
Dr. Narayan Bardoloi, N03755, Dr. Rajvin Samuel Ponraj, Dr. Mayur Dutta Bharali, Dr. Sagarika Das
INTRODUCTION
Modern phacoemulsification cataract surgery claims to provide earliest rehabilitation to a patient. It is a walk in walk out procedure. Patient can resume normal activities from the very day of surgery. In spite of these advantages a patient has to put eye drop into the operated eye from time to time for a period of four to six weeks. That takes away a lot of sheen out of this very beautiful procedure 1, 2. Here arises the problem of compliance, injury to corneal epithelial surface, high cost and frequent callbacks. A compliance monitoring study found that cataract surgery patients did not comply with the prescribed number of postoperative drops3. Some use improper technique during application of postoperative drops 4 . Examples of improper techniques include the drop missing the eye, instilling an incorrect number of drops in one dose, and contaminating the bottle tip4. The same study also reported that less than half of the patients waited less than 5 minutes between instilling different eye-drop medications.4 Noncompliance with ophthalmic topical drops has been reported to be as high as 40%.5
In another study, it has been found that 40% of the patients coming for phacoemulsification surgery suffer from dry eye disease of some form. Postoperative eye drop will add insult to the already compromised corneal surface.
High cost of postoperative medication adds to the causes of non-compliance in countries like India, Nepal, Pakistan and Bangladesh where half of the population live below the poverty line. How many drops, how many times, in which eye are frequent callbacks an ophthalmologist encounters during postoperative period.
Dropless cataract surgery is a new technique practiced by many American cataract surgeons for the last couple of years. A specially prepared compound called Trimoxi containing Triamcinolone acetonide and Moxifloxacin(TM) and Trimoxivanc(TMV) where Vancomycin is added is available in American market. After IOL implantation, the surgeons inject this mixture transzonularly into the vitreous cavity. This eliminates the need for instillation of eye drop postoperatively and patients can lead a life free from any compulsion. There has been many reports of surgeons resorting to this technique with very good effect and without any major complication. This study is an endeavor to do this technique in India for the first time. Since commercially available mixing compounds of TM is not available in India, we have mixed these two compounds on the operation table from fresh bottles of Moxifloxacin eyedrop and fresh ampoule of Triamcinolone acetonide (TA).
AIM
To evaluate the clinical outcome following intraoperative transzonular intravitreal injection of Triamcinolone- Moxifloxacin(TM) in patients undergoing phacoemulsification cataract extraction with IOL implantation.
SETTING
Chandra Prabha Eye Hospital, Jorhat, Assam, India.
STUDY PERIOD
February 2017- May 2017
INCLUSION CRITERIA
Patients who came for cataract surgery were informed about dropless cataract surgery along with its pros and cons. Those who voluntarily gave consent for the procedure were included in the study.
EXCLUSION CRITERIA
Patients who have glaucoma or are known steroid responders.
METHODS
A prospective, non randomized, non comparative clinical interventional study. The study protocol was approved by institutional ethics committee (IEC) of Chandraprabha Eye Hospital and abides by the tenets of the declaration of Helsinki. Informed consent was obtained from all participants.
All surgeries were done by a single surgeon. Under topical anesthesia, 2.2mm limbal temporal incision given. Phacoemulsification done with chopping technique in active fluidic system. After IOL insertion into the bag, the AC is filled with cohesive OVD. A mixture of 0.1ml each of TM was injected into the anterior vitreous transzonularly with a 27 gauze bent cannula. Plume of visible Triamcinolone suspension with antibiotic was seen within the vitreous. There is usual rise of IOP with shallowing of the AC and sometimes prolapse of iris. Bimanual irrigation and aspiration is done to remove the OVD and reform the AC. No patch is given and patient is allowed to go home after checkup of vital parameters. Follow up was done at Day 1, 7, 30, 60. On each visit, visual acuity, intraocular pressure (IOP), cells and flares were measured. Subjects were also asked to evaluate pain perception and overall satisfaction with surgery.
