
Dr. Sanket Bhatnagar, B16754, Dr. Shruti Kochar Maru, Dr. Rohit Shetty
Introduction:
Research on refractive solutions for presbyopia is essential as a large population in the world suffer from vision impairments associated with increasing longevity. Many structural and physiological changes occur in the eye with the onset of presbyopia including the decrease in amplitude of accommodation.1 Population based surveys have shown that 1.04 billion people in the world are in presbyopic age and about 517 million people do not have adequate corrective measures for the same. 2 Vision impairment from uncorrected presbyopia and low spectacle coverage predominantly exists in the developing nations like India.3
At present various static and dynamic techniques, have been attempted to give presbyopes good vision at near, intermediate and far viewing distances. However, no single method is accurate and completely reliable which can guarantee long term correction. Methods for alleviation of visual challenges in presbyopia include fixed and variable focal lens system, modification of optics of cornea, replacement of crystalline lens or partial restoration of active accommodation.4 An emerging option to aid in near and intermediate vision is to increase in depth of focus which can be obtained by induction of negative spherical aberration (SA). 5 Adaptive optics (AO) technology may find a clinical interest in demonstrating the effect of aberration modification on depth of focus.
At the advent of laser refractive surgery, the US Food and Drug Administration (FDA), included diabetes mellitus as a relative contraindication, and uncontrolled diabetes mellitus as an absolute contraindication for laser refractive surgery. There were however limited studies at the time and the recommendations were based on the pre-existing data based on non-laser ocular surgery. Laser refractive surgery has evolved drastically, however, still there are concerns regarding visual outcomes.
Diabetics have been associated with reduced accommodative amplitude in the pre presbyopic age group and early onset of presbyopia.6 Despite increasing popularity of refractive laser correction for presbyopia, its efficacy in diabetics is still questionable. Using adaptive optics in visual simulation, it is now possible to understand the tolerance of diabetic patients to laser presbyopic correction with induction of spherical aberrations and increase in depth of focus.
The purpose of the current study was to evaluate distance, intermediate and near vision in presbyopic patients by modifying spherical aberration (SA) using a Hartmann-Shack aberrometer combined with an adaptive optics visual simulator (Adaptive Optics Vision Analyzer- model VAO). To our knowledge, this is the first study in which the optical properties of the diabetic eyes were modified to assess the effect of alteration of spherical aberrations on depth of focus in a clinical setting.
Materials and Methods:
This was a prospective study conducted in accordance with the principles of the Declaration of Helsinki and all participants gave written informed consent. For one arm of the study, 100 eyes of 100 healthy presbyopes were recruited from patients visiting the out-patient department over 6 months. Participants with corrected distance visual acuity of 6/9.5 or better (decimal visual acuity ≥ 0.63 or LogMAR ≥ 0.22), spherical correction less than ±4.00 dioptres (D) and astigmatism less than 2.00 D were included.
For the other arm, 31 eyes of 31 diabetic patients with clear ocular media, no diabetic retinopathy, no previous ocular surgery or LASER, age above 40 years, astigmatism lower than 2D, and monocular corrected distance visual acuity better than 6/9.5 were included. Exclusion criteria included the presence of progressive myopia, advanced keratoconus, active ocular disease, diabetic retinopathy, contact lens wear or any other ocular diagnosis that may alter the optical quality. All the subjects underwent complete ocular examination before the test.
Adaptive Optics Visual Simulator
After proper focus and alignment, measurement of ocular aberrations was obtained using the Adaptive Optics Vision Analyzer(VAO). It comprises a liquid crystal spatial light modulator and a wavefront sensor which enables the equipment to not only measure the wavefront aberrations but also modify them using wavefront corrector unlike other aberrometers. 7
We used depth of focus –SA protocol to quantify the impact of spherical aberration (SA) to extend the DOF of a presbyopic patient. It starts with a basic objective and subjective assessment of the patient’s optics and then continues with a series of VA measurements at far, intermediate and near distance for variable amounts of SA. The output is a plot that shows the variation of VA for the different tested optics at the three testing distances with the fixed contrast. The root mean square of higher order aberration (HOARMS) in microns for a selected pupil size of 4.5mm. The analysis was limited up to the 5th order to maintain clinical relevance.
