
Dr. Sheetal Brar, B15612, Dr. Vandana John Serrao, Dr. Sri Ganesh
Abstract
Purpose– To compare the safety, efficacy and predictability of femtosecond enabled anterior penetrating and intrastromal corneal incision for the correction of pre-operative astigmatism at the time of cataract surgery
Methods– This prospective, randomized, comparison study included 51 eyes from 51 patients who underwent femtolaser assisted cataract surgery with the Catalys Precision System(J&J), of which 26 eyes received anterior penetrating and 25 eyes received intrastromal arcuate incisions for correction of corneal astigmatism in the range of 0.75 to 2.00 D of astigmatism. Follow-up was conducted at 1 week, 1 month and 6 months post-op. Vector analysis of astigmatism was performed using the Alpins method with ASSORT software.
Results-The mean pre-operative keratometric astigmatism and Target Induced Astigmatism(TIA) were 0.98 and 1.02 D in the AP group and 1.25 and 1.29 D in IS group respectively. There was no statistically significant difference between the post-operative keratometric astigmatism (AP=0.63, IS=0.69, P-value=0.2) and Surgically Induced Astigmatism(SIA)(AP=1.01, IS=0.85, P-Value=0.40) at 6 months post-op. Both groups demonstrated slight overcorrection shown by a comparable Correction Index(CI) of 0.96 and 0.94(p-value=0.98),although there was a wide variation in CI with 30% eyes in AP and 24% eyes in IS group showing overcorrection( CI>1).92% eyes in IS and 72% eyes in AP group were within ±0.5 D of astigmatism.
Conclusion-Both anterior penetrating and intrastromal incisions were safe and effective and demonstrated good predictability for astigmatism correction using femtolaser technology. However, both incisions showed a wide variability with a significant number of eyes getting overcorrected with time.
Key words: Femtolaser incisions, penetrating , intrastromal , astigmatism
Introduction
Astigmatic keratotomy has been a mainstay of low to moderate surgical astigmatism management during cataract surgery for years.1 Although effective, results with manual incisions can be unpredictable, even with advanced nomograms.2,3 The use of intraoperative aberrometry has improved predictability of manual incisions; however, results are subject to multiple intraoperative factors. The use of femtosecond lasers for limbal relaxing incisions (LRIs) has been described previously, to treat high astigmatism after penetrating keratoplasty and mixed astigmatism after previous refractive surgery.4,5 With the advent of femtosecond lasers for refractive laser-assisted cataract surgery, more surgeons have been able to take advantage of this technology and refine their nomograms and algorithms.6 This study aims at comparing the safety, efficacy and predictability of two types of arcuate incisions which can be created using the femtolasers for the correction of pre-operative astigmatism at the time of cataract surgery.
Materials and Methods
This prospective, non- randomised study was approved by institutional ethics committee and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients participating in the study.
Inclusion criteria were- patients undergoing cataract surgery for age related cataract who were between 40-70 years of age, with a minimum astigmatism of -0.75 D on corneal topography.
Eyes with features of corneal ectatic conditions on topography, corneal scars, pterygium, post refractive surgery, small palpebral fissures, small/ insufficiently dilating pupil, mature or intumescent cataracts, glaucoma, retinal pathologies, patients on systemic steroids, immune suppressants, were excluded from the study.
Preoperative evaluation
All patients underwent a thorough preoperative evaluation including anterior and posterior segment examination, manifest refraction, assessment of corrected distance visual acuity, corneal topography using Pentacam HR (Oculus Optikgeräte GmbH, Wetzlar, Germany), specular microscopy (Tomey, Japan),macular OCT( Optovue, Fremont , US).
IOL power was calculated by using three established formulae: SRK/T, Holladay II, and Haigis. The newer generation formulae – Haigis and Holladay II – performed well across a very wide range of axial lengths.They were combined to calculate the IOL power in emmetropic eyes; the SRK/T was excellent for long myopic eyes, and Haigis formula for hyperopic eyes. The refractive target was emmetropia to -0.25 D in all cases. All values were obtained by using partial coherence interferometry with swept source OCT(IOLMaster 700; Carl Zeiss Meditec AG).
