

Dr. Saurabh Mistry, M16776, Dr. Jyotirmay Biswas, Dr. Parthopratim Dutta Majumder
![]()
![]()
ABSTRACT:
Purpose: To study the clinical presentation and visual outcome of sympathetic ophthalmia (SO) in pediatric patients attending a tertiary care center.
Methods: Retrospective review of patient’s ≤18 years with sympathetic ophthalmia seen during the period 1997–2017.
Results: 17 patients were included. The inciting event was trauma in 13 patients whereas 4 patients developed SO following vitrectomy. The commonest presenting signs were anterior uveitis and exudative detachment. All patients were treated with systemic steroids, while 14 patients received additional immunosuppressive therapy. Of these, 4 patients needed more than one IMT drug to control the inflammation. 14 patients had a follow-up of more than 6 months. 4 patients developed recurrence on follow-up. The most common complication on long term followup was complicated cataract (9 patients) and secondary glaucoma (6 patients). Mean presenting best-corrected visual acuity (0.75 ± 0.60 logMAR) in the sympathizing eye improved significantly following treatment (0.26 ± 0.36 logMAR).
Conclusions: Appropriate immunosuppression can lead to favourable visual outcomes in the sympathizing eye of pediatric patients.
KEY WORDS:
Sympathetic Ophthalmia, Pediatric group, Imunosuppressives
INTRODUCTION:
Childhood blindness continues to be one of the major public health problems in developing countries. It is estimated that there are 1.4 million blind children in the world, two thirds of whom live in the developing countries, and that the causes of blindness in children vary according to region and socioeconomic development. [1, 2] Childhood blindness, especially if it is avoidable, is a particularly emotive subject more so, because of its significant impact on the child’s development, education, future job opportunities and quality of life. [3] A recent survey of childhood monocular blindness in a rural population in southern India found ocular trauma to be the second leading cause (the first being amblyopia due to uncorrected refractive errors) of visual impairment in the pediatric age group. [4]
Saxena et al. studied the pattern of ocular trauma in pediatric age group. They found that closed globe injuries accounted for 42.2% injuries, open globe for 53.9% whereas 3.9% were due to chemical injuries. Most common cause of injury was bow and arrow (15.2%) followed by house hold appliances (14.3%). Also, best corrected visual acuity of 6/12 or better was achieved in 79 eyes (91.86%) in closed globe group. However, only 17 eyes (15.45%) in open globe group could achieve this. [5] Penetrating injuries or open globe injuries have a higher risk of blindness not only from immediate ocular damage but also from long-term complications like sympathetic ophthalmia (SO).
SO is a bilateral diffuse granulomatous panuveitis that occurs after accidental or surgical insult to the uvea of one eye. After injury from either surgery or accident, a variable period of time passes before a sight-threatening inflammation develops in both the eyes. The incidence of SO ranges from 0.2 to 0.5% after penetrating ocular injuries and 0.01% after intraocular surgery. [11, 12] The disease usually responds rapidly to corticosteroid therapy, but recalcitrant cases may require the addition of other immunosuppressive agents. A severely injured eye with no prognosis for vision should be enucleated within 2 weeks of injury to prevent SO.
Recently, Kumar et al estimated the incidence of SO following trauma. It was 0.24% in the pediatric age group. [6] Though quite less, this complication assumes paramount significance because of its potential to cause blindness in both eyes following an injury to one eye. Recognition of signs and symptoms of SO is thus important because the disease is vision-threatening and many patients may end up with significant vision loss especially if treatment is not started quickly. Also, it is particularly challenging to manage pediatric patients, with very scanty literature available regarding management guidelines in such cases.
The current study was undertaken to look into the data of last 20 years’ in another tertiary eye care centre in Southern India. To the best of our knowledge the current study is the largest case series on pediatric SO from India.
METHODS:
This was a hospital-based retrospective case series that reviewed the files of all consecutive patients with SO at a single tertiary center between December 1997 and January 2017. The patients ≤18 years receiving a diagnosis of SO were included in current study. Cases with insufficient documentation and inadequate follow-up was excluded from the study.
