
![]()
Dr. Sheetal Brar, B15612, Dr. Sri Ganesh
ABSTRACT
Purpose: To report the feasibility of implantation and one year mean outcomes of a new design of anterior capsule fixated intraocular lens(IOL)Methods: The new IOL design is a foldable, hydrophilic, open loop PCIOL with two extra PMMA swivel haptics created on the optic surface to capture the anterior capsulotomy after the IOL is implanted in the bag.
Results: The new IOL was implanted in 25 eyes of 25 patients with mean age of 65 years, of which 19 eyes underwent phacoemulsification and 6 eyes had laser cataract surgery.Post-operatively, from 1 week through an average of 12 months( range 5 -18 months) all eyes showed stable refraction and anterior chamber depth with no evidence of decentration or tilt. All eyes had a post-operative residual spherical equivalent (SE) within ±1.5 D. Subjective questionnaire revealed high patient satisfaction with no complaints of dysphotopsia. Two eyes had minimum evidence of PCO at 8 months. No eye required explantation of IOL by the end of mean follow-up.
Conclusion: The new IOL design was feasible to implant and provided satisfactory outcomes in terms of no dysphotopsias or any adverse incidents.However, the long term effects on stabilisation of effective lens position due to capsular contraction, and PCO need to be verified, until all study eyes achieve a minimum post-operative follow-up of 12 months.
Key words:
posterior chamber intraocular lens
swivelhaptics
capsule fixation,
effective lens position,
dysphotopsia
Introduction:
Modern day cataract surgery has become a refractive surgery as patients desire spectacle free vision post operatively. Most of the variables influencing post- operative refraction have been overcome by advancement in keratometery, optical biometery and newer generation intraocular lens( IOL)calculation formulae. [1],[2] However, refractive surprises, IOL tilt, rotation, decentration, PCO, dysphotopsia continue to be the causes of patient dissatisfaction after a perfect cataract surgery. [3]
To overcome these problems, various capsule fixation lenses have been investigated.[4],[5],[6] However, some of these IOL designs may be associated with intra and postoperative complications such as capsulotomy tears, capsular block, iris chaffing and pigment dispersion. Other potential limitations could be difficult and incomplete removal of ocular viscoelastic device (OVD) from the bag behind the IOL, complicated designs and need for special injectors.
Concept of a new design of capsule fixation IOL
The new IOL design is a single piece, open loop, hydrophilic acrylic IOL with 6mm aspheric optic, bearing a 360°square edge and an overall diameter of 13mm. The lens has 2 extra haptics on the optic at 3 and 9 o’clock positions made of PMMA, which can swivel over a pivot. The technical specifications of the IOL design have been provided in Table 1.
Table 1. Specifications of the new “Swivel hapticscapsulotomyfixated IOL” :
| OPTICS CHARACTERISTICS | |
| Powers | +18 D to +24 D |
| Diameter | 6mm |
| Shape | Aspheric |
| Material | UV-blocking hydrophilic acrylic |
| Refractive Index | 1.462 at 35°C |
| Edge design | 360 degrees square edge |
| HAPTICS CHARACTERISTICS | |
| Overall length | 13 mm |
| Fixed haptics | |
| Design | Open/C-loop |
| Material | Hydrophilic acrylic |
| Number | 2 in number |
| Movable(Swivel) haptics | |
| Design | Straight |
| Material | PMMA |
| Number | 2 in number |
| Length | 2 mm |
| Optical A-Constant | 117.5 |
Pre-operative considerations and biometry:The IOL power is calculated using the IOL Master 700(Carl Zeiss Meditec, Germany) using the SRK/T formula. The recommended A-constant used for the new lens is 117.5, considering a relatively anterior position of the IOL compared to in the bag IOLs, where generally the A-constant used is between 118.2 to 118.7.
