Comparison of complication rates with other common techniques of sutureless SFIOL
| Pigment dispersion | 2 (3.7%) | |||
| Cystoid macular edema | 1(1.59%) | 4 (7.5%) | 1(1%) | Nil |
| Vitreous hemorrhage | 2(3.17%) | 0 (0.0%) | 5(8%) | 1(3.2%) |
| IOL Decentration | 3 (5.6%) | 2(6.4%) | ||
| Spontaneous IOL dislocation | 2(3.17%) | Nil | Nil | |
| Iris capture of IOL | 1(1.59%) | 8(8%) | Nil | |
| Spontaneous IOL dislocation | 1(1.59%) | Nil |
Figures :
Fig 1 – Flange of the externalized haptic
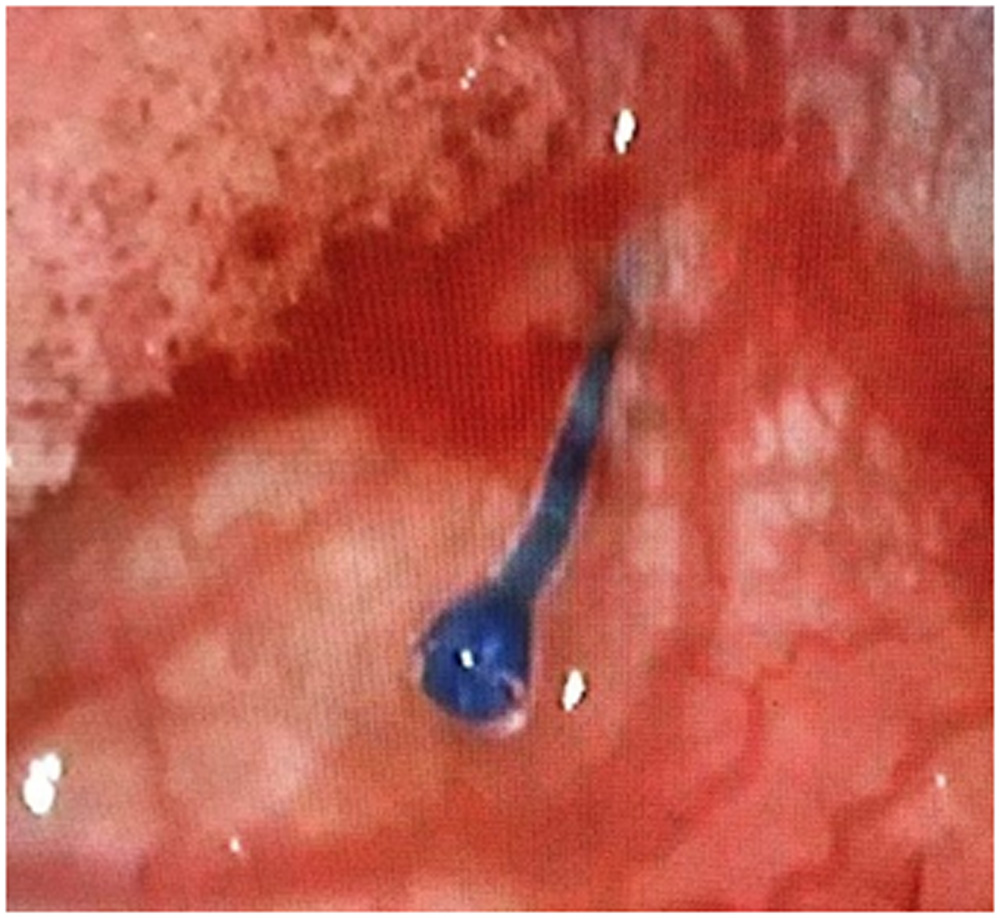
Fig 2 – Postoperative picture at 1 week
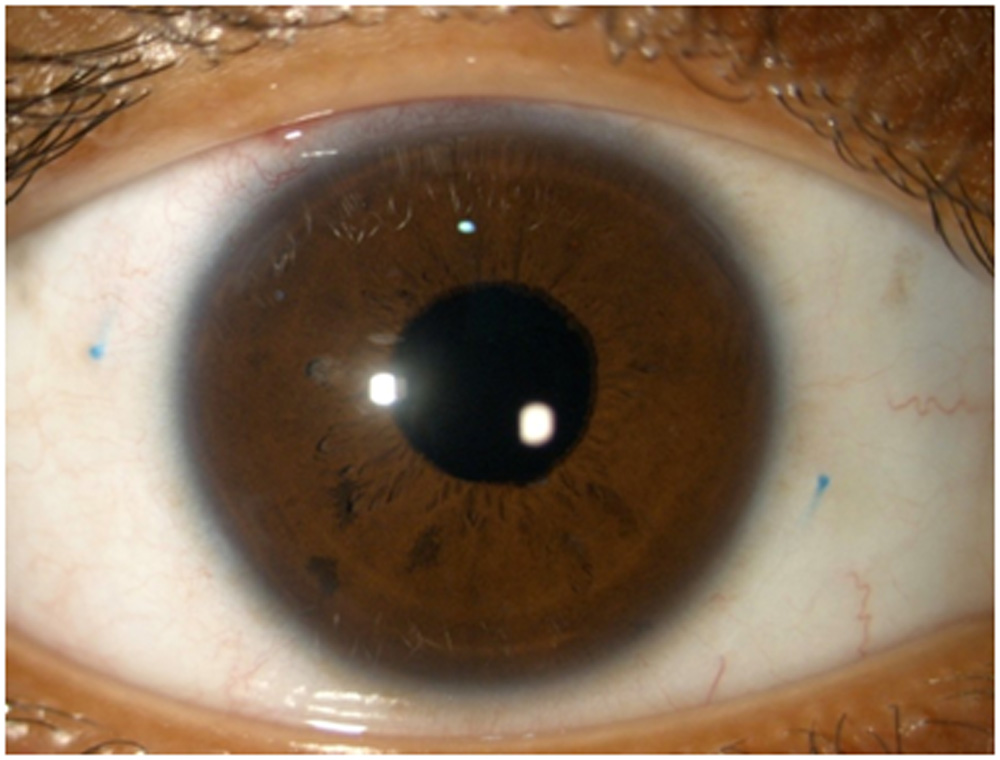
Fig 3 – Anterior Segment OCT demonstrating Intrascleral flange of the haptic
Leave a Comment