All patients underwent detailed medical evaluation, including medical history, best corrected visual acuity (BCVA), visual field assessment, slit lamp microscopy, intraocular pressure (IOP) by applanation tonometry, and indirect ophthalmoscopy. All the patients underwent FFA, USG and OCT in sympathizing eye and in case of an uncertain clinical picture, patients underwent ICG.
SO was diagnosed on the basis of two or more signs in sympathizing eye, with history of trauma or surgery preceding the onset of intraocular inflammation in other eye. [6,9]
- Anterior segment inflammation
- Posterior segment showing vitritis, exudative retinal detachment, optic nerve head edema, nummular chorioretinal lesions, vasculitis or a sunset-glow fundus.
- Diffuse choroidal thickening in the posterior pole on B-scan ultrasonography (USG)
- Multiple pinhead leak with late dye pooling, optic nerve head staining on fundus fluorescein angiography (FFA) and/or suggestive indocyanine green angiography (ICG) and/or multiple serous retinal detachment on optical coherence tomography (OCT)
- Characteristic histopathology of the enucleated exciting eye
The data including sex, age, clinical presentation, ocular involvement, type of ocular injury, time of injury, time from first injury to development of disease and to presentation were entered into a computer database. Visual outcome and subsequent incidence of ocular complications such as cataract, ocular hypertension, hypotony, macular edema, choroidal neovascularization, subretinal fibrosis, retinal detachment were also recorded.
BCVA results were converted to logarithm of the minimal angle of resolution (logMAR) for statistical analysis and are presented as logMAR and Snellen equivalent. Decrease in visual acuity was defined as two-step decrease in BCVA in Snellen’s chart. Ocular hypertension was defined as an IOP greater than 21 mm of Hg and ocular hypotony was defined as IOP less than 6 mm of Hg. Uveitis was classified according to the Standardization of Uveitis Nomenclature (SUN) Working Group classification [10]
All statistical analyses were performed using SPSS (SPSS Inc, Chicago, Illinois, USA) statistical package. The statistical analysis was performed using SPSS 14.0 and any statistical tests with p – value less than 0.05 was considered as statistically significant. Descriptive statistics was used for continuous variables and frequency distribution was used to determine the distribution of qualitative variables. Wilcoxon signed rank test was used to determine the difference between pre treatment and final visit visual acuity.
RESULTS:
From December 1997 to January 2017, 17 patients ≤18 years of age with the diagnosis of SO were seen in our center. Eleven patients (64.7%) were male and six (35.3%) were female. The mean age at presentation was 11.1 ± 3.1 years (range: 5 – 17 years). The inciting event of SO in 15 patients was penetrating trauma, whereas 2 patients (developed SO following vitrectomy. The median time from initial injury to onset symptoms of SO was 59 days (range: 10 to 1215 days).
Average duration of follow-up was 58 months (range, 1.4 – 224.4 months).
The commonest presenting signs were anterior uveitis, exudative detachment and disc hyperemia.
Mean presenting BCVA in the exciting eye was 3.12 ± 1.25 logMAR units (median visual acuity PL +ve). 5 exciting eyes subsequently developed phthisis during the course of follow-up. 2 exciting eyes developed band shaped keratopathy on follow-up.
Mean presenting BCVA in the sympathizing eye was 0.75 ± 0.60 logMAR units (median visual acuity 6/36). 6 patients had visual acuity of 20/200 or worse. The most common complication on long term follow up was complicated cataract (9 patients), secondary glaucoma (6 patients) and subretinal fibrosis (3 patients).
Management :
All 17 patients received systemic steroids, with 6 patients receiving additional intravenous methylprednisolone at presentation. Immunosuppressives were concurrently started in 14 patients (82.35%), of these 4 patients needed more than one immunosuppressant drug to control the inflammation.
The commonly preferred first line immunosuppressant drug was azathioprine and the second line drug was cyclosporine in our patients. The average duration of immunosuppression required to control inflammation was 7.85 months (range, 2.5 to 22 months).