Surgical Procedure and Planning of Intrastromal arcuate incisions: All surgical procedures were performed by a single experienced surgeon (SG), using the Catalys laser system (Johnson &Johnson, Inc.), software version 2.20.The programmed anterior capsulotomy size was 5.0 mm in all eyes, and crystalline lens fragmentation was performed using a standardized template.
Intrastromal AKs were planned using the Julian Steven Software version4 . A personal nomogram was used for intrastromal AKs (v3B) . All intrastromal AKs were 8.0 mm diameter paired symmetrical arcs and were limbal centered. The arcs were programmed to be intrastromal, nonpenetrating, with a depth between 20% and 80% of corneal pachymetry as measured locally by the laser system integral optical coherence tomography. Other intrastromal AK parameters were 90-degree side-cut angle; horizontal and vertical spot spacing of 5 mm and 10 mm, respectively; pulse energy of 5 mJ; anterior line density of 5; anterior line distance of 20 mm; and central line density of 4.
Anterior Penetrating AKs were planned using LRIcalculator.com website which is intended to give limbal relaxing incisions at the limbus5. However, for the 8 mm diameter, the obtained values of arc lengths were reduced by 20% before entering into the femtolaser.
Eye was marked in horizontal 0-180 degrees axis and the inner horizontal marks on the suction ring were manually aligned with the limbal marks before application of suction and laser delivery to ensure that the intrastromal AKs were placed at the required corneal meridian.
Cataract removal was completed by a standard phacoemulsification procedure using a Whitestar Signature phacoemulsification system (Johnson &Johnson, Inc.). A 2.8 mm clear corneal temporal main incision and one 1.5 mm side port (at 90 degrees and to the left of the main incision) were created using diamond keratomes. All surgeries were uneventful and no anterior or posterior gas breakthrough or opening of incisions was seen in intrastromal group as reported earlier. 7,8
Postoperative medications included topical 0.3% Ofloxacin (Exocin®, Allergan, Irvine, U.S.A.) 4 times for 2 weeks, 0.1% prednisolone acetate eye drops (Pred Forte®, Allergan, Irvine, U.S.A.) in tapering dosage for 6 weeks, 0.5 % Nepafenac eye drops 3 times a day for 4 weeks and lubricants 4 times for 4 weeks or more.
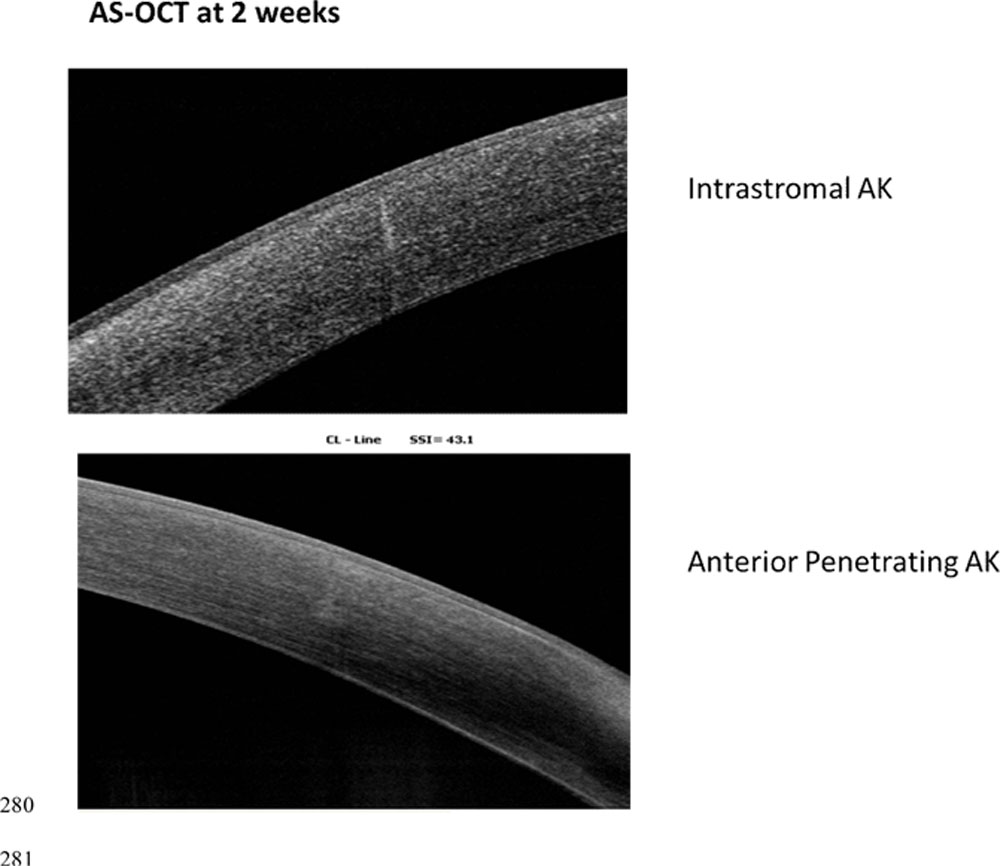
Patients were followed up on postoperative day 1, 1 week, 1 and 6 months. On all review visits from 2 week onwards, assessment of UDVA, manifest refraction, corrected distant visual acuity (CDVA), topography and AS-OCT was also performed. Figure 3 shows AS-OCT of two eyes which received anterior penetrating and intrastromal arcuate incisions with femtolaser at 2 weeks post –op.
