
![]()
Dr. Sneha Batra, Dr. Partha Biswas, Dr. Ajoy Paul, Dr. Preeyam Biswas
Abstract :
Purpose:
To evaluate visual, refractive outcomes and patient satisfaction following bilateral trifocal intraocular lens implantation after cataract surgery.
Methods:
Fifty six eyes of 28 patients that were operated in a tertiary eye care centre in Kolkata followed by implantation of trifocal intraocular lens, included in the study. A complete ophthalmic examination was performed preoperatively and postoperatively. The uncorrected and best distance-corrected monocular and binocular, near, intermediate, and distance visual acuities were measured 6 months postoperatively. In addition to the standard clinical follow-up, a questionnaire evaluating individual satisfaction and quality of life was submitted to the patients.
Results:
The mean age of patients at the time of surgery was 65 ± 10 years. 90% of eyes showed a spherical equivalent within ±0.50 diopters 6 months after surgery. All patients had a binocular uncorrected distance visual acuity of 0.00 LogMAR or better and a binocular uncorrected intermediate visual acuity of 0.10 LogMAR or better, 6 months after surgery. Furthermore, 80% of patients achieved a binocular uncorrected near visual acuity of 0.10 LogMAR or better. Patient satisfaction was high regarding visual quality.
Conclusions:
Trifocal IOL implantation provides excellent outcomes of visual function for far, intermediate, and near distances, providing high levels of visual quality and patient satisfaction. The use of 3 foci provided significant intermediate visual results without compromising near or distance vision.
FULLTEXT:
INTRODUCTION:
Spectacle independence is the great challenge of modern cataract surgery. Multifocal lenses remain one of the best solution to achieve spectacle independence after cataract surgery. The optical function of the refractive multifocal IOLs derives from the refractive zones for distance and near vision allocated concentrically over the optic lens. The main disadvantage of this lens type is the significant pupil-dependence and the loss of energy in the transition zone.
Diffractive multifocal IOLs use a diffractive pattern to create an additional focus for near vision in the first diffraction order. Although part of the incident light is intrinsically lost at higher orders of diffraction, studies have shown that the IOL offers good distance and near visual acuity (VA).1
Diffractive IOLs achieve better optical quality, based on optical bench measurements, than refractive multifocal IOLs.2-3Publications presenting results from clinical studies indicate better contrast sensitivity after diffractive IOL implantation than for refractive multifocal IOL implantation for equivalent visual acuities.3
However, most studies also report poor scores for intermediate vision, correlating to worse intermediate visual acuity.4-5It has also been reported that the implantation of bifocal diffractive IOLs leads to a higher percentage of spectacle-dependent patients, especially for intermediate distance vision.5
Hence, the quality of vision with multifocal IOLs is a real concern. In many cases, photic phenomena (glare, halos, positive or negative dysphotopsia) are described after multifocal lens implantation which result in blurred vision.6Multifocal IOLs do not cover the full range of vision and often have insufficient intermediate vision.7-9
Our purpose of the study was to evaluate visual, refractive outcomes and patient satisfaction following bilateral trifocal intraocular lens implantation after cataract surgery.
Methods:
Thisretrospective study comprises 56 eyes in 28 consecutive patients who had cataract surgery followed by bilateral implantation of the trifocal IOL between April 2016 and March 2017 at a tertiary eye hospital in Kolkata. The guidelines of the Helsinki Declarations were followed, and informed consent was obtained from all patients.