Recurrence of symptoms in sympathizing eye was noticed in 4 patients during the course of follow-up. Of these, one patient was not started on immunosuppressive therapy during the initial presentation.
Lensectomy with pars plana vitrectomy was performed in 3 sympathizing eyes during the course of the follow-up. Trabeculectomy to control secondary glaucoma was needed in one of the sympathizing eyes.
1 exciting eye underwent evisceration during the follow-up. Histopathological report suggested no granulomatous inflammation, and few chronic inflammatory cells. 1 exciting eye underwent enucleation and histopathological report suggested chronic granulomatous inflammation involving retina and choroid consistent with diagnosis SO.
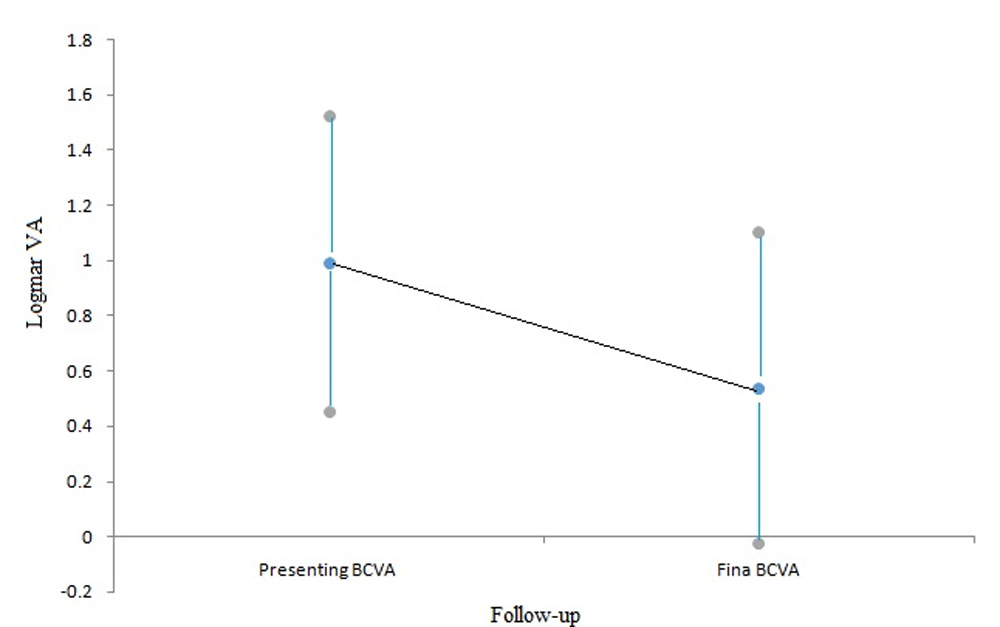
Mean final BCVA in the sympathizing eye was 0.26 ± 0.36 logMAR units (median visual acuity 6/9), which was significantly better than the presenting visual acuity with p value =0.038 using Wilcoxon signed rank test. [FIGURE 1] Good outcome (6/12 or better) was seen in 70.58% eyes (12/17), while 2 eye had fair outcome (6/12 to 6/60).
Three sympathizing eyes had poor visual outcomes (>6/60 snellen VA). Of these, one eye had poor visual outcome due to development of secondary glaucoma and subsequently patient underwent trabeculectomy to control the intraocular pressure. One patient had presented to our OPD almost after 3.5 years (1215 days exactly) after the initial inciting event, with presence of extensive subretinal fibrosis in the sympathizing eye. Third patient had multiple episodes of disease recurrence with complicated cataract and BSK at initial presentation.
Mean final BCVA in the exciting eye was 2.84 ± 1.49 logMAR units (median visual acuity PL +ve). 3 exciting eyes had very good improvement in visual acuity 6/12 or better at final follow-up.