Statistical Analysis: SPSS software for Windows version 17.0.0 (IBM Corp., Armonk, NY) was used for statistical analysis .All values were expressed as mean ± standard deviation (SD). Independent sample t test was carried out for intergroup comparison and paired t test was used for intragroup comparison of means. A p-value of 0.05 or less was considered statistically significant. JRS standard graphs were generated using Datagraph-med 5.20 software.
Vector analysis of astigmatism
Only the left eyes were included in the analysis. Astigmatism outcomes were reported according to standardised format. Refractive astigmatism at the spectacle plane was converted to the corneal plane using vertex distance of 12 mm. It was then analysed with vector analysis of Alpins using the Assort software , with consideration of the change in the astigmatic axis, measuring three vectors and relationships among them. The target-induced astigmatism vector (TIA), defined as the astigmatic change that the surgery was intended to induce; the surgically induced astigmatism vector (SIA), defined as the astigmatic change that the surgery actually induced; and the difference vector (DV), defined as the induced astigmatic change that would enable the initial surgery to achieve its intended target or the postoperative astigmatism. Magnitude of error (ME) is the arithmetic difference between the SIA and TIA. Angle of error (AE) is the angle between the axis of the SIA and TIA. The flattening index (FI) is a measure of the impact of an astigmatic treatment at off-axis orientation on the astigmatic change at its intended axis.9,10
Results
Twenty six eyes underwent astigmatism correction with Anterior Penetrating and 25 eyes using the Intrastromal incisions. All patients completed a mean follow-up of 6 months. Pre-operatively, both the groups were matched in terms of mean age, corneal thickness, mean keratometery, corneal astigmatism( Pentacam), axial length and IOL powers implanted( Table1).
Post-operative visual and refractive results
Post-operatively at 6 months, both groups showed significant reduction in mean residual corneal astigmatism, which reduced from 0.98±0.35D to 0.63±0.27D in AP group and 1.25±0.33D to 0.692 D in IS group( p<0.05 for both groups). There was no significant differences between the visual and refractive outcomes also at 6 months, wherein the post-operative residual sphere, cylinder, spherical equivalent(SE) mean keratometery and Corrected Distance Visual Acuity( CDVA) was comparable between the two groups( p values >0.05 for all parameters), ( Table 2).
Vector analysis of astigmatism
Vector analysis of astigmatism showed that both groups has comparable TIA before surgery(p=0.13). Six months after the surgery, both groups had comparable results in terms of SIA, CI, IOS, ME and AE (p-values >0.05 for all parameters), Table 3. Although statistically, there was no significant differences in the outcomes with vector analysis, the results were clinically better in the AP group compared to IS group, with the distribution of post-operative refractive astigmatism showing that 92% eyes in AP and 72% in IS group achieved post-op cyl ±0.5D and all eyes in AP group were within ±1.00 D and all eyes in IS group were within ±1.25 D( Fig 1).
Vector analysis showed comparatively favourable outcome in AP group, however difference was statistically not significant.
Comparing the CI, both groups showed a high percentage of eyes with overcorrection which was 30% and 24% in AP and IS groups respectively(Fig 2).