The new IOL design is suitable for implantation following a routine phacoemulsification or a femtolaser assisted cataract surgery. The most important prerequisite for implantation of this lens is an intact, circular and continuous curvilinear capsulorhexis (CCC) between 5.0-5.5 mm size. Relative contraindications for implantation of this lens are too small or too large capsulotomy, uneven or eccentric capsulotomy, torncapsulotomy, moderate to severe pseudoexfoliation(PXF) and intra-operative posterior capsule rupture or zonular dehiscence associated with vitreous loss.
Loading and implantation of the IOL (video clip1): The IOL can be implanted using a regular pusher type injector through a 2.8 mm incision. While loading, both the swivel haptics are rotated and folded on to the optic using a Sinskey’s hook while aligning them parallel to the longitudinal axis of the IOL. The IOL is then loaded in the cartridge while maintaining this alignment and then injected into the eye through a standard 2.8 mm incision. First, the optic with all the 4 haptics are positioned in the bag. After this, two Sinskey’s hooks are introduced- one from the main port and another from a side port to maneuver the IOL. The side port hook is used to gently push the optic towards the center and stabilize it, while the main port hook is used to rotate the swivel haptic and capture it on to the capsulotomy. In a similar manner, the second swivel haptic is also fixated to the capsulotomy on the other side. Viscoelastic is then aspirated from anterior chamber and the bag by gently tapping on the surface of the IOL. Folds in the posterior capsule at the end of surgery, indicate that most of the viscoelastic has been removed from the bag. Stability of the IOL is checked on table. Upon completion of surgery, wound is hydrated and sealed.
