
![]()
Dr. Jay Sheth, S18167, Dr. Mahesh G, Dr. Shruti Chandra, Dr. Giridhar Anantharaman
ABSTRACT
Purpose:Intravitreal ziv-aflibercept(IVZ) is emerging as a low-cost alternative for management of macular disorders in developing countries. The purpose of our study was to evaluate the short-term safety and efficacy, including morphological response of IVZ based on spectral-domain optical coherence tomography (SD-OCT) in diversechorioretinal disorders.
Methods: Prospectively, 10 eyes with varied pathologies such asPCV(3 eyes), Wet AMD(3 eyes), chronic CSCR(2 eyes) &neovasculopathy(PCN; 2 eyes) underwent IVZ therapy. At baseline, all patients underwent multimodal imaging including SD-OCT, ICGA, DFA & FAF(Spectralis) while SD-OCT was repeated at 1 month. Changes in BCVA, intraretinal fluid(IRF), subretinal fluid(SRF), subfovealchoroidal thickness(SFCT), along with dimensions(height,base diameter, area) of PED at maximum extent& shallow irregular PED(Double layer sign;DLS) were analysed at baseline & at 1 month.Detailed analysis of outer retinal layers(Ellipsoid zone, ELM, Hyperreflective dots), DRIL & VMIA was performed too.
Results: Compared with baseline, significant reduction was seen in height, base diameter& area of PED respectively (p=0.02, p=0.01, p=0.02) at 1 month. Statistically significant reduction was also noted in SFCT (p=0.0009), DLS height (p=0.01)& SRF height (p=0.01). 40% & 37.5% of eyes had complete resolution of IRF & SRF respectively. Improvement was noted in BCVA, DLS width & CMT, although not significantly. On detailed analysis, one eye showed complete resolution of DLS. At baseline, RPE rip was present in 7 eyes which showed early resolution in 2 eyes. Similarly, ELM disruption showed improvement in 4 out of the 9 eyes while ellipsoid disruption did not show any sign of restoration at one month in all 10 eyes. Likewise, disorganization of inner retinal layers (DRIL) improved in 1 out of the 5 eyes while reduction in hyperreflective dots was seen in 7 out of the 10 eyes. One eye has ERM which remained unchanged. None of the patients experienced any serious ocular or systemic adverse events.
Conclusion: Single intravitreal injection of ziv-aflibercept has promising anatomical outcomes on PED, besides achieving a dry macula, maintaining stable visual acuity with an acceptable safety profile.Morphometric improvement in choroidal thickness and integrity of disorganized retinal layers along with its low-cost favours its use as an efficacious anti-VEGF agent in the developing world.
INTRODUCTION
Anti-vascular endothelial growth factor (Anti-VEGF) therapy have become the treatment of choice for choroidal neovascularization secondary to wet age related macular degeneration (ARMD) and pachychoroid disorders.1, 2 Currently, the US-FDA (Food and Drug Administration) has approved pegaptanib (Macugen; Eyetech, New York, NY), ranibizumab (Lucentis; Genentech, S. San Francisco, CA/Roche, Basel, Switzerland), and aflibercept (Eylea; Regeneron, Tarrytown, NY) for intraocular use.3-5 However, in the American society of Retina Specialists (ASRS) Preferences and Trends Survey conducted in 2015, which was on basis of the current body of literature and considering the cost-effectiveness of bevacizumab (Off-label use; AVASTIN, Genentech, Inc.), 64% of the US retinal physicians used bevacizumab as the first-line treatment for AMD and &> 80% of US members treated choroidal neovascularization from histoplasmosis and other non-AMD causes with bevacizumab.6
Amongst the anti-VEGF agents, aflibercept is emerging as an effective alternative, especially for non-responders. However, the cost of aflibercept ($1,850/dose) is major hindrance for its widespread use, especially in developing nations. Ziv-aflibercept (Zaltrap; Regeneron) is a recombinant fusion protein of 115 kDA, composed of the extracellular VEGFbinding domains from human VEGF receptors 1 and 2 fused to the Fc portion of a human IgG1.7 It is approved by the FDA for management of metastatic colorectal carcinoma.7 Its off-label intravitreal use has been documented to be safe and effective for management of chorioretinal pathologies such as wet AMD, polypoidal choroidal vasculopathy (PCV), diabetic macular edema (DME) and so on.8, 9 However, a detailed evaluation of multimodal imaging features secondary to IVZ remains unexplored.
The purpose of our study was to perform a comprehensive morphometric analysis of efficacy of IVZ in variety of chorioretinal disorders. Additionally, we also evaluated the ocular and systemic safety profile of IVZ therapy.
