
Dr. Asmita Saha, A19654, Dr. Jonaki Roy, Dr. Subhankarsri Paul, Dr. Abhijit Chattopadhyay
Optical Coherence Tomography based Diagnosis of Polypoidal Choroidal Vasculopathy
Dr. Asmita Saha, Dr. Abhijit Chattopadhyay, Dr. Subhankarsri Paul, Dr. Jonaki Roy
Purpose: To evaluate the efficacy of an Optical Coherence Tomography based diagnosis of Polypoidal Choroidal Vasculopathy.
Methods: Retrospective observational study included 56 eyes of 56 patients (28 eyes with PCV & 28 eyes with typical exudative ARMD). Eyes with ≥3 of these OCT findings were diagnosed with PCV: multiple RPED, sharp RPED peak, RPED notch, hyporeflective lumen representing polyp, double layer sign, RPED with internal reflectivity, M-PED, sub-RPE hyperreflectivity. Eyes with a subfoveal choroidal thickness > 300 µm were associated with features of PCV despite having 2 OCT features. OCT-based diagnosis was compared with ICG-based method.
Result: In eyes with PCV, the above criteria was observed in 28 of 28 eyes with PCV (100%) & incidence of typical exudative ARMD was 8 of 28 eyes (28.6%). The sensitivity & specificity of the OCT-based diagnosis was 100% & 71.4% respectively.
Conclusion: The OCT-based diagnosis of PCV showed a high sensitivity & specificity. Increased choroidal thickness seen in cases of PCV.
Key-words: Optical coherence tomography, Polypoidal choroidal vasculopathy, Enhanced depth imaging, Age related macular disease, Retinal pigment epithelial detachment, Subfoveal choroidal thickness, Indocyanine green angiography
Introduction
Polypoidal choroidal vasculopathy (PCV) is a disorder characterized by a branching vascular network and polypoidal lesions on indocyanine green angiography (ICGA). It is becoming more frequently recognized as a cause of subretinal exudation and hemorrhage in the macula, which can result in significant damage to the macula and cause loss of vision. The prevalence of PCV is much higher in Asians than in whites and accounts for more than half of eyes diagnosed with neovascular age-related macular degeneration (nAMD).[1–4]
Photodynamic therapy, which is not a treatment employed in typical exudative AMD, is still considered a useful option in PCV; so differentiating them is important. ICGA is most important for diagnosis of PCV. At present, ICGA is essential in detecting characteristicchoroidal vascular changes including polypoidal vascular dilations and BVN; it has, therefore,become the gold standard in differentiating PCV from classic or occult CNV associated with typical nAMD.[14]However, ICGA is invasive, time consuming, and not widely available in many clinics. Spectraldomain optical coherence tomography (SD-OCT), which can capture high-resolution cross-sectional images of the posterior pole has proven valuable in detecting retinochoroidal morphologic changes.[12] Withmore comprehensive imaging modalities, it is possible to localize the lesions and to define their extent more precisely. Several studies have described OCT changes in eyes with PCV.[15–17]Sato et al18 described a double-layer sign(DLS), consisting of the retinal pigment epithelium (RPE) and another highly reflectivelayer underneath, which had been demonstrated as the most distinctive sign correlated with BVN by ICGA.[15–17]Saito et al16 showed that thumb-like polyps (TLPs), also called sharp pigment epitheliumdetachment (PED) peaks, which are observed as RPE protrusion under SD-OCT, corresponded to the“polypoidal lesions” imaged using ICGA. A TLP can be detected as a notch-like sign on the margin of thePED. [19] Recently, it has been suggested that TLPs represent not only the polyps themselves, but also the leakages from the polypoidal lesions.[20]A hyperreflective ring surrounding an area of hyporeflectivitylocated in the TLP probably represents the polypoidal lumen attached to the posterior surface of the RPE.The SD-OCT signs were defined according to the published literature.[12,15,16,19,23]Representative casesare shown in Figures 1, 2 and 3. Pigment epithelium detachment was determined as being present if singleor multiple dome-shaped detachment of the RPE was present. The DLS was defined as a flat gap with moderate reflection between the hyperreflective RPE band and the hyperreflective remainder of the Bruch’s membrane and inner choroid. In recent years, spectral domain optical coherence tomography (SD-OCT), including Enhanced Depth Imaging (EDI) OCT, has been used to investigate morphological alterations in eyes with PCV (Ojima et al. 2009; Ozawa et al. 2009; Freund et al. 2010; Chung et al. 2011; Koizumi et al.2011; Miura et al. 2011).