Discussion
Limited data is available on the outcomes of femto arcuate incisions for simultaneous correction of astigmatism at the time of cataract surgery. Day et al studied the effectiveness of femto intrastromal arcuate incisions and concluded that they could be easily programmed as an integral part of the treatment planning and significantly reduced corneal astigmatism at a relatively short follow-up of one month post-operative. However, they observed a mean correction index of 0.63 (undercorrection of 37%), with 75 eyes getting overcorrected.6 In contrast, our study saw a much higher CI for intrastromal group compared to theirs (0.94), suggesting a very minor undercorrection of 6%. The %age of eyes being overcorrected was also much higher 24% compared to 7% in their study. Chan et al studied the vector analysis of corneal astigmatism using the penetrating arcuate incisions created by the Victus femtolaser system(B&L). They used a Bespoke nomogram with a single AK paired with the main wound.They found a mean CI value of 0.86 with greater variability in AK efficacy and a higher rate of overcorrection and attributed the same to angle error (angle between the intended axis and the axis of the actual incisional effect ), which was implicated as a cause of variability in AK efficacy.11 In the present study also, we observed similar results in anterior peneterating group, where our CI was 0.96 and 30% eyes were overcorrected. In our study, the angle error was 18 deg in IS and 15 deg in AP group, representing imperfect AK placement or variations in AK construction in both groups.
Various factors that may contribute to angle error are – Variation in corneal pachymetry by location12(with midperipheral corneal thickness being greater in the superior and nasal regions than in the inferior and temporal regions), eye rotation or coronal x-y movement during femtosecond laser delivery following initial planning(Low suction)13, incomplete cylinder correction due to tissue bridges or gas escape, eye tilt following docking : arcs placement not orthogonal to the surface,loose conjunctiva, differences in corneal biomechanics14 and white to white diameter measurements (incisions placed at fixed diameter of 8 mm). Despite this variability in results, the visual outcomes were satisfactory and all eyes in both groups were within ±1.25 D.
In conclusion, both AP and IS femto arcuate incisions were safe and effective through a 6 month follow-up and significantly reduced corneal cylinder post-op, however the AP group showed clinically better results compared to IS group.Potential limitations of our study are relatively small sample size and short follow-up , since corneal relaxing incisions are known to regress with time.15 Nevertheless, to our knowledge this is the first study comparing the two types of arcuate incisons created by a single laser platform. There were between-eye variances in astigmatism vector reduction due to angular error in both groups, expected based on previous studies of manual astigmatic keratotomy. Hence we need longer follow-up and further understanding of the factors influencing the efficacy of intrastromal and penetrating AK is required to optimize outcomes.
Legends:
Figure 1 Post-operative residual cylinder between both groups at 6 months.
Figure 2. Compariosn of Correction Index and eyes which got over corrected between both groups at 6 months.
Table 1. Pre-operative baseline characteristics of patients included in the study (n=51 eyes)
Table 2. Comparison of visual and refractive results between both the study groups at 6 months
Table 3. Vector analysis comparison between both groups at 6 months.