While selecting the optimal negative spherical aberration, that has the best impact on near and intermediate and drop in Snellen’s acuity not more than one line was chosen.
Formula-
The optimal spherical aberration was converted to the spherical power using this mathematical formula for possible surgical modification.
Statistical analysis:
Statistical analyses were performed using MedCalc® statistical software Version 16.2 (MedCalc Software, Inc., Mariakerke, Belgium). The Shapiro-Wilk test checked normal distribution of continuous variables. All the analysed variables are presented as the mean ± standard error of mean, median [95% confidence interval of median]. Analysis of parametric variables was performed using ANOVA whereas that of non-parametric variables was performed by the Friedman test. The statistical significance was set at p values of <0.05.
Result:
In this study 100 eyes of healthy presbyopes, chosen as per a table of random numbers (48 male and 52 female), with mean age of 46 ± 6 years (range 40 to 66 years) were enrolled. The demographic and refractive measurements of healthy presbyopes for sphere(defocus), cylinder(astigmatism), RMS HOA and spherical aberration are summarized in table 1. The normality of distribution, mean with standard error of mean, median value with 95 % confidence interval and the standard deviation (SD) corresponding to each variable were assessed.The median value with 95% CI of sphere was -0.2 D [-0.5, 0], cylinder -0.3 D [-0.5, -0.25] and RMSHOA 0.16 µ [0.15, 0.17]. The mean baseline spherical aberration was 0.03 ± 0.004 µ.
Table 1: Median of all the variables in healthy and diabetic presbyopic eyes
| Median [95% CI] | ||
| Healthy Presbyopes (n=100) | Diabetic Presbyopes
(n=31) |
|
| Sphere (D) | -0.25 [-0.50, 0.00] | -0.15 [-0.26, 0.00] |
| Cylinder (D) | -0.32 [-0.50, -0.25] | -0.5 [-0.73, -0.32] |
| Axis (degrees) | 32 [9.45, 76.38] | 100 [87, 112.07] |
| HOARMS | 0.16 [0.15, 0.17] | 0.17 [0.15, 0.21] |
| SA | 0.03 [0.02, 0.04] | 0.01 [-0.02, 0.02] |
| VA at 40 cm | 0.32 [0.32, 0.40] | 0.8 [0.65, 0.90] |
| VA at 80 cm | 0.5 [0.50, 0.63] | 0.9 [0.70, 0.90] |
| VA at infinity | 0.9 [0.90, 1.00] | 0.9 [0.90, 1.00] |
| SA induced (µm) | 0.2 [0.20, 0.25] | 0.1 [0.10, 0.15] |
| Change in VA at 40 cm | 0.2 [0.20, 0.25] | 0.1 [0.00, 0.10] |
| Change in VA at 80 cm | 0.22 [0.20, 0.25] | 0.1 [0.00, 0.10] |
| Change in VA at infinity | -0.05 [-0.10, 0.00] | 0 [0.00, 0.00] |
CI = Confidence interval, D = Diopters, HOARMS= Root mean square of Higher order aberration,SA =Spherical aberration, VA = Visual Acuity
Figure 1 represents Box-and-Whisker plot where the middle line represents the median and central box represents the values from 25 to 75 percentiles. The points outside the line extending from the minimum to the maximum value implies outliers. For healthy presbyopes (n=100) the improvement in visual acuity (in decimals) is plotted for amount of induced spherical aberration, change in near (40 cm), intermediate (80 cm) and distant (infinity) acuity using repeated measures of analysis of variance (ANOVA).After inducing the optimal negative spherical aberration, 48 % subjects improved up to 0.2 decimal acuity and 42% subjects had improvement more than 0.2 for near acuity. For intermediate distance, 33% subjects improved by up to 0.2 decimal acuity and 50 % improved by more than 0.2. About 40% subjects retained or improved their baseline distant acuity. On performing Friedman test, the change in acuities for near and intermediate (after inducing optimal SA) are significantly different from acuity for distance (p<0.00001).