De Salvo et al.[20]suggested an optical coherence tomography (OCT)-based method to diagnose PCV. The OCT-based diagnosis was highly sensitive and specific.The purpose of the present study is to evaluate the efficacy of an OCT-based diagnosis of PCVwhere we attempted to improve this method by including a choroidal thickness criterion.
Materials & Methods
This retrospective, observational case series was performed at a single centre. 56 patients (28 eyes with active treatment-naïve PCV and 28 eyes with typical exudative ARMD) were included between November 2016 andApril 2017.
All patients were at least 50 year old (range: 53–75 years).The diagnosis of PCV was made based on ICGA findings of hyperfluorescent aneurysm-like lesions commonly known as polypoidal lesions, often in association with a BVN seen during thedye transit. The diagnosis of nAMD was determined based on FFA findings of neovascular lesions (including classic CNV, occult CNV, or both), with no polypoidal lesions or BVN shown on ICGA. Only those patients who underwentboth enhanced-depth imaging OCT [10] and ICGA examinations were included. Exclusion criteria were the presence of 1) other secondary choroidal neovascular diseases, such as angioid streaks, myopia, central serous chorioretinopathy, or presumed ocular histoplasmosis syndrome; 2) poor imaging of the RPE/choroid due to massive hemorrhage PED/subretinal hemorrhage, which masked the details of lesions; 3) cases of large cicatricial lesions; 4) a history of uveitis, diabetic retinopathy, proliferative retinopathy, or epiretinal macular membranes; 5) previous retinal surgery or intraocular injection; 6) poor image quality because of unstable fixation or severe cataract; and 7) anyassociated systematic disorders that might affect the eyes (e.g., systemic corticosteroid use, uncontrolled diabetes, or hypertension).Eyes with a subretinal hemorrhage greater than five disc areas in size were also excluded because large hemorrhages may interfere with accurate OCT-based classification. When exudative AMD and PCV were diagnosed in both eyes, the eye that had been affected first was used.
All patients underwent a comprehensive ocular examination, including visual acuity, fundus examination,color fundus photography, FFA, and ICGA using Spectralis equipment (Heidelberg Engineering,Heidelberg, Germany) Spectral domain-OCT was performed in each patient after fundus examination and fundus photography capture. Horizontal and vertical OCT scans (Spectralis; Heidelberg Engineering, Heidelberg, Germany) aligned at the central fovea were performed. Enhanced-depth imaging OCT driven by Spectralis software (Heidelberg Engineering) was performed using horizontal and vertical scans aligned at the central fovea. Fluorescein angiography and ICGA were also performed.
In this study, the OCT-based diagnosis of PCV was based on the presence of >=3 of the following findings: multiple RPED, sharp RPED peak, RPED notch, hyporeflective lumen representing polyp,double layer sign , RPED with internal reflectivity, M-PED , sub –RPE hyperreflectivity.Eyes with a subfoveal choroidal thickness >300 µm were associated with features of PCV despite having 2 OCT features.OCT based diagnosis was compared with ICGA based method.
A single examiner who was blinded to the angiography images and other patient information, performed the OCT-based diagnosis (Heidelberg Engineering). All the OCT imageswere reviewed.In the present study, the ICGA-based classification was considered to be the gold-standard method. PCV was diagnosed based on the presence of branching vascular networks and polypoidal lesions. Other cases were classified as typical exudative AMD. The subfoveal choroidal thickness was additionally measured using enhanced-depth imaging OCT images and was defined as the distance from the hyperreflective line of the subfoveal RPE-Bruch’s membrane complex to the innermost hyperreflective line of the subfoveal chorio-scleral interface.
The incidence of each OCT feature in cases of both PCV and typical exudative AMD was compared. The results of the OCT-based diagnosis were compared with those of theICGA-based analysis.The sensitivity and specificity of the OCT based diagnosis was analysed.
tatistical Analysis
Data were analysed using a commercial analytical software program (SPSS16.0; IBM Inc, New York,NY). Differences in age at diagnosis, gender, and SDOCT sign distribution between PCV and typicalnAMD were compared using theindependent t-test and the Chi-square test with Bonferroni’s correction. Diagnostic sensitivity, and specificity werecalculatedin each differential diagnosis strategy.