References
- Amesbury EC, Miller KM. Correction of astigmatism at the time of cataract surgery. Curr Opin Ophthalmol 2009; 20:19–24
- Kaufmann C, Peter J, Ooi K, Phipps S, Cooper P, Goggin M; for the Queen Elizabeth Astigmatism Study Group. Limbal relaxing incisions versus on-axis incisions to reduce corneal astigmatism at the time of cataract surgery. J Cataract Refract Surg 2005; 31:2261–2265
- Price FW, Grene RB, Marks RG, Gonzales JS; and the ARC-T Study Group. Astigmatism reduction clinical trial: a multicentre prospective evaluation of the predictability of arcuate keratotomy; evaluation of surgical nomogram predictability. Arch Ophthalmol 1995; 113:277–282
- Viswanathan D, Kumar NL. Bilateral femtosecond laser–enabled intrastromal astigmatic keratotomy to correct high post-penetrating keratoplasty astigmatism. J Cataract Refract Surg 2013; 39:1916–1920
- Venter J, Blumenfeld R, Schallhorn S, Pelouskova M. Nonpenetrating femtosecond laser intrastromal astigmatic keratotomy in patients with mixed astigmatism after previous refractive surgery. J Refract Surg 2013; 29:180–186
- Day A, Lau N, Julian S. Nonpenetrating femtolaser intrastromal astigmatic keratotomy in eyes having cataract surgery. J Cataract & Refract Surg. 2016(42)-47
- Kankariya VP, Diakonis VF, Kymionis GD, Yoo SH. Anterior gas breakthrough during femtosecond intrastromal astigmatic keratotomy (FISK) [letter]. J Refract Surg 2014; 30:511–513
- Cherfan DG, Melki SA. Corneal perforation by an astigmatic keratotomy performed with an optical coherence tomography guided femtosecond laser. J Cataract Refract Surg 2014; 40:1224–1227
- Alpins NA. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg 1993; 19:524–533
- Alpins N. Astigmatism analysis by the Alpins method. J Cataract Refract Surg 2001; 27:31–49
- Chan TCY, Cheng GPM, Wang Z, Tham CCY, Woo VCP, Jhanji V. Vector analysis of corneal astigmatism after combined femtosecond-assisted phacoemulsification and arcuate keratotomy. Am J Ophthalmol 2015; 160:250–255
- Ueno Y, Hiraoka T, Miyazaki M, Ito M, Oshika . Corneal Thickness Profile and Posterior Corneal Astigmatism in Normal Corneas. Ophthalmology 2015;122:1072-1078
- Febbraro JL, Koch DD, Khan HN, et al. Detection of static cyclotorsion and compensation for dynamic cyclotorsion in laser in situ keratomileusis. J Cataract Refract Surg. 2010;36:1718–1723.
- Sharifipour F, Panahi-Bazaz M, Bidar R, Idani A, Cheraghian B.Age-related variations in corneal biomechanical properties. J Curr Ophthalmol. 2016 Jun 11;28(3):117-22
- Lim R, Borasio E, Ilari L. Long-term stability of keratometric astigmatism after limbal relaxing incisions. J Cataract Refract Surg 2014; 40:1676–1681
| Pre-op | Group 1(IS) | Group2(AP) | P-value |
| AGE(years) | 63.16±8.35 | 67±8.89 | 0.11 |
| K1(D) | 43.58 ±1.70 | 43.58±1.34 | 0.83 |
| K2(D) | 44.28 ±1.82 | 44.22±1.39 | 0.76 |
| K MEAN(D) | 44.05 ±1.71 | 43.93±1.35 | 0.58 |
| CORNEAL ASTIG(D) | 1.25±0.33 | 0.98±0.35 | 0.78 |
| CCT(µm) | 529±36.73 | 523±32.27 | 0.19 |
TABLE 2.
| Group1(AP) | Group 2(IS) | P-value | |
| SPH(D) | -0.04±0.21 | -0.01±0.19 | 0.51 |
| CYL(D) | -0.35±0.39 | -0.18±0.29 | 0.07 |
| SE(D) | -0.22±0.28 | -0.1±0.23 | 0.08 |
| K1(D) | 43.74±1.35 | 43.67±1.64 | 0.97 |
| K2(D) | 44.17±1.31 | 44.39±1.75 | 0.51 |
| K MEAN(D) | 43.95±1.32 | 44.02±1.68 | 0.85 |
| CDVA
(LogMAR) |
-0.02±0.04 | 0.00±0.04 | 0.15 |
Table 3.
| Group 1(IS) | Group2(AP) | P-value | |
| SIA | 1.01±0.70 | 0.85±0.61 | 0.40 |
| TIA | 1.29±0.66 | 1.02±0.59 | 0.13 |
| DV | 0.77±0.46 | 0.56±0.26 | 0.06 |
| CI | 0.94±0.82 | 0.96±0.68 | 0.98 |
| IOS | 0.87±0.97 | 0.73±0.53 | 0.52 |
| ME | -0.26 ± 0.46 | -0.16 ± 0.45 | 0.43 |
| AE | -5.28 ± 27.66 | 3.42 ± 24.18 | 0.23 |
| AE ABS | 18 ± 21.36 | 15.65 ± 18.50 | 0.33 |
Figure1.