Trifocal intraocular lens combines two diffractive patterns, one adding +3.50 diopters (D) for the near vision and the other one +1.75D for the intermediate vision. An asymmetric distribution of energy among the three foci (near, intermediate, and far) allows for dominant distance vision, improved intermediate vision, and no impacted near vision. The IOL is based on a fully diffractive optic with gradual attenuation of the diffractive step height throughout the entire optic, resulting in a continuous change of the light energy distribution directed to the three primary foci. The percentage of lost energy for typical bifocal diffractive IOLs is 18%–20%, while it is approximately 15% for the trifocal IOL. This is due to accumulation of the energy from the second order of the diffractive pattern for the intermediate vision (+1.75 D) to the energy from the first order of the diffractive pattern for the near vision (+3.50 D).10
Detailed preoperative examination was done. VA was measured using a Snellen chart, intraocular pressure using a Goldmann tonometer, axial length and keratometric values using the IOLMaster 500 (Carl Zeiss Meditec, Jena, Germany). A slit lamp examination of the anterior segment and an indirect ophthalmoscopy were performed. Exclusion criteria was diabetic retinopathy, age-related macular degeneration, cornea guttata, or pseudoexfoliative syndrome, corneal astigmatisms greater than 1.75 D. The patient’s expectations regarding spectacle independence and visual quality were also assessed and explained.
One surgeon performed the surgeries using a standard bimanual phaco-chop technique of sutureless microincision, phacoemulsification, and topical anesthesia. Postoperative topical therapy included a combination of topical antibiotic and steroidal agents.The patients were examined at first postoperative day, then 1 week, 1 month, 3 months and 6 months after surgery. In every visit, detailed anterior and posterior segment evaluation done along with intraocular pressure. Uncorrected and corrected visual acuity was measured at near 33 CM, Intermediate at 67 cm, 100 cm and distance using snellen visual acuity chart, then converted to LogMar chart. All measurements were done in same room both preoperatively and postoperatively – usually at both mesopic and photophic condition.
The contrast sensitivity test was performed under same room light preoperatively and postoperatively using Pelli Robson Contrast Sensitivity Chart. The patients were surveyed using a quality of life questionnaire.
The results are presented as the mean ± standard deviation (SD) and were calculated using Excel worksheet 2007 software and statistically analyzed using SPSS Version 22. Differences were considered statistically significant when the P-value was less than 0.05.
RESULTS:
The mean age of patients at the time of surgery was 65 ± 10 years. 90% of eyes showed a spherical equivalent within ±0.50 diopters 6 months after surgery. Mean binocular uncorrected distance visual acuity of LogMAR 0.05±05 or better and a binocular uncorrected intermediate visual acuity of LogMAR 0.1±0.05 or better, 6 months after surgery. Furthermore, 80% of patients achieved a binocular uncorrected near visual acuity of LogMAR0.1±0.05( Fig- 1)
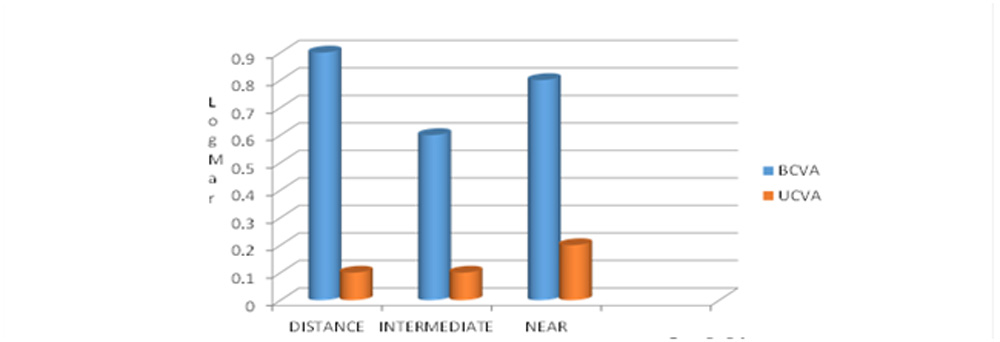
Fig-1: Best corrected visual acuity and Uncorrected visual acuity
Mean Log Mar contrast sensitivity was improved upto LogCS 1.95( Range 1.35 – 2.25 ).Fig – 2 ). Patient satisfaction was high regarding visual quality.