METHODS
It was a prospective study of 10 eyes of 9 patients with varied chorioretinal disorders presenting to the VitreoRetina Clinic of Giridhar Eye Institute, India, between January 2017 and February 2017. The study was conducted in accordance to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board. Written informed consent was obtained from each patient.
The etiologies included polypoidalchoroidalvasculopathy (PCV; 3 eyes), wet age related macular degeneration (Wet AMD; 3 eyes), chronic central serous chorioretinopathy (CCSCR; 2 eyes) &pachychoroidneovasculopathy (PCN; 2 eyes).
At baseline and at one month, all patients underwent detailed clinical evaluation including assessment of best corrected visual acuity (BCVA) on Snellen chart, intraocular pressure (IOP) measurement by Goldmannapplanation tonometry (AT), along with anterior segment and fundus evaluation by slit-lamp biomicroscopy and indirect ophthalmoscopy. Multimodal imaging was performed including spectral domain optical coherence tomography (SD-OCT); Central macular thickness [EDI-OCT], fundus autofluorescence (FAF), digital fluorescein angiography (DFA), and ICGA(Spectralis HRA + OCT, Heidelberg Engineering, Heidelberg, Germany)while SD-OCT was repeated at 1 month.
Image Analysis
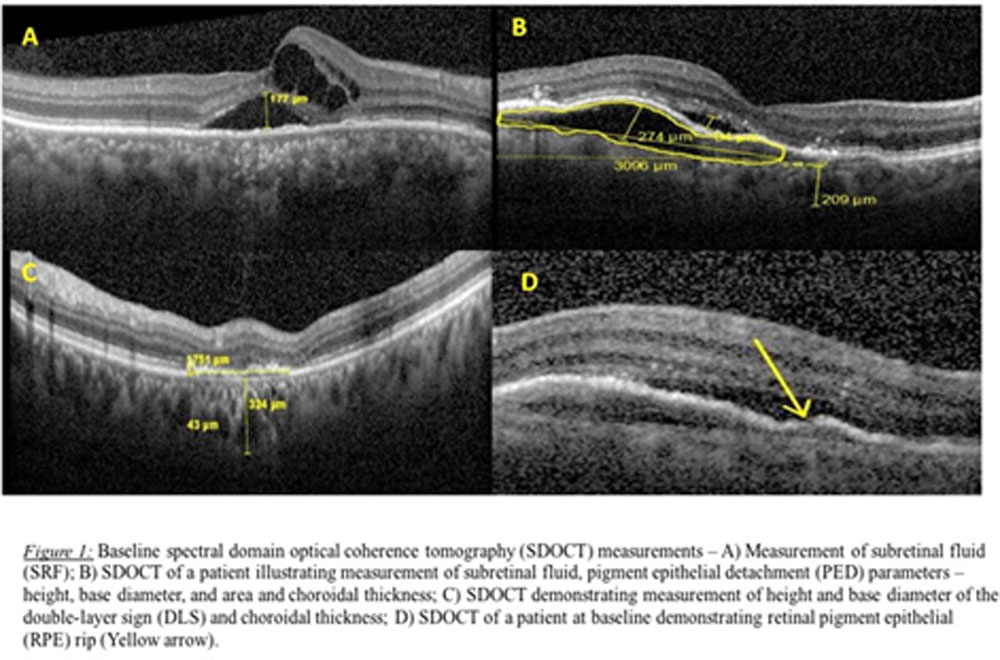
Subfovealchoroidal thickness (SFCT) was measured manually with the help of built-in calipers in OCT software(Figure 1). Measurements were taken from the outer portion of hyperreflective line corresponding to the RPE to the inner portion of hyperreflective zone corresponding to the choroidoscleral junction by a single masked observer (J.S.). They were obtained in the subfoveal region (subfovealchoroidal thickness; SFCT). Automated central macular thickness (CMT) was also calculated using the 25-line raster scan protocol.
A dense scan was carefully analysed to look for maximum extent of PED and Double layer sign (DLS; defined as two hyperreflective layers separated by a gap – the inner layer is the hyperreflective irregularly elevated RPE and the outer layer is the inner layer of the Bruch’s membrane) and subsequently, their dimensions including the height, width and area were calculated using the built-in calipers (Figure 1B and 1C).PED was evaluated for presence or absence of any notch, type of reflectivity (Hyper, hypo, mixed) and for underlying pachyvessel. Presence of pachyvessel was also evaluated underlying the DLS along with the reflectivity of DLS (Hyper, hypo, mixed). In cases where pachyvessel was present in associated with either PED or DLS, the choroidal thickness was also measured in that location (Figure 1C).