Results
A total 56 eyes in 56 patients satisfied the eligibility criteria (Table 1). Of these, 35 (62.5%) were men, and 21 (37.5%) were women. The mean age ± standard deviation was 65.8 ± 7.3 years. Based on the ICGA findings, typical exudative AMD and PCV were diagnosed in 28 eyes (50%) and 28 eyes (50%), respectively.The incidences of each OCT feature in typical exudative AMD and PCV are summarized in Table 1. In eyes with PCV, multiple RPED, sharp RPED peak, RPED notch, hyporeflective lumen representing polyp, double layer sign, RPED with internal reflectivity, M-PED and sub-RPE hyperreflectivity were observed in 20 eyes (71.4%), 10 eyes (35.7%), 12 eyes (42.9%), 8 eyes (28.6%), 12 eyes (42.9%), 18 eyes (64.3%), 10 eyes (35.7%) and 12 eyes (42.9%) respectively. In eyes with typical exudative AMD, these lesions were identified in 6 eyes (21.4%), 2 eyes (7.1%), 0 eyes (0%), 0 eyes (0%), 4 eyes (14.3%), 8 eyes (28.6%), 0 eyes (0%) and 0 eyes (0%) respectively. The incidences of all five findings were significantly higher in eyes with PCV than in those with typical exudative AMD (Table 1).Figures 1, 2 and 3 show representative cases of PCV with various OCT features.
Table 1. Incidence and number of OCT features in the included patients
| OCT Features | PCV
(n=28) |
Typical Exudative AMD (n=28) | p-value* |
| Multiple RPED | 20 eyes (71.4%) | 6 eyes (21.4%) | <0.001 |
| Sharp RPED Peak | 10 eyes (35.7%) | 2 eyes (7.1%) | <0.001 |
| RPED Notch | 12 eyes (42.9%) | 0 eyes (0%) | <0.001 |
| Hyporeflective Lumen representing Polyp | 8 eyes (28.6%) | 0 eyes (0%) | <0.001 |
| Double Layer Sign | 12 eyes (42.9%) | 4 eyes (14.3%) | <0.001 |
| RPED with internal reflectivity | 18 eyes (64.3%) | 8 eyes (28.6%) | <0.001 |
| M-PED | 10 eyes (35.7%) | 0 eyes (0%) | <0.001 |
| Sub-RPE hyperreflectivity | 12 eyes (42.9%) | 0 eyes (0%) | <0.001 |
*Chi-square test with Bonferroni’s correction
Among the 28 ICGA-confirmed PCVs, three or more OCT features were noted in 20 eyes (71.4%), whereas three or more OCT features were identified in 2 (7.1%) of 28 ICGA-confirmed typical exudative AMDs. Additionally, among the 28 ICGA-confirmed PCVs, two OCT features with subfoveal choroidal thickness > 300 µm were noted in 8 eyes (28.6%).The distribution of OCT features in PCV and typical exudative AMD are summarized in Tables 2 and 3. The sensitivity and specificity of the OCT-based PCV diagnosis were 100% and 71.4% respectively.
Table 2.Distribution of OCT features in PCV and typical exudative AMD
| No. of OCT Features present | PCV
(n=28) |
Typical Exudative AMD (n=28) |
| 1 | 0 | 2 eyes (7.1%) |
| 2 | 8 eyes (28.6%) | 6 eyes (21.4%) |
| 2 with subfoveal choroidal thickness > 300 µm | 8 eyes (28.6%) | 2 eyes (7.1%) |
| 3 or more | 20 eyes (71.4%) | 6 eyes (21.4%) |
Table 3.Sensitivity and specificity of the OCT-based PCV diagnosis
| True Positive (TP) | True Negative (TP) | False Negative (FN) | False Positive (FP) |
| 28 | 20 | 0 | 8 |
| Sensitivity
[TP/(TP+FN)] |
100% [28/(28+0)] | Specificity
[TN/(TN+FP)] |
71.4 % [20/(20+8)] |
Figure 1: Features of PCV on SDOCT:Dome shaped PED,Sub RPE cavities (Hyporeflective Lumen representing Polyp),Bumpy and M- shaped PED.Indocyanine green angiography (ICGA) shows a well-defined branch vascular network with polypoidal lesions onthe margin. In the horizontal SD-OCT scan at the level of polyp, the RPE layer shows a protruding shape in the parafovea, which is correlated with the location of polypoidallesions on ICGA.
