
Dr. Rajvin Samuel Ponraj, P20063, Dr.
Sagarika Das, Dr. Mayur Dutta Bharali, Dr. Narayan Bardoloi
Abstract
Purpose –To analyse postoperative refractive outcomes of a single surgeon and to compare 3 calculators: Alcon AcrySof IQ Toric Web Based Calculator (Alcon), Holladay IOL Consultant Software of Verion and ASCRS Toric Calculator (Barrett). We attempt to identify optimized strategy for selecting toric IOL by looking at each calculator individually and then together.
Study design–Retrospective comparative clinical trial
Material and Methods
33 patients (41 EYES) who underwent phacoemulsification surgery with insertion of Toric IOL over the past one year were analysed. Recommended lens power target refraction, Toric power, surgery induced astigmatism, predicted residual astigmatism andIOL placement were collected and compared.
RESULTS
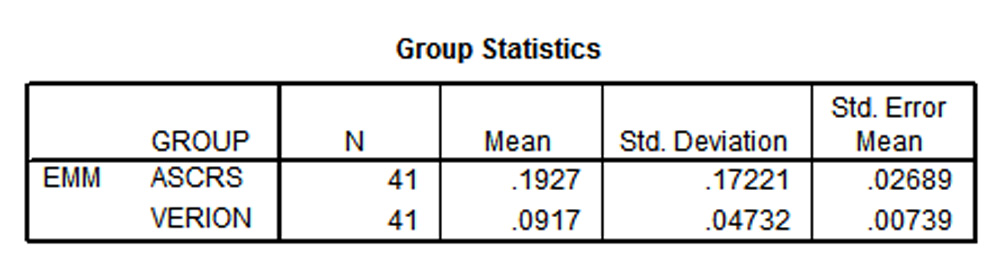
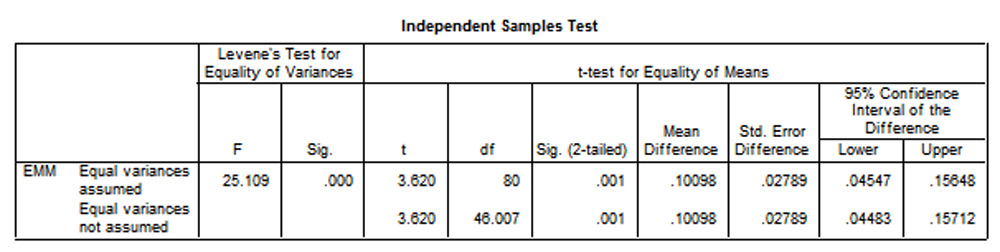
Mean standard error of target refraction were 0.1927 +/- 0.17221 and 0.0917 +/- 0.04732 by ASCRS Barett and Verion respectively. A statistically, significant difference in target refraction between ASCRS Barrett and Verion(Holladay)was observed (P<0.01),with latter being more accurate.
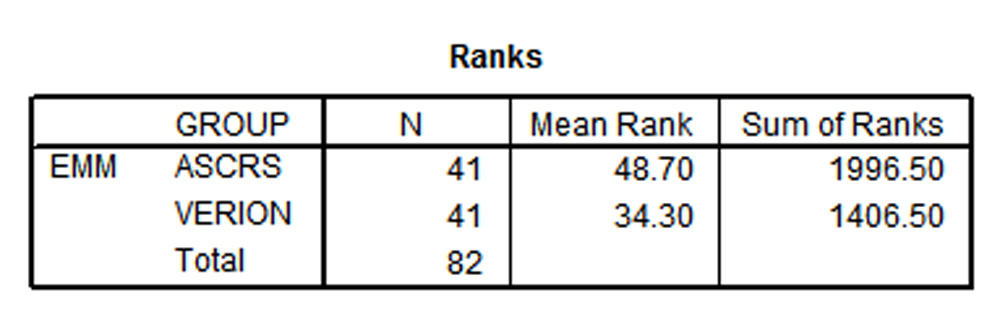
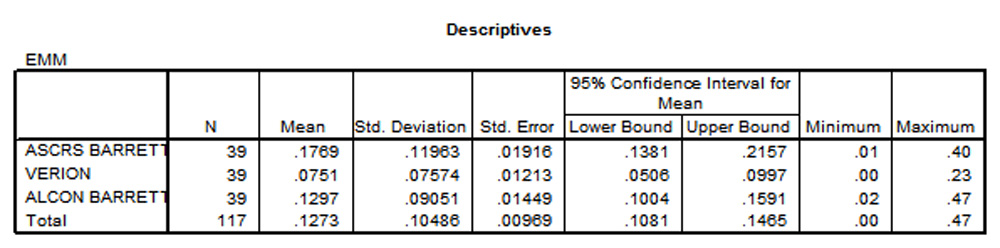
Mean standard error in Toric cylinder power were 0.1769 +/- 0.11963, 0.0751 +/- 0.07574, 0.1297 +/- 0.10486 by ASCRS Barett, Verion and Alcon Barrett respectively.In terms of Toric cylinder power, statistical difference was more (P < 0.001)with Verion and less accurate with ASCRS Barrett.