The sections were also evaluated for presence or absence of intraretinal fluid (IRF) and subretinal fluid (SRF). In eyes with presence of SRF, the maximum vertical extent was measuredmanually (Figure 1A). Additionally, in the section with maximum extent of PED, a detailed analysis was performed of the outer retinal layers. This included scrutinizing the integrity of the retinal pigment epithelium (RPE)(Figure 1D), ellipsoid layer (EZ) and external limiting membrane (ELM), and looking for presence of intraretinalhyperreflective dots, disorganization of outer retinal layers (DRIL) and vitreomacular interface abnormalities (VMIA). DRIL was considered to be present when it affected more than 50% of central 1mm zone. VMIA included epiretinal membranes (ERM) and vitreomacular traction (VMT).
Baseline ICGA was analysed for features such as dilated choroidal vessels, nodular hypercyanescence, abnormal vascular network, blocked cyanescence and mid-phase hypercyanescence. Furthermore, DFA was examined for various types of hyperfluorescence and hypofluorescence along with features of occult and classic CNVM
Intravitreal Injection
Ziv-aflibercept is available in vials of 100 mg / 4 ml (1.25 mg / 0.05 ml). Injection ziv-aflibercept is stored under recommended conditions and details are checked prior to aliquoting. Aliquotingis performed by a vitreo-retinal fellow under all aseptic precautions using a single 26-G needle prick technique, whereby only the syringes are changed leaving the needle in its place. 0.05 ml of ziv-aflibercept is aliquoted in tuberculin syringe, placed in a sterile cloth and then stored in a sterile tray which is kept in a refrigerator under 2º C -8º C.
All intravitreal injections are performed in an OT complex. With the patient in supine position, the eye is confirmed by fundus examination followed by administered subconjunctivalanesthesia(0.5 mL of 2% lignocaine) in inferotemporal quadrant. 5% povidine iodine is instilled allowing a five-minute contact period. Subsequently, 0.05 ml of IVZ is given in the inferotemporal quadrantat 3.5 mm away from the limbus with a 30-gauge needle under all aseptic precautions. The eye was then patched after instilling 5% povidine iodine drops and moxifloxacin ointment for 4 hours. After the injection, topical moxifloxacin is prescribed for a period of 14 days.
Changes in BCVA, IRF, SRF, SFCT, dimensions of PED and DLS were analysed at baseline & at 1 month. Alternation in integrity of outer retinal layers (RPE, EZ, ELM), DRIL and VMIA was also evaluated at end of 1 month.Statistical analysis was done using the SPSS software, version 16.0 and statistical significance was set at p value of 0.05.
RESULTS
The mean age of the study population was 69 ±12.04 years of which 77.78 % (7 patients) were men and 22.22 % (2 patients) were women.
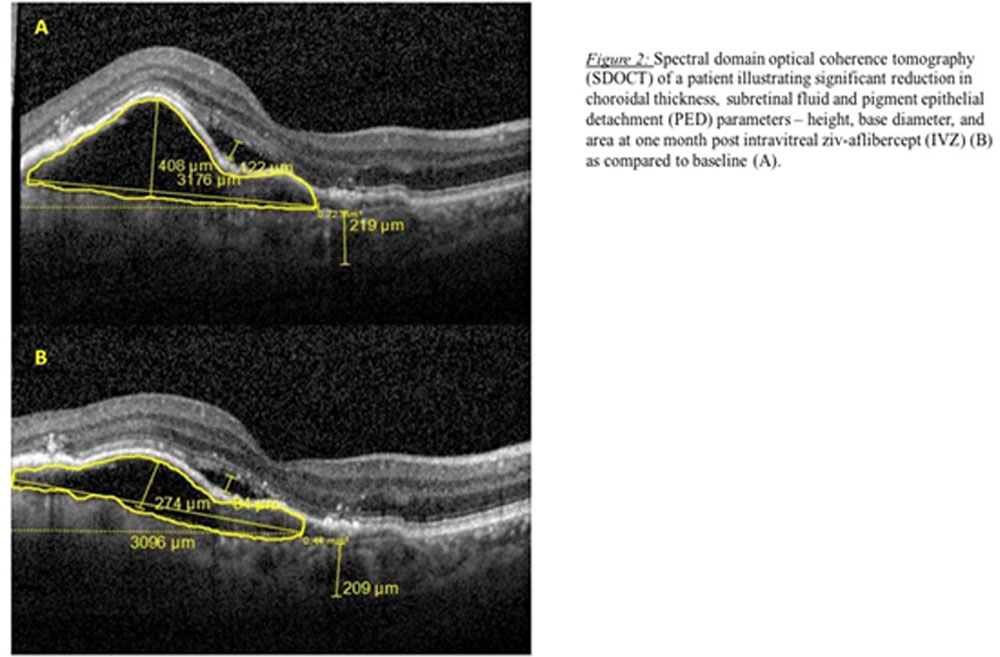
Compared with baseline, statistically significant reduction was noted in height, base diameter & area of PED respectively (p=0.02, p=0.01, p=0.02) at one month(Table 1) (Figure 2A). Five eyes each showed presence of notched PED and associated pachyvessel with PED. There was no significant difference in CT at level of pachyvessel at end of one month (p = 0.07) (Table 1).Six eyes had mixed PED reflectivity while hyperreflectivity and hyporeflectivity was present in two eyes each. In one eye, the PED reflectivity changed from hyper to mixed type post IVZ with early RPE regeneration.