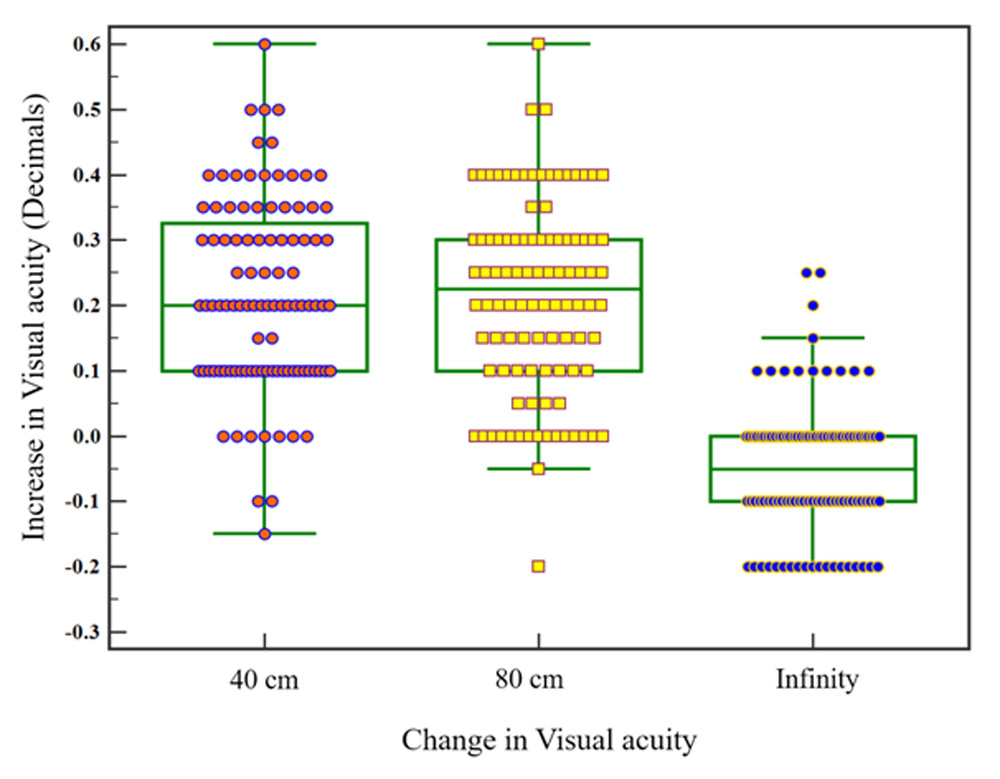
Figure 1: Improvement in visual acuity for presbyopes
In the second cohort of 31 eyes of diabetics, (4 female and 27 males) the mean age was 50 ± 6 years (range 40 to 62 years) and all the relevant parameters are summarized in table 1. The mean spherical power was -0.14 ± 0.09 D and mean SA was -0.002 ± 0.007 µ. The median value of cylinder was -0.62 D [-0.73, -0.32] and RMSHOA was 0.17 µ [0.15, 0.21].
Figure 2 represents box and whisker plot of diabetic presbyopes after introducing optimal spherical aberration. Majority of the patients had good baseline acuity to begin with and 45 % of them retained their baseline near vision and approximately 40 % patients retained their baseline intermediate vision. On the other hand, 50 % patients showed improvement in near and 60 % patients improvement in intermediate after negative SA induction. About 84% subjects retained or improved their baseline distant acuity. On performing Friedman test, the change in acuities for near and intermediate were significantly different from acuity for distance (p=0.00024).