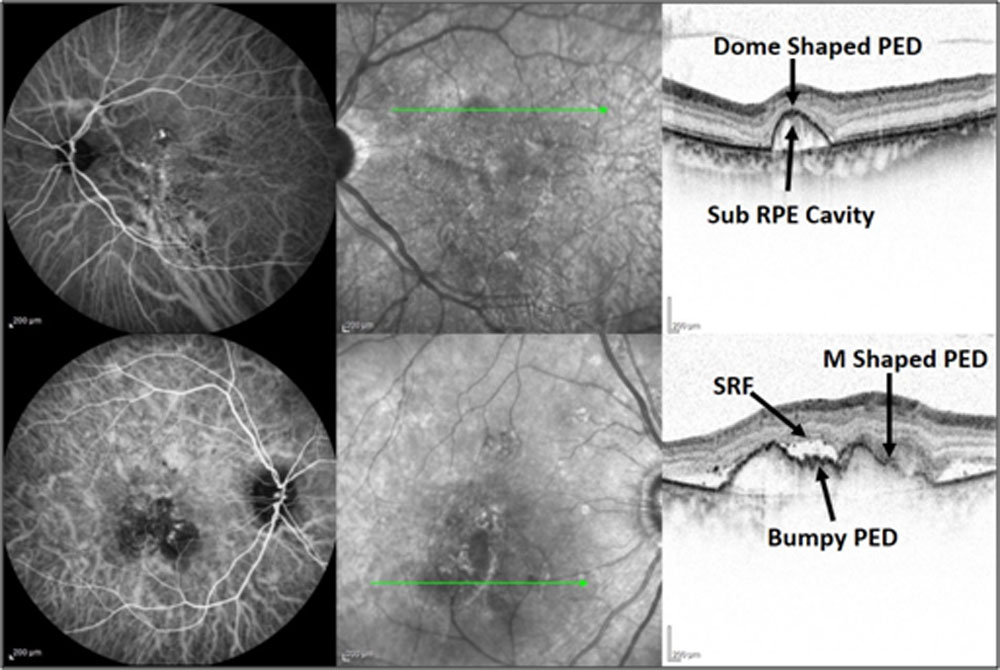
Figure 2: M- shaped PED with internal reflectivity, Sub-RPE Cavities (Hyporeflective Lumen representing Polyp), Double Layer Sign(DLS) and Sub-RPE Hyper-reflectivity. A DLS consisting of a hyperreflective detached flatterRPE and Bruch’s membrane underneath is observed in the macular area. On vertical scanning, the DLS was corresponding to the branch vascular network in ICGA. (Polyp with BVN encircled)
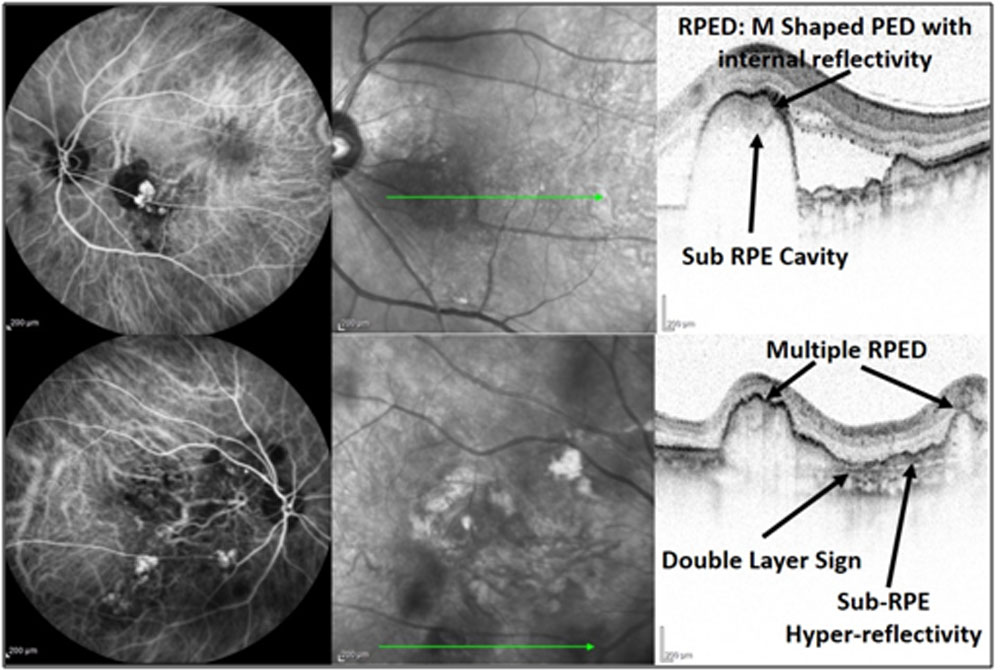
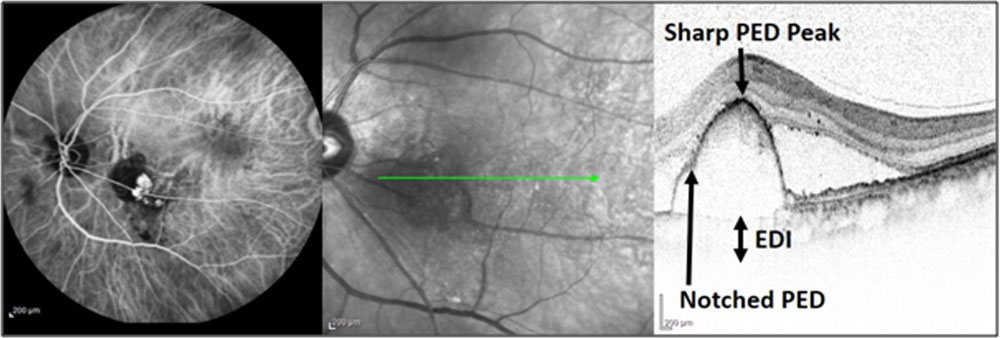
Figure 3: Features of PCV on SDOCT:Notched PED, Sharp PED peak and Enhanced Depth Imaging (EDI). Polypoidallesions at the edge of PED areclearly demonstrated in ICGA. PED was located in theparafovea. Double layer sign is also evident.(Polyp with BVN encircled)
Discussion
In the present study, the OCT-based diagnosis of PCV with the addition of choroidal thickness as a criterion showed a higher sensitivity as compared to the criterion proposed by De Salvo et al. [20]. However this study has relatively lower specificity.In the present study, the OCT-based diagnosis was performed for patients regardless of the presence of visible RPED, whereas the efficacy of the method was originally determined in patients with at least one RPED [20]. The results of this study, in combination with those of the previous study [20], advocate that the OCT-based diagnosis of PCV is a useful method in clinical practice.
In the study by De Salvo et al. [20], an OCT-based analysis was undertaken for eyes with one or more incidences of pigment epithelial detachment; classic exudative AMD were excluded. However, in our study we incorporated all the patients, irrespective of their fundus and fluorescein angiography findings, for the mentioned reasons. Firstly, as previously described by De Salvo et al. [20], the OCT-based method can be useful for