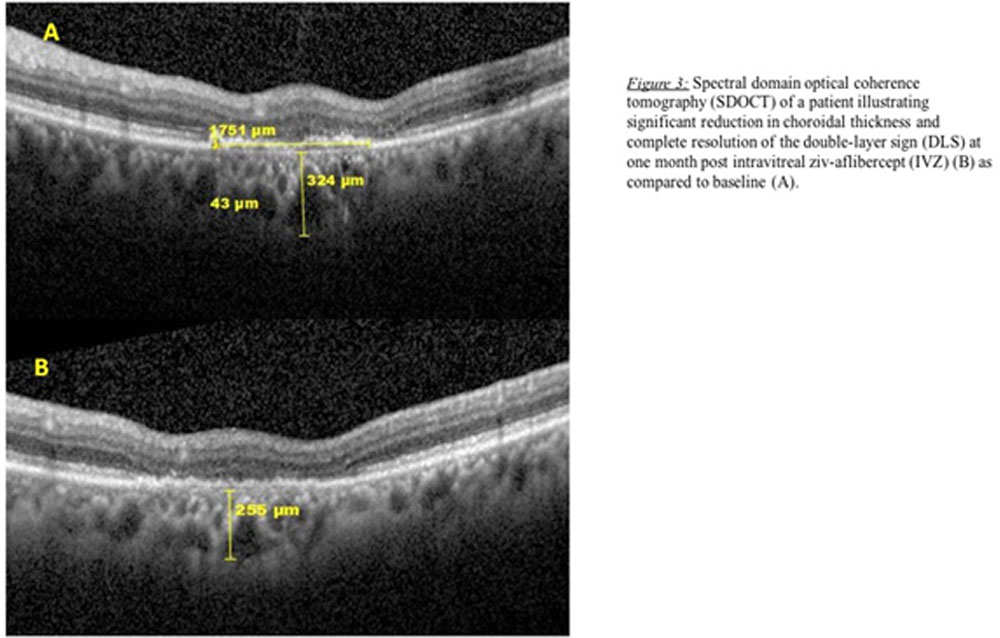
DLS was present in 8 eyes with hyporeflectivity seen more frequently (6/8 eyes) than hyperreflectivity (2/8 eyes). All 8 eyes hadpachyvessel associated with the DLS. No significant change in CT was noticed at level of pachyvessel (p = 0.08) (Table 1). Statistically significant reduction was noted in the height of the DLS (p = 0.01) whereas the width did not change significantly (p = 0.12) (Table 1). One eye demonstrated complete resolution of the DLS (Figure 3).
Complete resolution of IRF and SRF was seen in 40% and 37.5% of eyesrespectively. SRF height also showed significant reduction (p = 0.01) (Table 1). SFCT was significantly reduced at the end of one month (p=0.0009) (Table 1) (Figure 4A and B). The eyes also showed an improvement in BCVAand CMT, although it was not statistically significant (Table 1).