DISCUSSION:
The patients in the current series developed SO following injury by a variety of mechanisms. This is consistent with the literature, where studies have reported sympathetic ophthalmia following trauma to be most likely cause. In our series, the commonest object causing trauma was wooden stick (23.5%). These findings correlate well with various studies done in India.(13,14)
However, more recent studies report injury from ocular surgery to be the more common cause.(15) Although incidence of sympathetic ophthalmia has declined in the recent past, prevalence of ocular surgery is increasing and necessitates careful monitoring of changing disease incidence. Sympathetic ophthalmia is a concern following multiple intraocular surgeries such as cataract extraction, paracentesis, and iridectomy, and is of particular concern following vitreoretinal surgery.
Vitreoretinal surgery is suggested to be the cause behind half of all sympathetic ophthalmia cases and, thus, upto 1 out of every 800 vitreoretinal cases.(16) Interestingly, in our case series two patients presented with SO following multiple vitreo-retinal surgeries after penetrating trauma and one patient following vitrectomy alone without any antecedent trauma. Performing multiple vitreo-retinal surgeries in a traumatized eye with poor visual prognosis may further increase the risks for developing SO in such eyes.
Our data showed that most of the patients (65%) developed SO within 2 months following the initial injury (median interval of 54 days). However significantly in six patients the onset was delayed (range, 7 months to 40 months). With late onset of disease, often there is unreliable historical information among the pediatric age group.(17) Also poor visual outcome can result from lack of awareness of the parents about this entity with late onset of disease. Hence it is important for the treating ophthalmologist to properly counsel the parents about the possibility of developing SO in the uninvolved eye in the near future.
All patients received systemic steroids as soon as the diagnosis of SO was made, and 6 patients (35%) also received intravenous methylprednisolone at an adequate dose prior to starting oral steroids. Subsequently, 82.3 % (14 of 17) received additional immunosuppression with azathioprine or methotrexate or cyclosporine in combination with steroids. In a similar study conducted by Kumar et al. only 50% patients received immunosuppressive drugs, as compared to our series. (18) In our series, azathioprine was the preferred first line drug (10 patients), failing which to control inflammation cyclosporine was used as second line IMT. Immunosuppressives were started only after obtaining clearance from the pediatrician or internist and was closely monitored by them. All the patients tolerated immunosuppressive drugs well and none developed any untoward side effects.
There has been debate regarding the only known means of prevention of sympathetic ophthalmia, i.e. removal of the injured eye (enucleation) or its content (evisceration) within a week after the traumatizing incident. In a retrospective study of 14 pediatric patients with SO conducted by Kumar et al. there were 4 enucleations and one evisceration during the follow-up period. (18) In contrast to this, in our study there were only one evisceration and one enucleation after the onset of SO. The decision regarding enucleation or evisceration needs to be made very carefully, because the vision in the exciting eye eventually may be better than the vision in the sympathetic eye in some patients. Till now no benefit of enucleation after the onset of SO has been noted in the study, and the lack of detailed data on the timing of enucleation made it difficult, if not impossible, to draw any conclusions to this end. (19)
Surprisingly, in our study three exciting eyes were found to have vision 6/12 or better at final follow-up after the onset of sympathetic ophthalmia. The presenting visual acuity was perception of light (PL) in these exciting eyes. Of these, two patients received immunosuppressive therapy to control the ocular inflammation. If there is reasonable doubt regarding the visual potential of an injured eye, then every effort should be made to preserve it considering the pediatric age group. With aggressive immunosuppressive therapy, good vision may be retained even in an exciting eye.
Our series also showed that 70.5% of pediatric patients with SO had a good visual outcome of 6/12 or better in the sympathizing eye, this is similar to the results found by Kumar et al. (18) Though in our series the use of immunosuppressive drugs to control inflammation was about 82%, the visual outcomes were comparable. But importantly to note is that in our series more than 80% patients had a longer follow-up duration of more than 6 months, which suggests that good visual outcomes continues to be maintained with the current treatment regimen.
To conclude, the early signs and symptoms of SO must be carefully watched for, and if the disease does develop, prompt and aggressive therapy with appropriate immunosuppression can lead to favourable visual outcomes in the sympathizing eye of pediatric patients. Creating awareness among the parents by the treating ophthalmologist of the possibility of development of SO in the uninvolved eye is of utmost importance for early recognition and management.