25 eyes of 25 patients (mean age 65 years), were implanted with the new lens and followed up for an average of 12 months (range 5-18 months). All eyes had a least follow- up of 5 months. 19 eyes had phacoemulsification, while 6 eyes had femto assisted laser surgery.The study was approved by the institutional ethics committee of our hospital and informed consent was obtained by all patients participating in the study.
RESULTS
Initial experience suggested that the IOL was feasible and safe to implant without any intraoperative complications of capsulotomy tears or haptic breakage while capturing the swivel haptic on to the capsulotomy. None of the lenses were explanted.
Figure 1.shows results of post-op SE predictability: 7 eyes had post op SE within ±0.5 D, while all eyes had post-op SE within ±1.5 D at the end of mean follow-up period.
Post-operatively, dilated clinical photography showed stable position of the lens and swivel haptics with no evidence of decentration, tilt or rotation.Figure 2 shows the clinical photographs of an eye implanted with the new IOL following routine phacoemulsification at 2 week and 6 months follow up.
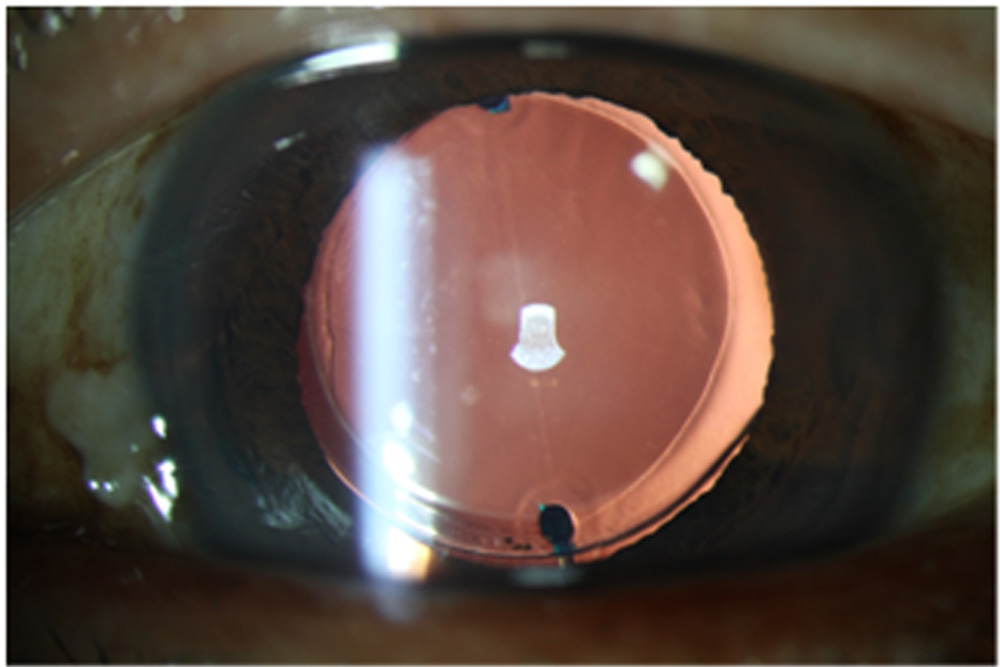
RE 2 week Post-Op
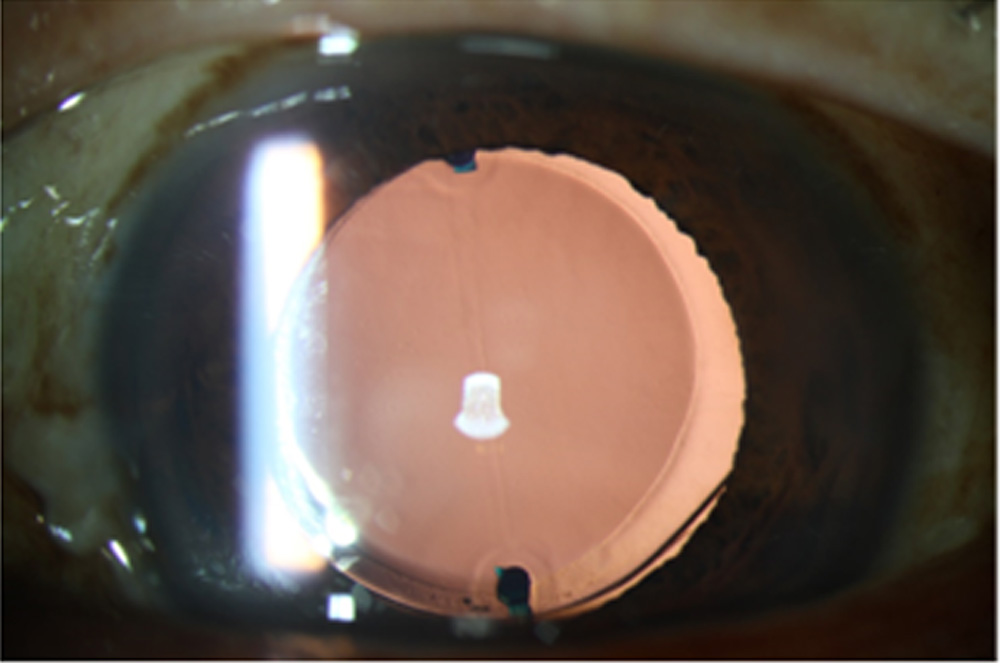
RE 6 month Post-Op
Note the stable position of the swivel haptics without any tilt or decentration over time. Anterior chamber depth(ACD) measured with IOL Master 700 also showed no significant change at 12 months mean follow-up (4.26 mm) compared with two week follow up (4.24 mm)( p-value =0.08).