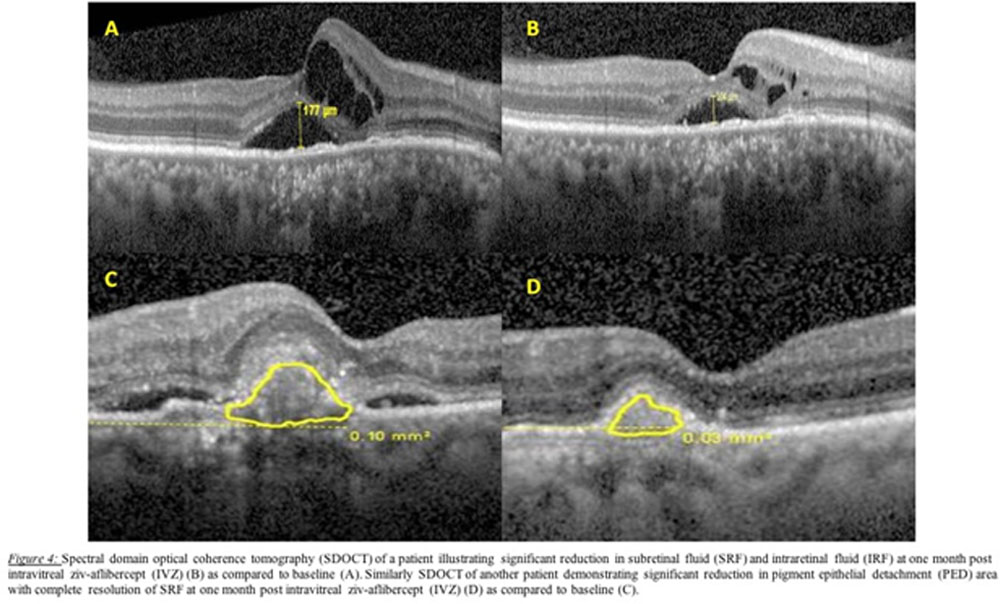
Table 1: Changes in BCVA and SD-OCT parameters at baseline and one month post intravitrealziv-aflibercept
| Parameter | Baseline | 1 Month post-IVZ | p-value |
| BCVA | 0.48 ± 0.297 | 0.46 ± 0.327 | 0.73 |
| SFCT | 215.7 ± 130.09 µm | 201.6 ± 129.93 µm | 0.009 |
| CMT | 365.2 ± 103.9 µm | 317.7 ± 87.24 µm | 0.11 |
| PED Base Diameter | 1884.9 ± 1433.02 µm | 1753.7 ± 1431.08 µm | 0.02 |
| PED Height | 344.8 ± 274.95 µm | 272 ± 217.88 µm | 0.01 |
| PED Area | 0.57 ± 0.63 mm2 | 0.44 ± 0.49 mm2 | 0.02 |
| CT at pachyvessel associated with PED | 132.9 ± 168.53 µm | 118.8 ± 148.97 µm | 0.07 |
| DLS Height | 35.5 ± 20.88 µm | 23.40 ± 22.54 µm | 0.01 |
| DLS Width | 996 ± 716.05 µm | 702 ± 773.92 µm | 0.12 |
| Choroidal Thickness at DLS | 226.5 ± 145.07 µm | 203 ± 134 µm | 0.08 |
| SRF Height | 104.2 ± 67.53 | 41.9 ± 49.1 | 0.01 |
IVZ: Intravitrealziv-aflibercept; BCVA: Best corrected visual acuity; SFCT: Subfovealchoroidal thickness; CMT: Central macular thickness; PED: Pigment epithelial detachment; CT: Choroidal thickness; DLS: Double layer sign; SRF: Subretinal fluid
On detailed analysis, at baseline, RPE rip was present in 7 eyes which showed early resolution in 2 eyes (Table 2) (Figure 5). Similarly, ELM disruption showed improvement in 4 out of the 9 eyes (Figure 6) while ellipsoid disruption did not show any signs of restoration at one month in all 10 eyes (Table 2). Likewise, DRIL improved in 1 out of the 5 eyes (Figure 6) while reduction in hyperreflective dots was seen in 7 out of the 10 eyes (Table 2). One eye has ERM which remained unchanged (Table 2). None of the patients experienced any serious ocular or systemic adverse events.