patients allergic to fluorescein dye. Therefore, by using the OCT-based method in such patients, PCV can be diagnosed without fluorescein angiography findings. Secondly, small serous RPEDs are at times hard to identify precisely by fundus photographs, even though they are easily identifiable by stereoscopic fundus examination.To perform a subgroup analysis in clinical studies without ICGA, fundus findings may be interpreted mainly using fundus photographs. Thus, it is our belief that a PCV diagnosis using OCT has some advantages over the earlier suggested methods, in spite of using only a single imaging modality, which may lose some sensitivity and specificity. The primary advantage of an OCT-based diagnosis of PCV is that it helps clinicians determine treatment strategy in the absence of ICGA results. According to us, another important benefit of an OCT-based method is that the treatment outcomes in PCV patients in large clinical trials cannot be crudely estimated without ICGA results. It is important to diagnosePCV to establish an appropriate treatment plan. However, the OCT-based diagnosis of PCV has some limitations when compared with the gold-standard ICGA-based method. However, according to us, using the OCT-based method to subgroup analyses in future large clinical trials can provide definite benefits because the result will thus be generated from high quality data. The evaluations in the present study can provide a good reference in future studies.
Since it is known that eyes with PCV usually exhibit a thicker choroid than that observed in typical exudative AMD [19, 20]. In the study by De Salvo et al. [20], however, the choroidal thickness was not used as a criterion to diagnose PCV. In the present study, we incorporated a choroidal thickness criterion as an additional criterion to improve the sensitivity of OCT-based diagnoses.