RESULTS
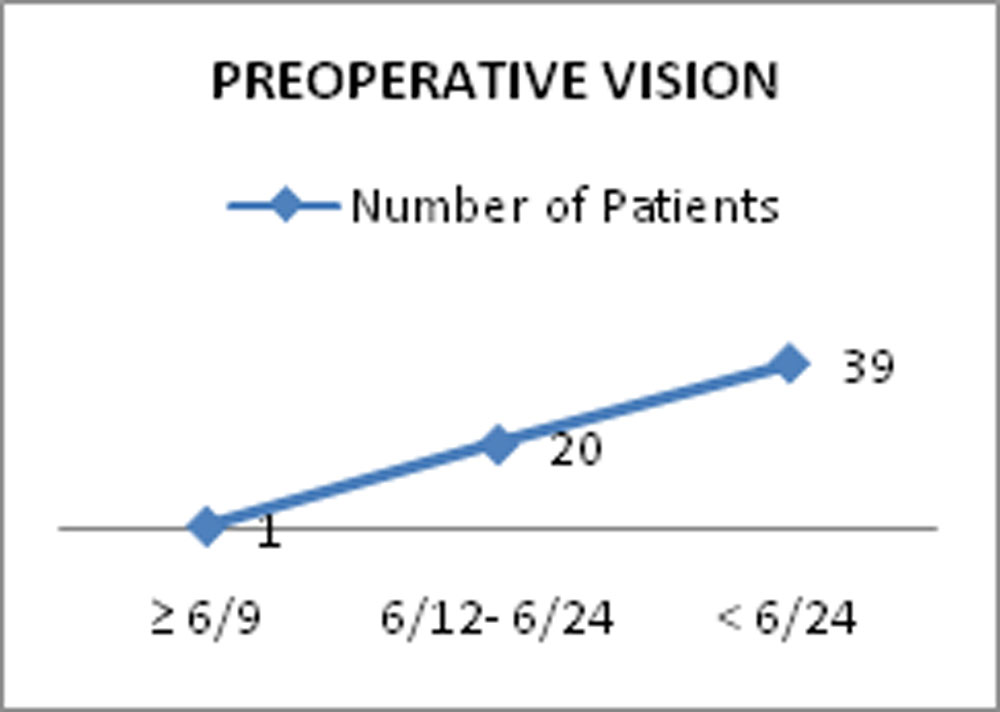
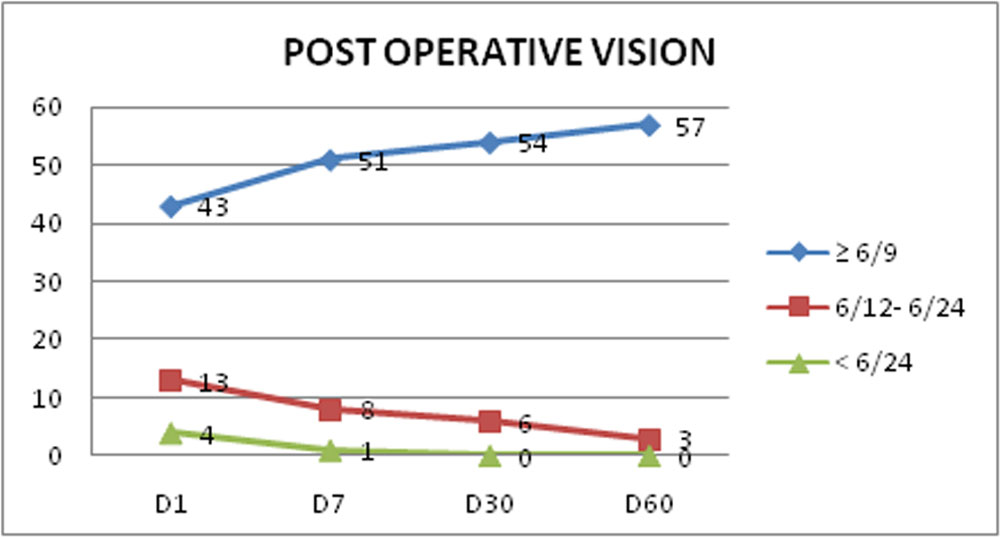
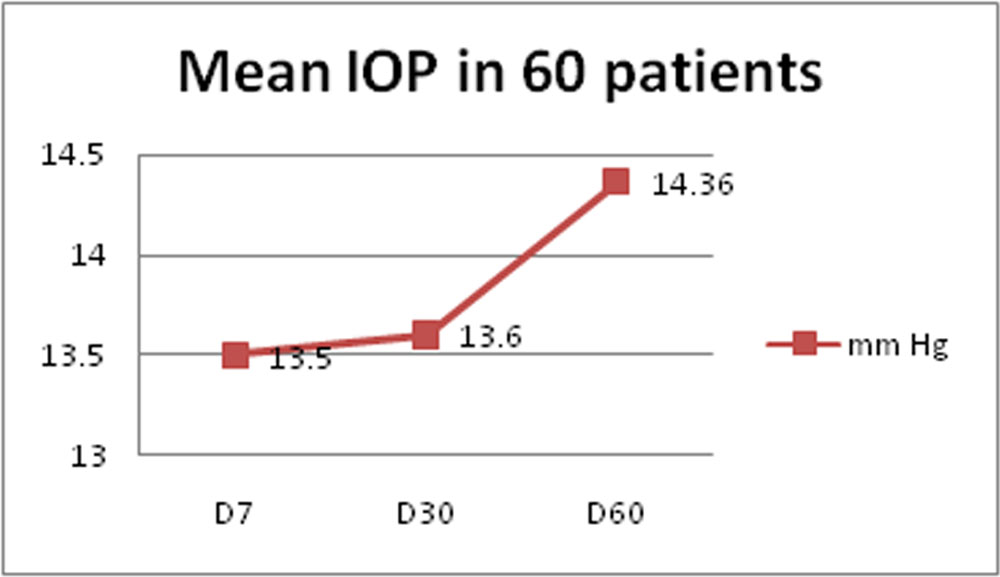
Out of 60 cases, 36 female (60%) and 24 (40%) were male. Mean age was 61 years (SD 10.8). Cataract density showed NS 1 and 1+ in 5 (8.33%), 2 and 2+ in 17 (28.33%), 3 and 3+ in 16 (26.66%) and 4 and 4+ in 22 (33.66%) of cases. UCVA improved in all cases. 72% achieved 6/9 or better vision on day 1, which improved to 95% on day 60. 10% complained of floaters on day 1 which decreased to 6.6% on day 30 and o on day 60. Mean IOP was normal on all visits.
intraoperative complications were encountered in 12 cases which comprised of bleeding in 1 eye (8 %), leakage in 8 eyes (67%), pain in 3 eyes (25 %). There was no case of postoperative endophthalmitis. 100% of cases (60) did not require supplemental medication after surgery. The rate of postoperative cystoid macular edema was nil. All patients expressed happiness over the result and being free from putting eye drops.
OUTCOME
DEMOGRAPHIC PROFILE
| NO OF CASES | 60 |
| Sex [number of patients (%)] | |
| FEMALE | 36(60%) |
| MALE | 24(40%) |
| AGE( YEARS) | |
| MEAN(SD) | 61(10.8) |