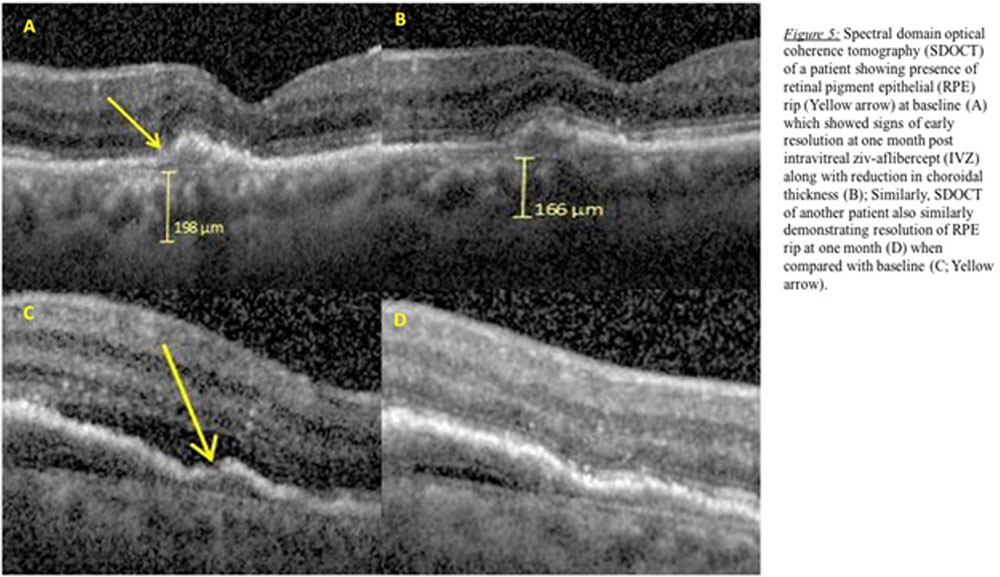
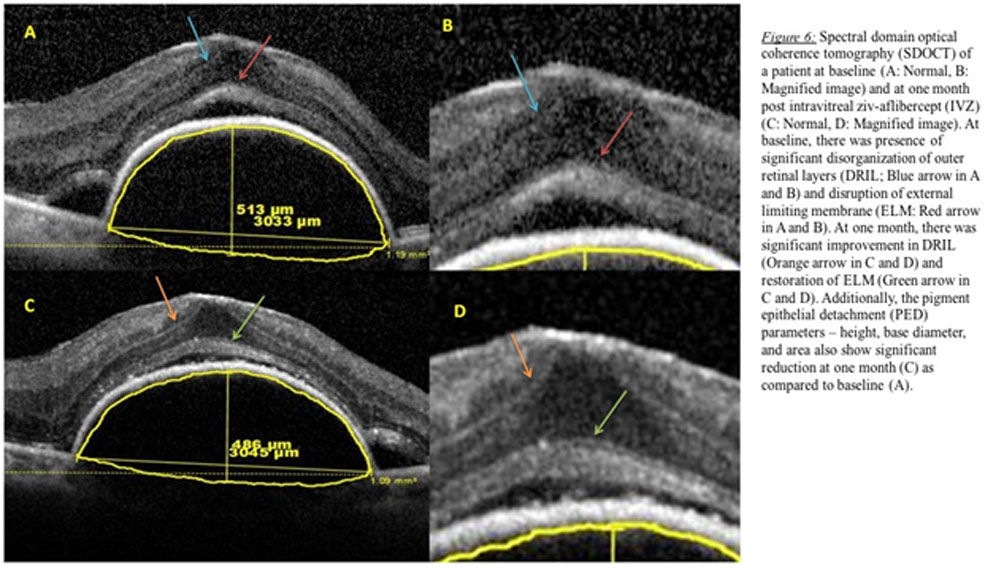
Table 2: Changes in micromorphic parameters on SD-OCT at baseline and one month post intravitrealziv-aflibercept
| Parameter | Baseline (number of eyes) | Resolution one month post-IVZ (number of eyes) |
| RPE Rip | 7 | 2 |
| EZ Disruption | 10 | 0 |
| ELM Disruption | 9 | 4 |
| DRIL | 5 | 1 |
| Hyperreflective IR dots | 10 | 7 (reduced) |
| VMIA | 1 (ERM) | 0 |
IVZ: Intravitrealziv-aflibercept; RPE: Retinal pigment epithelium; EZ: Ellipsoid disruption; ELM: External limiting membrane; DRIL: Disorganization of outer retinal layers; IR: Intraretinal; VMIA: Vitreo-macular interface abnormalities; ERM: Epiretinal membrane
DISCUSSION
In the past decade, anti-VEGF agents have become the standard of care for various chorio-retinal disorders. Amongst the various choices available, aflibercept is considered the first line agent based on results of multiple landmark trials.5, 10, 11 Nonetheless, the cost of aflibercept remains a major deterrent to its widespread use in developing nations. Ziv-aflibercept is a biosimilar to aflibercept, but has a different buffer solution and undergoes a different purification process.12 Being an economical option, over the past few years, ziv-aflibercept has been successfully used for management of various chorioretinal disorders such as wet AMD, PCV, and DME and so on.8, 9, 13, 14 However, its use in PCN and chronic CSCR has not yet been described in literature. PCN is a recently described disease entity belonging to the pachychoroid disease spectrum. Its management is still evolving, but being primarily a choroidal neovascularization disease, the management involves administration of intravitreal anti-VEGF therapy.15 In our series, we describe the use of IVZ in PCN and CCSCR for the first time in literature.