REFERENCES:
- World Health Organization. Global initiative for the elimination of avoidable blindness. Programme for the Prevention of Blindness and Deafness. Geneva: WHO, 1997 (WHO/PBL/97.61).
- World Health Organization. Preventing blindness in children: report of WHO/IAPB scientific meeting. Programme for the Prevention of Blindness and Deafness, and International Agency for Prevention of Blindness. Geneva: WHO, 2000 (WHO/PBL/00.77).
- Gupta N, Tandon R, Gupta SK, Sreenivas V, Vashist P. Burden of Corneal Blindness in India.Indian Journal of Community Medicine : Official Publication of Indian Association of Preventive & Social Medicine. 2013;38(4):198-206. doi:10.4103/0970-0218.120153.
- Bandrakalli P, Ganekal S, Jhanji V, et al. Prevalence and causes of monocular childhood blindness in a rural population in southern India. J Pediatr Ophthalmol Strabismus. 2012;49:303–307.
- Saxena R, Sinha R, Purohit A, Dada T, Vajpayee RB, Azad RV. Pattern of pediatric ocular trauma in India. Indian J Pediatr. 2002 Oct;69(10):863-7. PubMed PMID: 12450295.
- Kumar K, Mathai A, Murthy SI, Jalali S, Sangwan V, Reddy Pappuru R, Pathangay A. Sympathetic ophthalmia in pediatric age group: clinical features and challenges in management in a tertiary center in southern India. Ocul Immunol Inflamm. 2014 Oct; 22(5):367-72.
- Kilmartin DJ, Dick AD, Forrester JV:Sympathetic ophthalmia risk following vitrectomy: should we counsel patients. Br J Ophthalmol 2000, 84(5):448–449. 10.1136/bjo.84.5.448
- Kilmartin DJ, Dick AD, Forrester JV:Prospective surveillance of sympathetic ophthalmia in the UK and Republic of Ireland. Br J Ophthalmol 2000, 84(3):259–263. 10.1136/bjo.84.3.259
- Gupta V, Gupta A, Dogra MR. Posterior sympathetic ophthalmia: a single centre long-term study of 40 patients from North India. Eye 2008 22,1459-1464
- Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol 2005; 140:509 –516.
- Makley TA, Azar Sympathetic ophthalmia: A long-term follow-up. Arch Ophthalmol 1978;96:257-62.
- Marak GE. Recent advances in sympathetic ophthalmia. Surv Ophthalmol 1979;24:141-56.
- Krishnan M, Sreenivasan R. Ocular injuries in union territory of Pondicherry–clinical presentation. Indian J Ophthalmol. 1988 Jun;36(2):82–5.
- Misra S, Nandwani R, Gogri P, Misra N. Clinical profile and visual outcome of ocular injuries in a rural area of western India. The Australasian Medical Journal. 2013;6(11):560-564. doi:10.4066/AMJ.2013.1876
- Kilmartin DJ, Dick AD, Forrester JV. Prospective surveillance of sympathetic ophthalmia in the UK and Republic of Ireland. Br J Ophthalmol. 2000 Mar;84(3):259–63.
- Kilmartin DJ, Dick AD, Forrester JV. Sympathetic ophthalmia risk following vitrectomy: should we counsel patients? Br J Ophthalmol. 2000 May;84(5):448–9.
- Acuna OM, Yen KG. Outcome and prognosis of pediatric patients with delayed diagnosis of open-globe injuries. J Pediatr Ophthalmol Strabismus. 2009 Aug;46(4):202-207; quiz 208-209.
- Kumar K, Mathai A, Murthy SI, Jalali S, Sangwan V, Reddy Pappuru R, et al. Sympathetic ophthalmia in pediatric age group: clinical features and challenges in management in a tertiary center in southern India. Ocul Immunol Inflamm. 2014 Oct;22(5):367–72.
- Sen HN, Nussenblatt RB. Sympathetic Ophthalmia: What Have We Learned? Am J Ophthalmol. 2009 Nov;148(5):632–3.