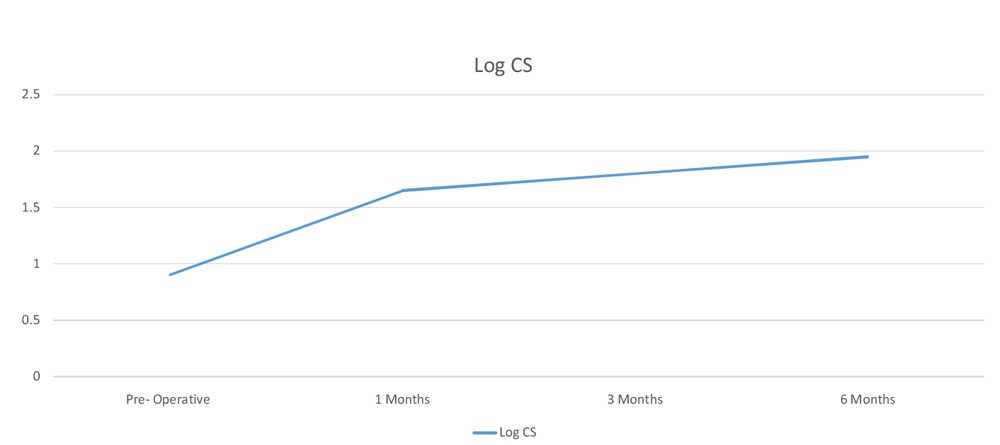
Fig -2 : Preoperative and Postoperative Contrast sensitivity in LogMar Scale
A summary of the questionnaire answers regarding the photic phenomena is given in Figure 3. 18% percent of the patients reported spontaneously seeing halos, 8% on inquiry, but halos were not seen by 74 % of the patients. Nevertheless, the halos were not considered to be bothersome.

Fig – 3: Status of Patient satisfaction with trifocal implantation after cataract surgery
The quality of vision was then assessed with respect to the preoperative condition. The quality of vision was estimated to be good for watching TV and book reading in 100% of cases and was good for needle work in 85% of cases. Spectacle independence was achieved for 90% of eyes for distance vision and for 85% for near vision. In the 15% of the patients requiring spectacles for near vision, half of them only needed their spectacles for very small characters.
Discussion:
The optical principles of the multifocal IOL are very different from the trifocal IOL; the former being made of concentric diffractive zones allocated to near, intermediate, and distance visions, combining diffractive and refractive IOL principles.3 The purpose of this study was to analyze the objective and subjective outcomes after the implantation of a diffractive trifocal IOL, and to compare the clinical findings with the theoretical findings in previous literatures.
The outcomes with the trifocal IOL are good for intermediate and near vision, and are similar to the outcomes of several studies on the implantation of multifocal IOLs that have been reported in a recent article from de Vries et al.8 Furthermore, the distance and near visual acuities are maintained with the trifocal IOL while enhancing the intermediate visual acuity.
Optimum VA outcomes are confirmed by the percentage of spectacle independence, which is comparable with any of those reported in other studies.11 Spectacle independence is achieved for 90% of eyes for distance vision and for 85% for near vision with the trifocal IOL. In the 15% of the patients requiring spectacles for near vision, half this number need them for very small characters only.
Multiple studies show compromised contrast sensitivity in multifocal IOL implantation. This also increase glare and halos in dim light condition.12 Our study shows mean log contrast sensitivity is LogCS 1.95 with minimum glare and halos. Patients also shows high level of satisfaction in their questionnaire.
The study by de Vries13 et al showed that 38.2% of patients were dissatisfied after implantation of a multifocal IOL because they experienced major photic phenomena, with or without blurred vision. There is an important discrepancy between the reported rates of subjective photic phenomena.14This discrepancy could be due to the explanations given to the patient by the surgeon to describe photic phenomena. Glare can be translated as sensitivity to light (dazzle) or as the sensation of a white veil in front of the actual image. Halos can also be explained in two ways: dazzle with light or rings around lights.