To begin with, there were few concerns regarding the use of ziv-aflibercept due to osmolarity issues. Studies evaluating the safety profile of intravitreal injections have demonstrated that osmolarity of <500 mOsm does not have any adverse effect on the RPE.16 So, although ziv-aflibercept has an osmolarity of 1045mOsm, its effective intravitreal osmolarity is only 312 mOsm since it is injected in about 4ml of vitreous cavity. Also, animal studies on ziv-aflibercept did not reveal any significant increase in its plasma levels after intravitreal administration.17 Hence, ziv-aflibercept can be considered to be safe for intravitreal therapy, which has been corroborated by various studies. In the current series, we did not find any serious systemic adverse event.
In a retrospective review of 16 eyes of patients with non-responsive AMD switched to IVZ, Braimah et al did not find any significant improvement in BCVA, CMT, PED height and presence of IRF and SRF between baseline and 12 months.18In contrast, in our study, we found significant improvement in morphometric parameters in relation to the PED, including reduction in height, base diameter and area. Improvement in PED height and volume has been demonstrated after intravitreal aflibercept treatment by Chan et al at end of 6 months.19 Even de Massougnes S et al have shown improvement in PED height after aflibercept therapy at end of 1 year.20Improvement in PED parameters as demonstrated in our study has been seen after aflibercept use, but not yet been described after IVZ therapy in literature. Additionally, in the current study, even the DLS, which in itself is a shallow irregular PED, showed significant reduction in height, although not in the base diameter. One eye even exhibited complete resolution of DLS within one month of IVZ. Changes in DLS after IV anti-VEGF therapy has not yet been studied. Improvement in the PED parameters is a crucial outcome after single dose of IVZ since it is one of the most resistant parameter to anti-VEGF therapy and an important cause of persistent disease activity or frequent recurrences.
Mansoor et al reported significant improvement in BCVA and CMT at 1 month and 3 months post IVZ for wet AMD.21 In contrast, Braimah et al did not find any significant improvement in BCVA and CMT at end of 12 months for refractory AMD.18 Similarly, in our series, although we noted improvement in BCVA and CMT, it was not significant. Nonetheless, we noted significant reduction in SRF height and SFCT. 40% and 37.5% of eyes had complete resolution of IRF and SRF respectively. Reduction in choroidal thickness is a vital finding of our study since 7of the 10 eyes belonged to the pachychoroid disease spectrum (PCV : 3 eyes, chronic CSCR : 2 eyes and PCN : 2 eyes). Although this pilot study evaluates only one month outcomes, the results are very encouraging to warrant the use of IVZ in this emerging group of disease entity, namely pachychoroid disorder.
In this study, we performed a comprehensive evaluation of individual retinal layers. RPE rip was seen in 7 eyes at baseline which showed signs of early resolution in 2 of them at the end of one month. Similarly, ELM disruption showed improvement in 4 out of the 9 eyes while ellipsoid disruption did not show any signs of restoration at one month in all 10 eyes. Likewise, DRIL improved in 1 out of the 5 eyes while reduction in hyperreflective dots was seen in 7 out of the 10 eyes. One eye has ERM which remained unchanged. These micromorphic changes are very critical in visual prognosis. Although we did not find any notable change in BCVA, the results are too short term to assess the visual outcomes effects secondary to restoration of these retinal layers. Nonetheless, the beneficial effect of IVZ on retinal layers can be postulated to have favourable long-term outcomes.
The strength of our study includes evaluation of an emerging cost-effective anti-VEGF agent, namely, intravitrealziv-aflibercept, in wet AMD and pachychoroid disease spectrum. We also evaluated the hitherto unstudied effect of IVZ on CCSCR and PCN. Moreover, it is a singular study to perform a detailed qualitative and quantitative assessment of IVZ on various morphological features on multimodal imaging, whereby we illustrate promising anatomical outcomes.
The limitations of our current study include the limited sample size, inclusion of patients with multiple aetiologies and short-term study. Additionally, we could not perform subgroup analysis of effect of IVZ on individual disease entity due to small sample size. However, the favourableshort-term morphometric and safety outcomes is indicative of similar potentially encouraging outcomes with long-term studies and larger sample size.
In conclusion, our study demonstrates that off-label use of single dose of intravitrealziv-aflibercept has promising retinal and choroidal morphological outcomes on multimodal imaging, besides maintaining stable visual acuity with an acceptable safety profile. Additionally, its low-cost favours its use as an efficacious anti-VEGF agent in the developing world.