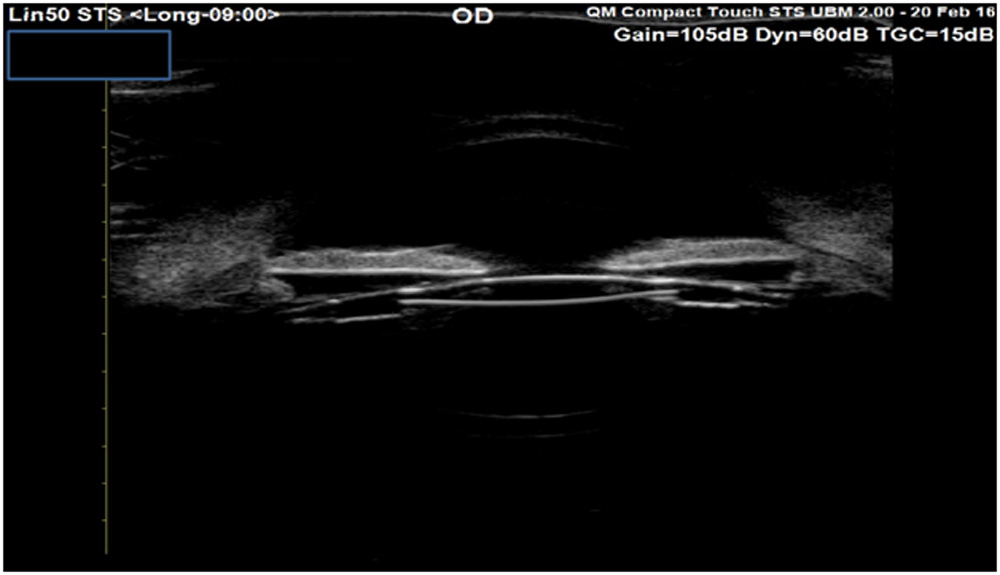
Ultrasound Biomicroscopy (UBM) demonstrated the effective lens position(ELP) to be more anterior and just behind the iris plane as compared to conventional in the bag lenses, where it is expected to be more posterior (Figure 3).
No evidence of iris chaffing, pigment dispersion, secondary glaucoma or capsular block syndrome was observed in any of the eyes implanted with the new IOL at the end of the mean follow-up. Two eyes had evidence of mild visually non –significant PCO beginning at 8 months, which did not require YAG capsulotomy.
Discussion: The new swivel haptics anterior capsule fixated IOL design potentially overcomes most of the limitations of the previously introduced capsulotomy fixation IOLs. Bag- in- the- lens(BIL, Morcher GmbH, Stuttgart, Germany) was the first capsulotomy fixated IOL introduced in 2006, mainly for the purpose of obviating the need of Yag laser capsulotomy. [4]The long-term outcomes in adult and pediatric eyes showed the IOL to be safe for implantation and effective for reducing the incidence of PCO. However, the surgical technique involved placement of the anterior and posterior capsules in the IOL’s groove after a capsulorhexis of the same size created in both capsules using a special anterior capsulorhexis ring caliper. [7]Therefore, this surgical technique appears to be more challenging , thus requiring a higher degree of surgical skill.
The 90F intraocular lens (Morcher GmbH, Stuttgart, Germany) has the design of a C-loop intraocular lens with an additional flank. In contrast to the femtosecond laser-assisted in-the-bag lens technique, only the anterior capsule is fixated in the side flank, whereas the posterior capsule is kept intact and the IOL is implanted in the capsular bag.[5]However, the risk of tearing of capsulotomy or capsular block syndrome still needs to be evaluated with this lens. The new swivel haptics anterior fixated IOL, by virtue of its simple design and lesser manipulation of the capsulotomy may be potentially associated with lesser risk of capsulotomy tears.Also, observation of folds in the posterior capsule at the end of surgery suggested, almost a complete removal of the OVD, minimizing the chances of capsular block syndrome due to OVD retention in the post-operative period.
Preussner et al emphasized that knowledge of post-operative ACD is important to accurately predict the postoperative IOL position and refraction[8]. This, however, cannot be easily predicted as the capsular bag size differs in individuals and there is a variable degree of capsular contraction over time. Following the new IOL implantation, however, the IOL position is shown to be just behind the iris (on UBM) due to capsule fixation, negating the influence of bag size on the effective lens position(ELP) to a great extent. This may help better prediction of post-operative ACD, based upon which the A-constant can be refined for improving predictability of post-operative refraction. Thus, a stable fixation and ELP may be achieved which may not be influenced by capsular changes overtime.However, this aspect needs to be verified over a longer follow-up period i.e. all eyes completing at least 12 months follow-up.
According to one of the theories, negative dysphotopsias(ND) were more likely to develop in postoperative eyes in which there was a larger distance between the back of the iris and the anterior capsule of the lens[9]. Since the new IOL is captured on to the anterior surface of the capsulotomy, it brings the IOL position more anterior compared to in the bag lenses, thus reducing the distance between back of the iris and anterior lens capsule, consequently preventing negative dysphotopsias. However, the MasketTM ND IOL negates dysphotopsia through a different mechanism by allowing for the implant to be capsule bag fixated and provides a flange of the anterior optic edge to override the anterior capsulotomy[6].