The trifocality does not appear to introduce any additional problems to those reported for diffractive bifocal MIOLs. This may be explained by the number of diffractive steps (26 steps) used in the FineVision IOL, which is lower than that for other diffractive IOLs (32 for the Tecnis and 28 for the Acrilisa), thus reducing the halos induced by the diffractive edges.13 In addition, FineVision shows convoluted diffractive steps, ie, with smoothed edges. Halos are therefore attenuated compared to more or less convoluted IOLs with sharp diffractive steps.
Conclusion:
Trifocal IOL implantation provides excellent outcomes of visual function for far, intermediate, and near distances, providing high levels of visual quality and patient satisfaction. The use of 3 foci provided significant intermediate visual results without compromising near or distance vision and thus good spectacle independence. The trifocal diffractive IOL induces minimal photic phenomena (halos, glare). The contrast sensitivity did not decrease as other multifocal IOL and provides excellent patient satisfaction.
Reference:
- Mesci C, Erbil H, Ozdoker L, Karakurt Y, Bilge AD. Visual acuity and contrast sensitivity function after accommodative and multifocal intraocular lens implantation. Eur J Ophthalmol. 2010;20(1): 90–100.
- Maxwell WA, Lane SS, Zhou F. Performance of presbyopia-correcting intraocular lenses in distance optical bench tests. J Cataract Refract Surg. 2009;35(1):166–171.
- Mesci C, Erbil HH, Olgun A, Aydin N, Candemir B, Akçakaya AA. Differences in contrast sensitivity between monofocal, multifocal and accommodating intraocular lenses: long-term results. Clin Experiment Ophthalmol. 2010;38(8):768–777.
- Cochener B, Lafuma A, Khoshnood B, Courouve L, BerdeauxG.Comparison of outcomes with multifocal intraocular lenses: a meta-analysis. ClinOphthalmol. 2011;5:45–56.
- Petermeier K, Messias A, Gekeler F, Szurman P. Effect of +3.00 diopter and +4.00 diopter additions in multifocal intraocular lenses on defocus profiles, patient satisfaction, and contrast sensitivity. J Cataract Refract Surg. 2011;37(4):720–726.
- Voskresenskaya A, Pozdeyeva N, Pashtaev N, Batkov Y, TreushnicovV,Cherednik V. Initial results of trifocal diffractive IOL implantation. Graefes Arch ClinExpOphthalmol. 2010;248(9):1299–1306.
- Sood P, Woodward MA. Patient acceptability of the Tecnis multifocal intraocular lens. ClinOphthalmol. 2011;5:403–410.
- de Vries NE, Webers CA, Touwslager WR, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859–865.
- de Vries NE, Webers CA, Montés-Micó R, Ferrer-Blasco T, Nuijts RM. Visual outcomes after cataract surgery with implantation of a +3.00 D or +4.00 D aspheric diffractive multifocal intraocular lens: Comparative study. J Cataract Refract Surg. 2010;36(8):1316–1322.
- Gatinel D, Pagnoulle C, Houbrechts Y, Gobin L. Design and qualification of a diffractive trifocal optical profile for intraocular lenses. J Cataract Refract Surg. 2011;37(11):2060–2067.
- Alió JL, Agdeppa MC, Pongo VC, El Kady B. Microincision cataract surgery with toric intraocular lens implantation for correcting moderate and high astigmatism: pilot study. J Cataract Refract Surg. 2010; 36(1):44–52.
- Lesieur G. [Outcomes after implantation of a trifocal diffractive IOL.] J FrOphtalmol. 2012;35(5):338–342. French [with English abstract].
- deVries NE, Nuijts RM. Multifocal intraocular lenses in cataract surgery: literature review of benefits and side effects. J Cataract Refract Surg. 2013;39(2):268–278.
- Cochener B, Vryghem JC, Rozot P, et al. Visual and refractive outcomes after implantation of a fully diffractive trifocal lens. ClinOphthalmoly, 2012;6:142.
Leave a Comment