To identify whether an OCT-based diagnosis is beneficial for subgroup analysis in clinical studies, we compared the short-term treatment outcomes of PCV between cases that were classified based on ICGA and those classified using OCT. The findings showed that the treatmentoutcomes were comparable, irrespective of the method used for the diagnosis. This result suggests potential utility of OCT-based classification for subgroup analysis in future clinical studies, without the requirement for ICGA.
We hope that further additional studies may establish more accurate criteria for the OCT-based diagnosis of PCV. More complex diagnosis methods may not be appropriate for use in clinical practice. However, we believe that even a complicated approachthat requires significant time and effort to classify PCV can be used for the subgroup analysis in clinical studies.
To summarise, the OCT-based diagnosis of PCV withthe addition of the choroidal thickness criterion improved the sensitivity of the method. This OCTbased method may help clinicians develop appropriate treatment strategies for patients for whom ICGA results are not available. Moreover, we believe that this method may be useful in the subgroup analysis of data in large clinical trials that lack an ICGA examination. To establish more accurate and robust criteria for the OCT based diagnosis of PCV further discussionsand additional studies will be required.
Acknowledgements
This study was supported by Priyamvada Birla Aravind Eye Hospital, Kolkata (India).
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflict of interest.
References
- Yannuzzi LA, Wong DW, Sforzolini BS, et al. Polypoidal choroidal vasculopathy and neovascularized age-related macular degeneration. Arch Ophthalmol 1999;117:1503–1510.
- Ciardella AP, Donsoff IM, Huang SJ, et al. Polypoidal choroidalvasculopathy. Surv Ophthalmol 2004;49:25–37.
- Liu Y, Wen F, Huang S, et al. Subtype lesions of neovascularage-related macular degeneration in Chinese patients. GraefesArch Clin Exp Ophthalmol 2007;245:1441–1445.
- Maruko I, Iida T, Saito M, et al. Clinical characteristics ofexudative age-related macular degeneration in Japanese patients.Am J Ophthalmol 2007;144:15–22.
- Kuroiwa S, Tateiwa H, Hisatomi T, et al. Pathological featuresof surgically excised polypoidal choroidal vasculopathy membranes.Clin Exp Ophthalmol 2004;32:297–302.
- Nakashizuka H, Mitsumata M, Okisaka S, et al. Clinicopathologicfindings in polypoidal choroidal vasculopathy. InvestOphthalmol Vis Sci 2008;49:4729–4737.
- Yoshida Y, Kohno T, Yamamoto M, et al. Two-year results ofreduced-fluence photodynamic therapy combined with intravitrealranibizumab for typical age-related macular degenerationand polypoidal choroidal vasculopathy. Jpn J Ophthalmol2013;57:283–293.
- Hata M, Tsujikawa A, Miyake M, et al. Two-year visual outcomeof ranibizumab in typical neovascular age-related maculardegeneration and polypoidal choroidal vasculopathy.Graefes Arch Clin Exp Ophthalmol 2014;253:221–227.
- Lima LH, Schubert C, Ferrara DC, et al. Three major lociinvolved in age-related macular degeneration are also associatedwith polypoidal choroidal vasculopathy. Ophthalmology2010;117:1567–1570.
- Nakata I, Yamashiro K, Yamada R, et al. Significance of C2/CFB variants in age-related macular degeneration and polypoidalchoroidal vasculopathy in a Japanese population. InvestOphthalmol Vis Sci 2012;53:794–798.
- Lafaut BA, Leys AM, Snyers B, et al. Polypoidal choroidalvasculopathy in Caucasians. Graefes Arch Clin Exp Ophthalmol2000;238:752–759.
- Ozawa S, Ishikawa K, Ito Y, et al. Differences in macularmorphology between polypoidal choroidal vasculopathy andexudative age-related macular degeneration detected by opticalcoherence tomography. Retina 2009;29:793–802.
- Uyama M, Wada M, Nagai Y, et al. Polypoidal choroidalvasculopathy: natural history. Am J Ophthalmol 2002;133:639–648.
- Criteria for diagnosis of polypoidal choroidal vasculopathy [inJapanese]. Nihon Ganka Gakkai Zasshi 2005;109:417–427.
- Abe S, Yamamoto T, Haneda S, et al. Three-dimensional featuresof polypoidal choroidal vasculopathy observed byspectral-domain OCT. Ophthalmic Surg Lasers Imaging2010:1–6.