References
- Rofagha S, Bhisitkul RB, Boyer DS, et al. Seven-year outcomes in ranibizumab-treated patients in ANCHOR, MARINA, and HORIZON: a multicenter cohort study (SEVEN-UP). Ophthalmology 2013;120:2292–2299.
- Koh A, Lee WK, Chen LJ, et al. EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina (Philadelphia, Pa) 2012;32:1453–64.
- Macugen Diabetic Retinopathy Study Group. A phase II randomized double-masked trial of pegaptanib, an anti-vascular endothelial growth factor aptamer, for diabetic macular edema. Ophthalmology 2005;112:1747–1757.
- Nguyen QD, Brown DM, Marcus DM, et al; RISE and RIDE Research Group. Ranibizumab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology 2012;119:789–801.
- Do DV, Schmidt-Erfurth U, Gonzalez VH, et al. The DA VINCI study: phase 2 primary results of VEGF Trap-Eye in patients with diabetic macular edema. Ophthalmology 2011; 118:1819–1826.
- Available at: https://www.asrs.org/pat-survey/pat-survey-archive. Accessed July 6, 2015.
- Patel A, Sun W. Ziv-aflibercept in metastatic colorectal cancer. Biologics 2014;8:13–25.
- Mansour AM, Al-Ghadban SI, Yunis MH, et al. Ziv-aflibercept in macular disease. Br J Ophthalmol 2015; 99:1055–1059.
- Chhablani J, Narayanan R, Stewart MS, et al. Short-term safety of intravitrealziv-aflibercept in age-related macular degeneration. Retina 2015.
- Schmid MK, Bachmann LM, Fas L, et al. Efficacy and adverse events of aflibercept, ranibizumab and bevacizumab in age-related macular degeneration: a trade-off analysis. Br J Ophthalmol 2015;99:141–6.
- Schmidt-Erfurth U, Kaiser PK, Korobelnik JF, et al. Intravitreal aflibercept injection for neovascular age-related macular degeneration: ninety-six-week results of the VIEW studies. Ophthalmology 2014;121:193–201.
- Trichonas G, Kaiser PK. Aflibercept for the treatment of agerelated macular degeneration. OphthalmolTher 2013;2:89–98.
- de Oliveira Dias JR, Xavier CO, Maia A, de Moraes NS, Meyer C, Farah ME, Rodrigues EB.Intravitreal injection of ziv-aflibercept in patient with refractory age-related macular degeneration.Ophthalmic Surg Lasers Imaging Retina. 2015 Jan;46(1):91-4.
- Videkar C, Kapoor A, Chhablani J, Narayanan R.Ziv-aflibercept: a novel option for the treatment of polypoidal choroidal vasculopathy.BMJ Case Rep. 2015 Dec 18;2015.
- Pang CE, Freund KB.Pachychoroidneovasculopathy.Retina. 2015 Jan;35(1):1-9.
- Marmor MF, Martin LJ, Tharpe S. Osmotically induced retinal detachment in the rabbit and primate. Electron miscoscopy of the pigment epithelium. Invest Ophthalmol Vis Sci 1980;19:1016–29.
- de Oliveira Dias JR, Badaró E, Novais EA. Preclinical investigations of intravitrealziv-aflibercept. Ophthalmic Surg Lasers Imaging Retina 2014;45:577–84.
- Braimah IZ, Agarwal K, Mansour A, Chhablani J; Ziv-aflibercept Study Group.One-year outcome of intravitrealziv-aflibercept therapy for non-responsive neovascular age-related macular degeneration.Br J Ophthalmol. 2017 Jun 8.
- Chan CK, Jain A, Sadda S, Varshney N.Optical coherence tomographic and visual results at six months after transitioning to aflibercept for patients on prior ranibizumab or bevacizumab treatment for exudative age-related macular degeneration (an American Ophthalmological Society thesis).Trans Am Ophthalmol Soc. 2014 Jul;112:160-98.
- de Massougnes S, Dirani A, Mantel I.Good visual outcome at 1 year in neovascular age-related macular degeneration with pigment epithelium detachment: Factors Influencing the Treatment Response.Retina. 2017 Mar 30.
- Mansour AM, Chhablani J, Antonios RS, Yogi R, Younis MH, Dakroub R, Chahine H.Three-month outcome of ziv-aflibercept for exudative age-related macular degeneration.Br J Ophthalmol. 2016 Dec;100(12):1629-1633.
Leave a Comment