
Dr. Maneesh Bapaye, B12628
Introduction
Dissection of vascularized fibrovascular membranes in a diabetic tractional or combined retinal detachment is one of most challenging situations faced by a vitreoretinal surgeon. A key to achieving successful membrane dissection is achieving a correct plane of dissection between viable retina and vascular membrane. With small gauge transconjunctival vitrectomy systems most of the membrane peeling is achieved by vitreous cutters. Even then in presence of flat fibrovascular proliferation it may be difficult to achieve a dissection plane to insert the cutter port. We have designed a instrument which is used to achieve dissection plane in such tricky case scenarios and believe will add significant value to the diabetic vitreous surgery
Description
The titanium instrument has a handle and a narrow shaft. Length of the shaft from tip to handle is 32mm (Fig.1). At the tip the shaft is bent at almost 45 degrees and has a blunt round tip and sharpened edges. The tip measures 0.6mm. Diameter of the shaft is 0.5mm (Fig.2). It can be introduced through 23 gauge cannulae of transconjunctival vitrectomy systems. Handle measures around 95-100mm and has serrations for firm grip. The tip enters between the ERM and the retina & the sharpened edge create clean dissection plane between the major vascular nails without pulling onto the tissues. A vitrectomy cutter can then be used to achieve segmentation of membranes.
Results:
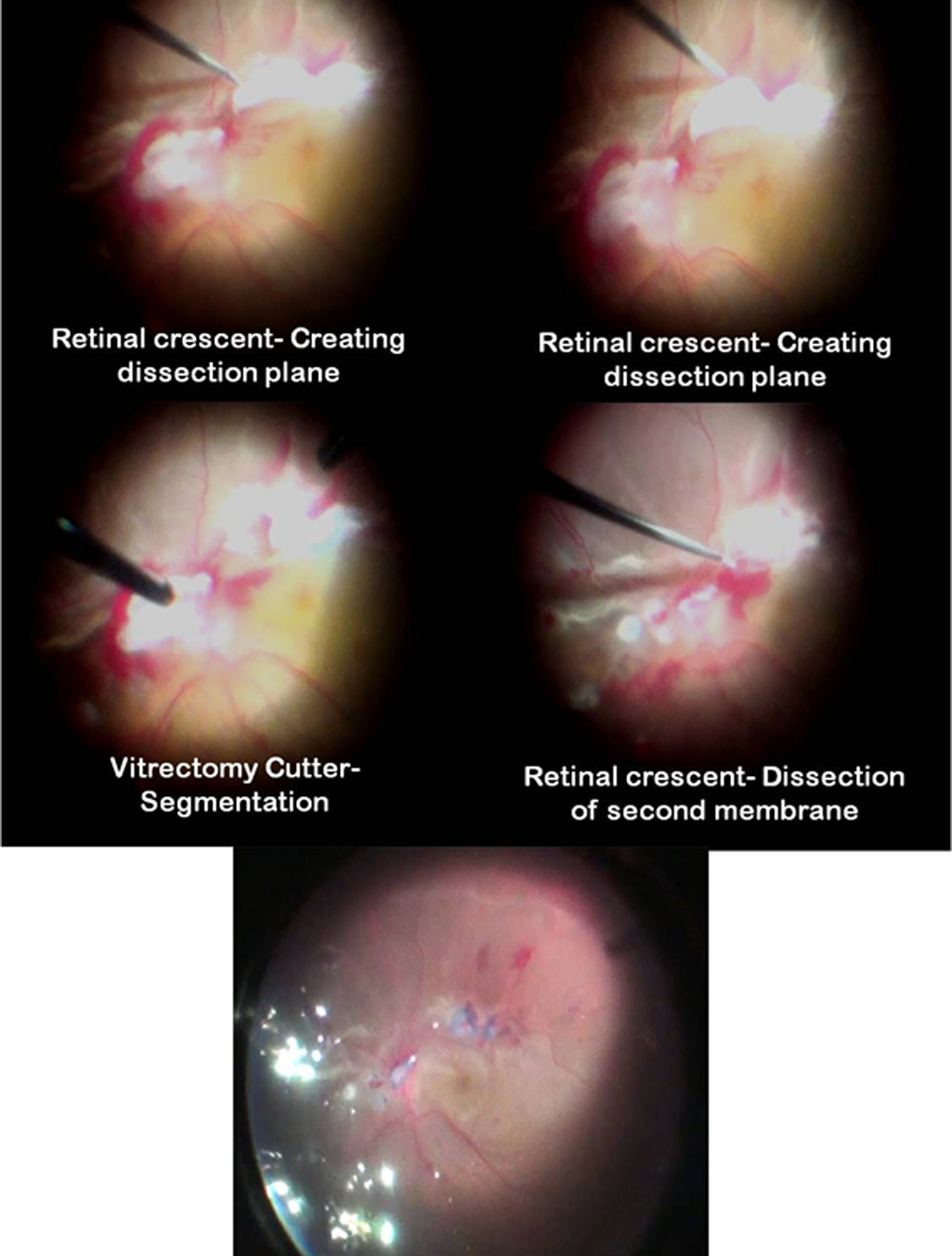
The Retinal Crescent has been used only a 4-5 cases. In most of the cases fibrovascular membrane dissection was achieved membrane dissection was completed without causing or with a very few iatrogenic retinal breaks. Clean dissection plane could be achieved in crucial situations like flat fibrovascular membranes, dense fibrovascular membranes in setting of combined retinal detachment, fibrovascular membranes close to macula and in peripapillary region. Fig.3 depicts intraoperative pictures of fibrovascular membrane dissection where the crescent was used.
Discussion
Vitrectomy for proliferative diabetic retinopathy involves debulking of central vitreous, creating an opening in posterior vitreous cortex (PVC) in area where posterior vitreous detachment is present, truncating the cone of PVC 360 degrees to the edge of vascularized epiretinal membranes. These membranes are then segmented into smaller islands before delaminating from vascular apices1. Segmentation can be done using curved scissors or cutter tip of small gauge vitrectomy system. In absence of or presence of shallow PVD, inside-out delamination of ERM starting near optic disk and progressing along vascular arcades. It is considered safer to segment the ERM into smaller