- Saito M, Iida T, Nagayama D. Cross-sectional and en faceoptical coherencetomographic features of polypoidal choroidalvasculopathy. Retina 2008;28:459–464.
- Yang LH, Jonas JB, Wei WB. Optical coherence tomographicenhanced depth imaging of polypoidal choroidal vasculopathy.Retina 2013;33:1584–1589.
- Sato T, Kishi S, Watanabe G, et al. Tomographic features ofbranching vascular networks in polypoidal choroidal vasculopathy.Retina 2007;27:589–594.
- Ojima Y, Hangai M, Sakamoto A, et al. Improved visualizationof polypoidal choroidal vasculopathy lesions using spectraldomainoptical coherence tomography. Retina 2009;29:52–59.
- De Salvo G, Vaz-Pereira S, Keane PA, et al. Sensitivity andspecificity of spectral-domain optical coherence tomography indetecting idiopathic polypoidal choroidal vasculopathy. Am JOphthalmol 2014;158:1228–1238 e1221.
- Khan S, Engelbert M, Imamura Y, Freund KB. Polypoidalchoroidal vasculopathy: simultaneous indocyanine green angiographyand eye-tracked spectral domain optical coherencetomography findings. Retina 2012;32:1057–1068.
- Iida T. Polypoidal choroidal vasculopathy with an appearancesimilar to classic choroidal neovascularisation on fluoresceinangiography. Br J Ophthalmol 2007;91:1103–1104.
- Iijima H, Iida T, Imai M, et al. Optical coherence tomographyof orange-red subretinal lesions in eyes with idiopathic polypoidalchoroidal vasculopathy. Am J Ophthalmol 2000;129:21–26.
- Cheung CM, Lai TY, Chen SJ, et al. Understanding indocyaninegreen angiography in polypoidal choroidal vasculopathy:the group experience with digital fundus photography and confocalscanning laser ophthalmoscopy. Retina 2014;34:2397–2406.
- Yannuzzi LA, Sorenson J, Spaide RF, Lipson B. Idiopathic polypoidal choroidal vasculopathy (IPCV). Retina 1990; 10:1-8.
- Spaide RF, Yannuzzi LA, Slakter JS, et al. Indocyanine green videoangiography of idiopathic polypoidal choroidal vasculopathy. Retina 1995;15:100-10.
- Koh AH, Chen LJ, Chen SJ, et al. Polypoidal choroidal vasculopathy: evidence-based guidelines for clinical diagnosis and treatment. Retina 2013;33:686-716.
- Coscas G, Yamashiro K, Coscas F, et al. Comparison of exudative age-related macular degeneration subtypes in Japanese and French Patients: multicenter diagnosis with multimodal imaging. Am J Ophthalmol 2014;158:309-18.e2.
- Imamura Y, Engelbert M, Iida T, et al. Polypoidal choroidal vasculopathy: a review. Surv Ophthalmol 2010;55:501-15.
- Spaide RF, Koizumi H, Pozzoni MC. Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol 2008;146:496-500.
- Koh A, Lee WK, Chen LJ, et al. EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina 2012;32:1453-64.
- Cho M, Barbazetto IA, Freund KB. Refractory neovascular age-related macular degeneration secondary to polypoidal choroidal vasculopathy. Am J Ophthalmol 2009;148:70-8.e1.
- Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med 2006;355:1432-44.
- Kim SW, Oh J, Kwon SS, et al. Comparison of choroidal thickness among patients with healthy eyes, early age-related maculopathy, neovascular age-related macular degeneration, central serous chorioretinopathy, and polypoidal choroidal vasculopathy. Retina 2011;31:1904-11.
- Koizumi H, Yamagishi T, Yamazaki T, et al. Subfoveal choroidal thickness in typical age-related macular degeneration and polypoidal choroidal vasculopathy. Graefes Arch Clin Exp Ophthalmol 2011;249:1123-8.
- Kawamura A, Yuzawa M, Mori R, et al. Indocyanine green angiographic and optical coherence tomographic findings support classification of polypoidal choroidal vasculopathy into two types. Acta Ophthalmol 2013;91:e474-81.
- Koizumi H, Yamagishi T, Yamazaki T, Kinoshita S. Relationship between clinical characteristics of polypoidal choroidal vasculopathy and choroidal vascular hyperpermeability. Am J Ophthalmol 2013;155:305-13.e1
Leave a Comment