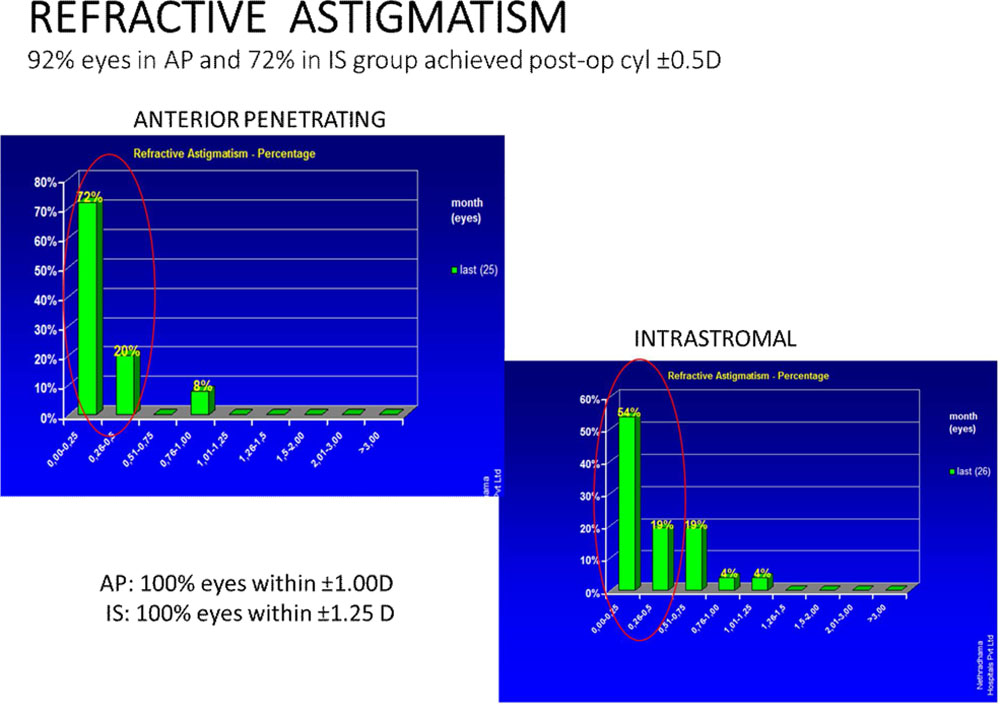
Figure 2.
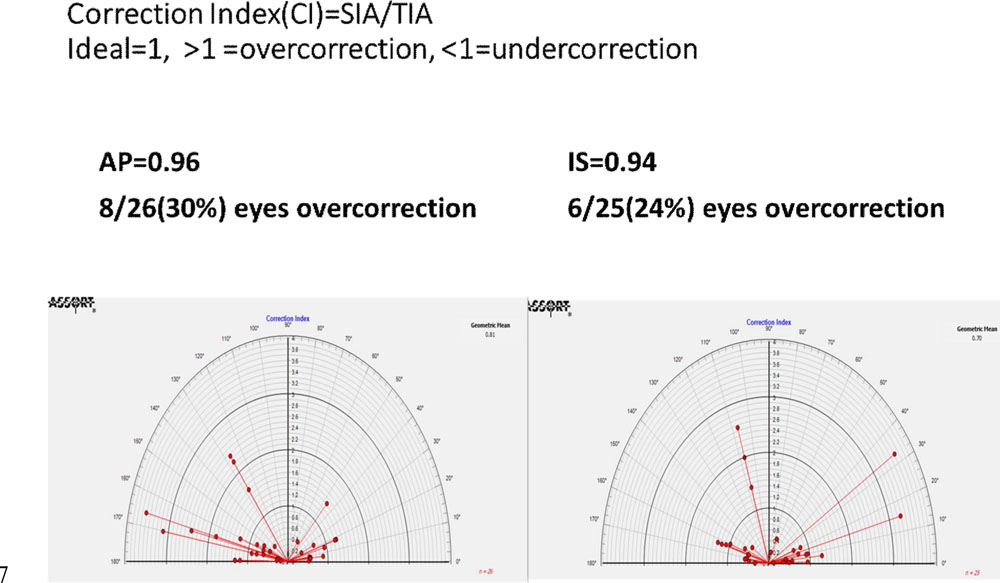
Figure 3.
Leave a Comment