segments between points of vascular adhesions before delaminating rather than attempting to remove these en-bloc. Scissors or vitreous cutters are used to segment and then delaminating the membranes. Successful segmentation without creating retinal break can be achieved by finding correct plane between retina and ERM which is frequently tightly adherent to it. Chances of creating iatrogenic retinal break are significant in case correct plane of dissection is not achieved. The risk is higher in cases of combined tractional and rhegmatogenous detachment as retina is redundant and mobile. Membrane pics frequently used for management of PVR membranes can’t be used in fibrovascular membranes as they can pull the retina and create iatrogenic breaks. Other methods of membrane dissection in diabetic patients are en-bloc dissection and bimanual dissection methods. In case of en-bloc dissection, uncut PVC cone is used to apply traction on ERM edge and delaminating. Chances of iatrogenic breaks are higher in other areas of tight vitreoretinal adhesions while surgeon is concentrating on ERM removal. In case of bimanual dissection, end gripping forceps is used to lift edge of ERM while vitrectomy cutter tip or curved scissors are used to cut the vascular apices. Chandelier light source or assistant holding light pipe is used for endoillumination. While bimanual technique is safer than en-bloc dissection improper position of light source as well as diffuse rather than focused light may become an issue in proper visualization of operative field. Application of excessive traction on membrane edge held by forceps in non-dominant hand can potentially lead to iatrogenic retinal break. The retinal crescent helps in creating appropriate plane for segmentation of membranes. The sharpened edges of the instrument can shear flimsy adhesions without creating traction on underlying retina, minimizing chances of iatrogenic break. It helps in reducing number of iatrogenic breaks and enhancing speed of membrane dissection by creating appropriate dissection plane. Sometimes retinal membrane peeling forceps are also used to create such plane but they can inadvertently avulse vascular nails causing significant bleeding or creating iatrogenic breaks in fragile retina. This problem is taken care of with the retinal crescent as it doesn’t cause any pull on retinal tissues.This instrument is meant to act as accessory rather than replacement for scissors or vitreous cutter in management of vascularized membranes.
Conclusion:
The Retinal Crescent creates correct dissection plane setting of vascularized membranes without causing retinal traction thereby achieving faster, cleaner membrane dissection with less chances of iatrogenic retinal break formation.