Regarding the occurrence of PCO, it may be proposed that the incidence of PCO with new swivel haptic IOL may be similar to the conventional in the bag IOLs. This may be due to the uniform shrink wrap effect and the 360° square edge of the IOL optic preventing the lens epithelial cells(LECs) to migrate and proliferate towards the optical center[10]. Two eyes showed minimum PCO at 8 months, which was not significant and did not require YAG capsulotomy.Since all eyes did not reach 12 months follow-up and the minimum follow- up was 5 months, the long term outcomes in terms of PCO development still need to be seen until all eyes complete 12 months follow-up.
Other potential advantages are-simple design, easy to manufacture and pack, can be used with standard injector through 2.8 mm incision and needs no special instruments or surgical training. Also, the swivel haptic fixation ensures rotational stability which may provide significant advantage for toric designs, irrespective of bag size.Lastly, the IOL is easy to explant by simple disengagement of the swivel haptics, if required.
In conclusion, our initial experience with the new IOL with swivel haptic capsule fixation suggests that it may be a safe and feasible alternative to the conventional PCIOL designs potentially providing a stable IOL position and low incidence of dysphotopsia, and without any visually threatening intra or post- operative complications. However, prospective clinical trials with a larger number of patients are necessary to confirm these early findings, investigate long-term results in terms of effective lens position stabilization and PCO and to optimize A- constants.
REFERENCES
1. Cooke DL, Cooke TL. Comparison of 9 intraocular lens power calculation formulas. J Cataract Refract Surg 2016;42(8):1157-64
2. Shajari M, Cremonese C, Petermann K, Singh P, Müller M, Kohnen T. Comparison of Axial Length, Corneal Curvature, and Anterior Chamber Depth Measurements of 2 Recently Introduced Devices to a known Biometer. Am J Ophthal 2017 ;178:58-64.
3.Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35(6):992-7
4. Tassignon M-JBR, De Groot V, Vrensen GFJM. Bag-in-the-lens implantation of intraocular lenses. J Cataract Refract Surg 2002; 28:1182–1188
5. Burkhard Dick H.B, Schultz T. Intraocular Lens Fixated in the Anterior Capsulotomy Created in the Line of Sight by a Femtosecond Laser. J Refract Surg 2014;30(3):198-201
6. Masket S, Fram NR. Pseudophakic negative dysphotopsia: surgical management and new theory of etiology. J Cataract Refract Surg 2011; 37:1199–1207
7. Tassignon M-J, Rozema JJ, Gobin L.A ring-shaped caliper for better anterior capsulorhexis sizing and centration. J Cataract Refract Surg 2006; 32:1253–1255
8. Preussner PR, Wahl J, Weitzel D, Berthold S, Kriechbaum K, Findl O. Predicting postoperative intraocular lens position and refraction .J Cataract Refract Surg. 2004;30:2077-83.
9.Henderson BA, Geneva II. Negative dysphotopsia: a perfect storm. J Cataract Refract Surg 2015;41:2291-312
10. Schmidbauer JM, Escobar-Gomez M, Apple DJ, Peng Q, Arthur SN, Vargas LG. Effect of haptic angulation on posterior capsule opacification in modern foldable lenses with a square, truncated optic edge.J Cataract Refract Surg 2002;28:1251-5.
Legends
Table 1.Specifications of the new IOL.
Figure 1. Post-operative SE predictability at the end of mean follow-up
Figure 2. Clinical photograph of an eye at 2 weeks and 6 months after implantation of the swivel-haptics capsule fixation IOL showing a stable position of IOL, without any rotation, tilt or decentration
Figure 3. Ultrasound Biomicroscopy(UBM) of an eye at 2 weeks post implantation of the swivel-haptics capsule fixation IOL showing the effective lens position of the IOL to be just behind the iris and much anterior compared to conventional in the bag implantation
Leave a Comment