| MEDIAN(RANGE) | 62(44-83) |
| CATARACT DENSITY [number of cases (%)] | 60 |
| 1 and 1+ | 5(8.33%) |
| 2 and 2+ | 17(28.33%) |
| 3 and 3+ | 16(26.66%) |
| 4 and 4+ | 22(36.66%) |
| PREOPERATIVE VISION
|
|
|||||||||||||||
|
POST OPERATIVE VISION |
||||||||||||||||||||||||||||||
|
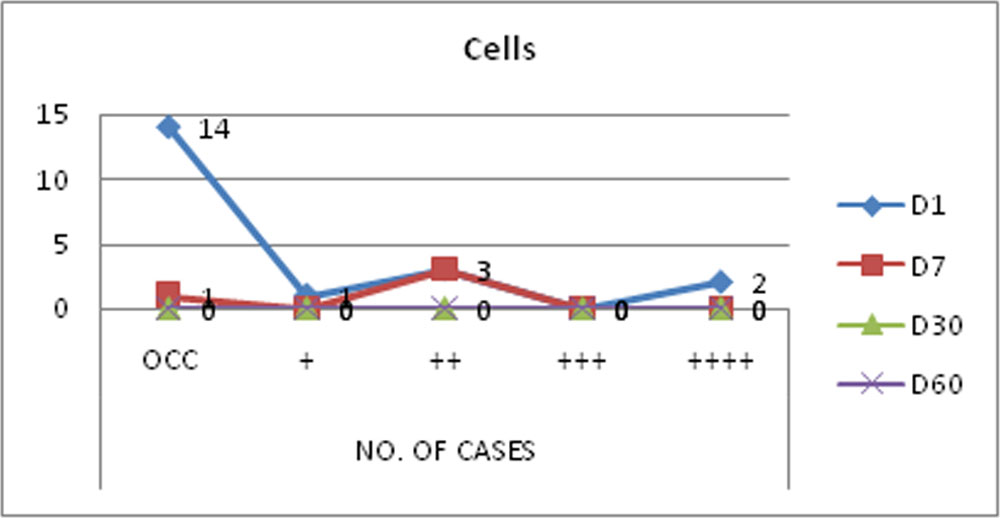
CELLS
| NO. OF CASES | |||||
| OCC | + | ++ | +++ | ++++ | |
| D1 | 14(23.33%) | 1(1.66%) | 3(5%) | 0 | 2(3.33%) |
| D7 | 1(1.66%) | 0 | 3(5%) | 0 | 0 |
| D30 | 0 | 0 | 0 | 0 | 0 |
| D60 | 0 | 0 | 0 | 0 | 0 |
FLOATERS
| NO. OF CASES | |
| D1 | 6(10%) |
| D7 | 5(8.33%) |
| D30 | 4(6.66%) |
| D60 | 0 |
MEAN IOP
| Number of Days | NO. OF CASES | mm Hg (SD) |
| D7 | 60 | 13.5(1.66) |
| D30 | 60 | 13.6(1.79) |
| D60 | 60 | 14.36(1.93) |
DISCUSSION
Immediate post operative foggy vision, appearance of floaters, postoperative IOP rise were issues that made us apprehensive about the procedure. That, none of the patients complained of foggy vision and none had rise of IOP, is the most reassuring aspect of this study. Another rewarding point is that none of the patients had to resort to instillation of any eye drop during the postoperative period for whatsoever reason.