References
1.Vitreous Microsurgery (5th Edition): Charles S, Calzada J & Wood B. Chapter 19. Diabetic Retinopathy
Legends
Fig.1a: Retinal crescent
Fig1b: Shaft of retinal crescent
Fig2a: Tip of retinal crescent
Fig2b: Measurement of the tip
Fig.2c: Angle of the tip
Fig.3: Intraoperative picture composite of retinal crescent used for fibrovascular membrane dissection
Figure1:
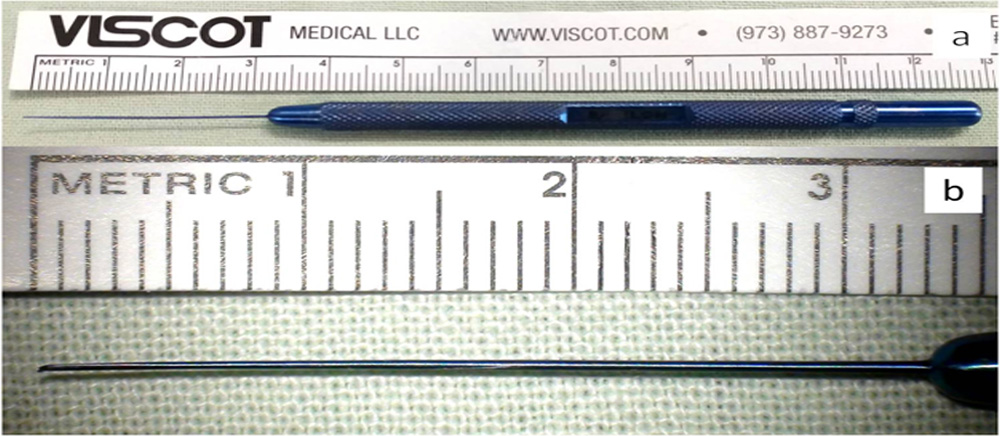
Figure 2
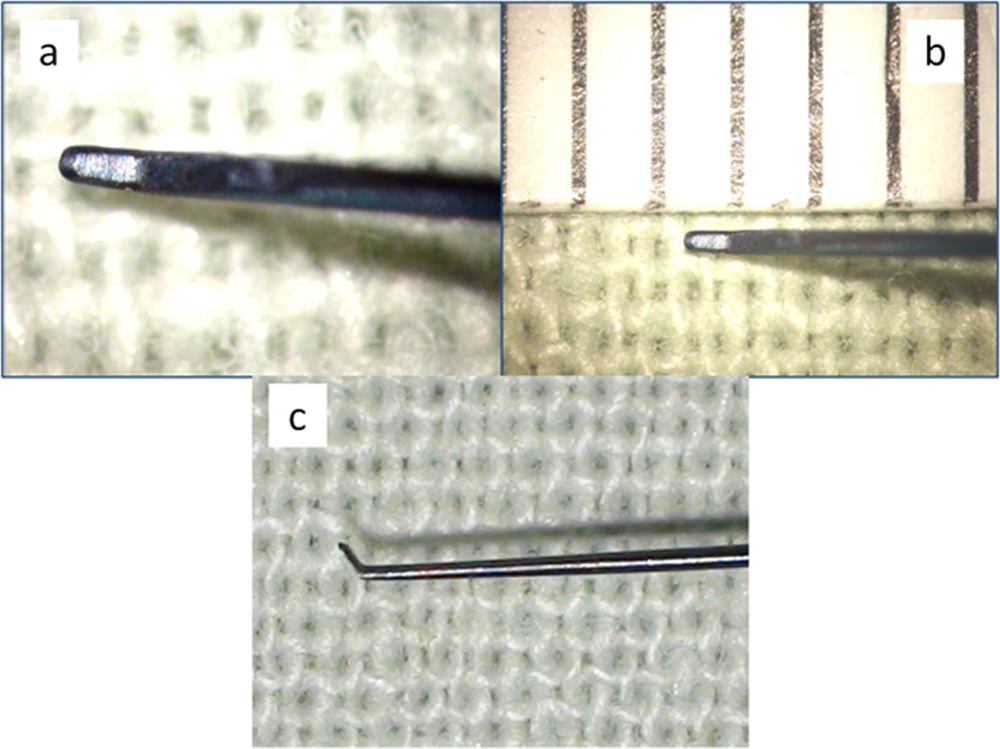
Figure 3
Leave a Comment