TABLE 1: Characteristics of the study population with sympathetic ophthalmia
| Serial No | Age (yrs) | Time from injury to onset of symptoms (days) | Mode of injury | Sympa-thizing eye | Presen-ting Visual acuity (logMAR)- OD;OS | Mode of treatment | Duation of IMT (days) | Recur-rence | Final visit visual acuity (logMAR) – OD;OS | Follow-up duration (days) | Comp-lications in sympa-thizing eye |
| 1 | 11 | 24 | Metal Rod, S/P Vitrectomy | OD | 0.2;0.48 | CS+IMT(1) | 75 | No | 0.0;4.0 | 1439 | Cataract |
| 2 | 7 | 38 | Details of Trauma NA | OD | 0.2;3.5 | CS+IMT (1) | 210 | No | 0.0;0.3 | 812 | Glaucoma |
| 3 | 14 | 1095 | Trauma with stick | OD | 1.0;4.0 | CS+IMT (3) | 540 | Yes (1) | 3.5;4.0 | 1813 | Cataract; Glaucoma; Subretinal fibrosis |
| 4 | 10 | 15 | Fist injury | OS | 3.5;3.0 | CS+IMT(1) | 480 | Yes (2) | 4.0;2.77 | 6320 | Cataract |
| 5 | 15 | 10 | Hit by Stone | OS | 3.5;0.0 | CS | NA | No | 4.0;0.0 | 6732 | Nil |
| 6 | 15 | 66 | Chisel & Hammer | OD | 3.5;3.5 | CS+IMT(1) | 660 | No | 0.1;4.0 | 5648 | Cataract; Glaucoma; RD |
| 7 | 8 | 40 | Injury with hair band | OS | 0.0;0.6 | CS | NA | No | 0.0;0.2 | 1710 | Nil |
| 8 | 12 | 240 | Details of trauma NA, S/P PK | OD | 1.0;1.0 | CS+IMT (1) | 120 | No | 0.0;2.77 | 830 | Cataract; Glaucoma |
| 9 | 13 | 1095 | Injury with rubber baloon | OS | 3.0;1.0 | CS | NA | Yes (1) | 3;0.18 | 2660 | Cataract; Glaucoma |
| 10 | 12 | 545 | Trauma with stick; S/P Cataract Sx | OD | 0.18;2.0 | CS+IMT (1) | 115 | No | 0.0;2.0 | 400 | Nil |
| 11 | 9 | 47 | Trauma with aluminium plate | OD | 0.48;0.48 | CS+IMT(2) | 150 and ongoing | No | 1.0;1.0 | 155 | Cataract |
| 12 | 11 | 59 | Trauma with stick; S/P Vitrectomy | OS | 3.5;0.3 | CS+IMT(1) | 120 | No | 4.0;0.0 | 125 | Nil |
| 13 | 9 | 50 | Trauma with stick | OD | 0.78;3.5 | CS+IMT(1) | 189 | No | 0.0;0.1 | 239 | Cataract |
| 14 | 5 | 1215 | Intraocular Surgery details NA | OD | Fixates and follows; 4.0 | CS+IMT(2) | 70; lost to follow-up | No | Not fixating; 4.0 | 76 | Subretinal fibrosis |
| 15 | 11 | 350 | S/P Vitrectomy | OD | 0.78;4.0 | CS+IMT(1) | 120 | No | 0.48;4.0 | 406 | Cataract |
| 16 | 17 | 54 | Fire cracker injury | OD | 2;3.5 | CS+IMT(2) | 309 and ongoing | Yes (1) | 0.18;3.0 | 380 | Glaucoma; Subretinal fibrosis |
| 17 | 10 | 50 | Fire cracker injury | OD | 0.78;4.0 | CS+IMT(1) | 30 and ongoing | No | 0.18;4.0 | 42 | Nil |
FIGURE 1: Visual Outcome in Sympathizing eye: Mean plot with 95% CI showing significant difference between presenting and final BCVA. Wilcoxon signed rank test (p = 0.038 < 0.05).
Leave a Comment