There has been lot of debates regarding usefulness of perioperative antibiotics in prevention of post-cataract endophthalmitis. The ESCRS study is strong proof that intracameral injection of cefuroxime is responsible for five-fold decrease in post-cataract endophthalmitis7. The study was done across Europe and the results were so astounding that it had to be stopped midway to offer the control group the benefit of the result. Intracameral moxifloxacin is used as a prophylaxis in India, Canada and many south American countries. A recent large study published by Aravind Eye Hospital confirms its efficacy in prevention of post-cataract endophthalmitis8. Injection of moxifloxacin into the vitreuos cavity should serve the same purpose as done by intracameral moxifloxacin. Though we did not encounter any endophthamitis in our 60 cases, it should not be taken as conclusive as the strength of this study is very small.
Ocular hypertension following systemic, topical, subtenon and intravitreal steroid is a known phenomenon in steroid responders. It is easy to control in systemic or topical medication as one need to discontinue it. In cases of subtenon and intravitreal, this facility is unfortunately unavailable as long acting steroid is injected for once. Since TA is degradable inside the eye, the initial rise in IOP could be controlled effectively by anti glaucoma medication till the half life of the drug is over. If the situation demands, urgent removal of intravitreal TA, a simple 25 G PPV would suffice to get rid of the complication.
Appearance of floaters and not so ‘wow’ vision immediately after surgery may be a disappointment to the patient unless he or she is thoroughly counseled before the surgery. Fortunately we did not have this problem much.
Failure to give the injection on first attempt was an initial hiccup of this procedure. Since the procedure is blind, there is some learning curve. Though we had to repeat the injection on three occasions in one patient, but it was successful in first attempt in 70% cases. Overall it was successful in all cases.
Intraoperative iris prolapse and bleeding were not difficult to manage as the procedure of phacoemulsification is a closed chamber one.
CONCLUSION
The study clearly demonstrates that this procedure is very effective and safe. If further randomized controlled studies can prove its usefulness, the procedure could be a boon to the working rural population of India for whom putting eye drop during working hours is not only difficult, but unsafe as well. If they could be freed from this burden, their post operative lives will be easier.
REFERENCES
- American Academy of Ophthalmology Cataract and Anterior Segment Panel. Preferred practice Pattern1 guidelines. Cataract in the adult eye. San Francisco, CA: American Academy of Ophthalmology; 2011 ; Available at: https://www.aao.org/preferred-practice-pattern/cataract-in-adult-eye-ppp–october-2011.
- Shoss BL, Tsai LM. Postoperative care in cataract surgery. Curr OpinOphthalmol 2013; 24:66–73.
- HermannMM,U¨ stu¨ndag C, Diestelhorst M. Electronic compliancemonitoring of topical treatment after ophthalmic surgery. Int Ophthalmol 2010; 30:385–390
- An JA, Kasner O, Samek DA, Levesque V. Evaluation of eyedrop administration by inexperienced patients after cataract surgery. J Cataract Refract Surg 2014; 40:1857–1861.
- Vandenbroeck S, De Geest S, Dobbels F, Fieuws S, Stalmans I, Zeyen T. Prevalence and correlates of self-reported nonadherence with eye drop treatment: the Belgian Compliance Study in Ophthalmology (BCSO). J Glaucoma. 2011;20(7):414–421.
- Stringham d jack et al. Dropless Cataract Surgery: What Are the Potential Downsides.ajo.2016.02.001.
- ESCRS Endophthalmitis Study Group. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. J Cataract Refract Surg 2007; 33:978–988
- Haripriya, A., Chang, D. F. & Ravindran, R. D,. Endophthalmitis Reduction with Intracameral Moxifloxacin Prohylaxis. Ophthalmology, 2017.
Leave a Comment