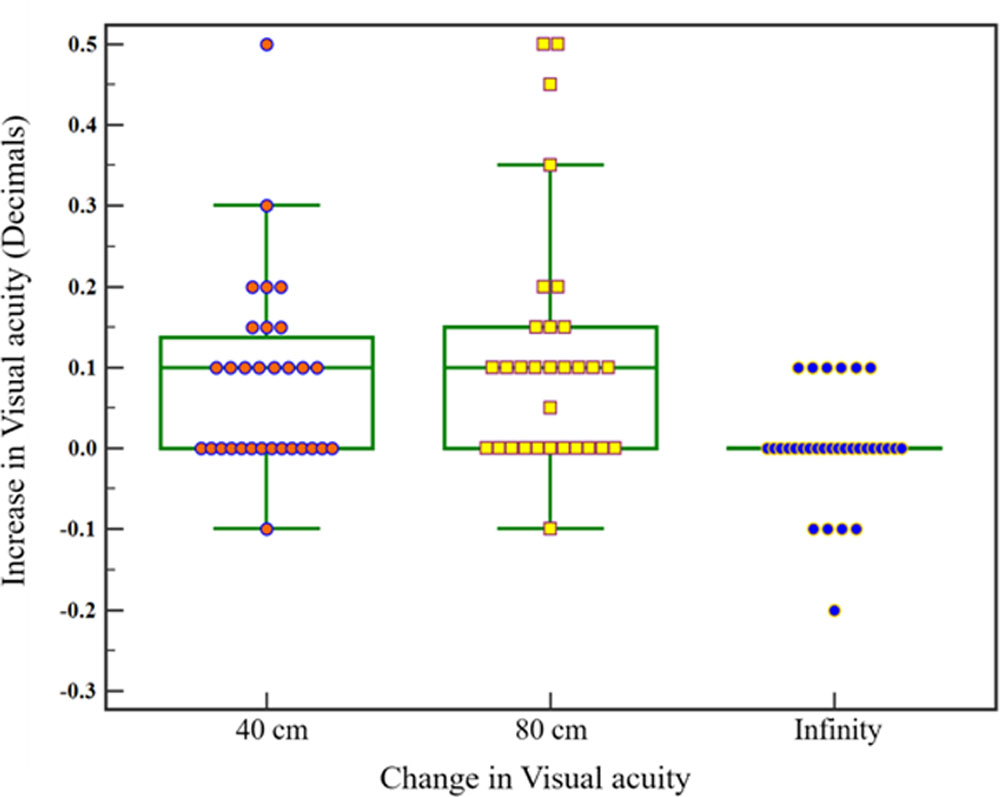
Figure 2: Improvement in visual acuity for diabetics
The optimal spherical aberration was converted to the spherical power and the two groups (healthy presbyopesvs diabetic presbyopes) were compared. Figure 3 shows the One-way Analysis of Variance between the groups and the difference is statistically significant (p=0.001). The duration of diabetes mellitus and amount of induced sphere did not correlate (r=0.1; p=0.71).
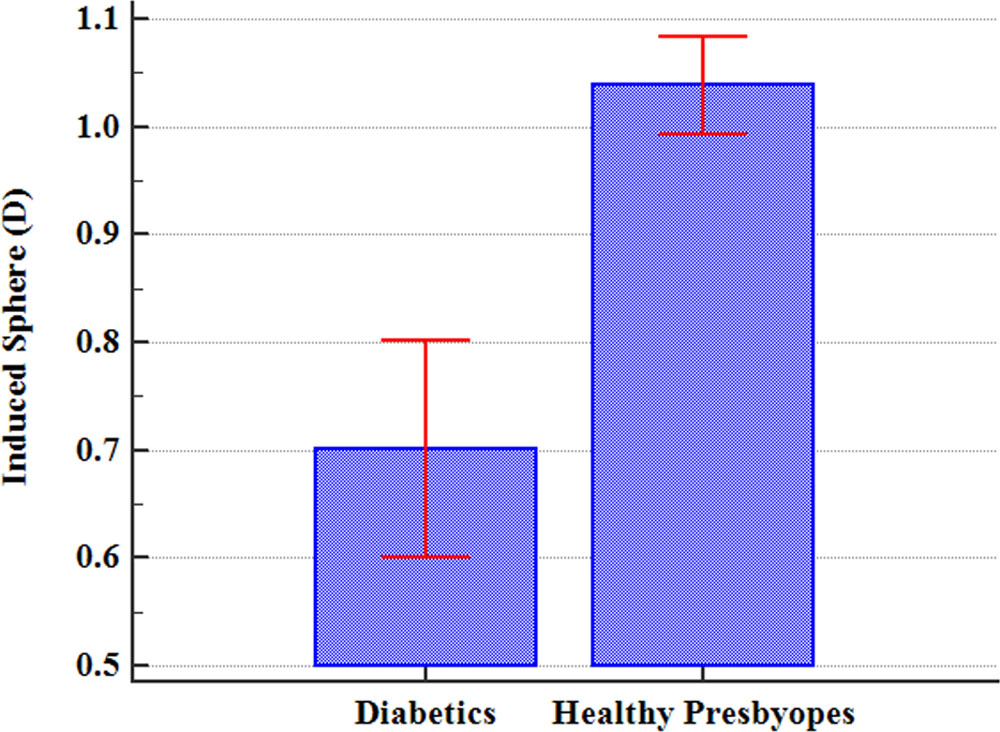
Figure 3: Comparison graph between diabetic and healthy presbyopes
Discussion:
Subjective amplitude of accommodation below 3 D can be considered as presbyopia and the amplitude falls to zero at the age of 52. 8,9 Depth of focus can be defined as the variation in image distance of a lens or an optical system which can be tolerated without incurring an objectionable lack of sharpness in focus.10 Negative spherical aberration induced by corneal laser ablation improves near and distance vision in presbyopic patients.11,12Nio et al., also showed that induction of spherical and irregular aberrations can increase the depth of focus using a theoretical eye model but not without decreasing the modulation transfer function at high spatial frequencies.13 Cheng et al. reported that a change in spherical aberration in a negative direction is linearly related to the amplitude of accommodation.14 The availability of devices like VAO with adaptive optics combined with Hartmann Shack technology has opened new avenues in bespoke optical corrections using wavefront-guided corneal surgery15, aberration-correcting contact lenses16, and wavefront-based custom intraocular lenses17.In a study conducted on the repeatability of the device we found that the intraclass correlation coefficient (ICC) for spherical aberration was 0.92 and 0.90 in normals and keratoconus subjects respectively.It is therefore a suitable tool to perform repeatable visual simulations. This indicates the precision of the VAO and these results are important refractive surgeons during refractive decisions.
Altered glycaemic levels have been associated with visual alterations due to hydration of the crystalline lens.18 Corneal ablation in diabetics has also been associated with variable outcomes and higher enhancement rates of nearly 28% 19, though the reason for the same is not clear. Other implications for refractive surgery in diabetics include a greater risk of epithelial ingrowth20 and worsening of diabetic retinopathy.21
We found in this study that different individuals differ in their tolerance to the induction of spherical aberrations, and there are some that may not accept them at all. The use of an adaptive optics visual simulator enables us to identify those individuals that may benefit from a procedure for presbyopic correction like Laser Blended Vision and those that will respond poorly.
Adaptive Optics is an emerging technology which shows huge potential in imaging and visual quality testing. It is likely that the future of presbyopic treatment involves simulation using adaptive optics can help in true customization of treatment by altering aberrations like spherical aberrations and defocus based on individual tolerance and acceptance.
Conclusion:
Adaptive optics simulator gives patient specific tolerance limits of SA and also ability to study its impact on distance, near and intermediate vision. This can be used in customising laser presbyopia surgery
Leave a Comment