CONCLUSIONS
In our series, it was observed that majority of patient’s IOL power were closer to emmetropization when calculated with the Verion system when compared to online calculator ASCRS Barrett. There was a significant difference in the Toric cylinder power between Verion and ASCRS Barrett. However Toric cylinder powers were comparable between Verion and ALCON Barrett. IOL placement was similar between ALCON and ASCRS Barrett online calculators.
Introduction
One of the most successful methods to reduce astigmatism at the time of cataract surgeryis arguably the Toric intraocular lenses (IOLs). However,it was found that residual astigmatism following Toric IOL implantation remains a concern, with 36.5% of eyes not within 25% of their target astigmatism correction and 35.2% having uncorrected distance visual acuity worse than 20/251,2.Patients are offered the opportunity to correct corneal astigmatism at the time of cataract surgery and achieve spectacle independence for distance vision with the help of these lenses3.
A small error in an IOL’s position may affect the patient’s uncorrected visual acuity significantly with the use of Toric IOL’s. For every one degree of error in a Toric IOL’s rotational alignment, there is a 3.3 percent decrease in the correction of astigmatism.If there is a mis-alignement in the axis by 10 degrees, then that corresponds to a 33 percent loss of the Toric correction4.
Surgeonsare able to deliver optimal refractive outcomes for cataract patients with astigmatism by facilitating IOL selection and axis that is most suitable.Online calculators namely the ASCRS Barett Toric, and Alcon Barett Toric intraocular lens (IOL) implantation and the Verion (Holladay formula) are designed to provide the most accurate preoperative prediction of residual astigmatism, surgically induced astigmatism and also allow better management of corneal astigmatism, leading to better uncorrected visual acuity5.
Materials and Methods
This is a retrospective analysis of 41 eyes of 33 patients who underwent cataract extraction by phacoemulsification with Toric IOL implantation through a 2.2 mm limbal incision by a single surgeon at a tertiary eye care centre in Jorhat, Assam.Patients with intraoperative complications or irregular astigmatism, corneal diseases were excluded from the study.Data were obtained from the electronic medical record, IOL master and Verion reference unit and entered into the online calculators.
Methods of calculation
The data that we included were as follows.Preoperative vision and astigmatism, measurements made with the IOL master namely white to white diameter(WTW), Anterior Chamber depth(ACD),measurements made with Verion namely : K reading(K), Axial length(AL), Optimized IOL parameters.
Ideal lens calculator was determined by analysing post-op refractive outcomes and its closeness to emmetropization. These data were compared with the online calculators.We performed this by incorporating data into our online tool. We entered the name of surgeon and name and details of patient. We entered desired spherical equivalent ,post-operative refractive outcomes and a constant for Toric IOL. The patient’s data namely eye, Flat K, steep K and their respective axis, Axial length, Optical ACD, surgery induced astigmatism and the location were also entered. We then selected the calculate option.
The display on the screen recommends Toric IOL power and its axis alignment for preferred post-operative spherical equivalent and residual astigmatism.
STATISTICAL ANALYSIS
All statistical analysis were performed using Statistical package for social science(SPSS,version 17) for Microsoft windows. The data were not normally distributed. And therefore parametric tests /Non parametric were performed. The data were expressed as Mean and SD. A one way analysis of variance with a post hoc Tukey HSD/ Kruskall Wallis was used for notnormally distributed continuous data. Independent sample students t test/ Mann Whitney test were used to compare continuous variables between two groups. A two sided p value< 0.05 was considered statistically significant.
T – Test
P value < 0.01
Mann-Whitney Test
Oneway
P value < 0.001
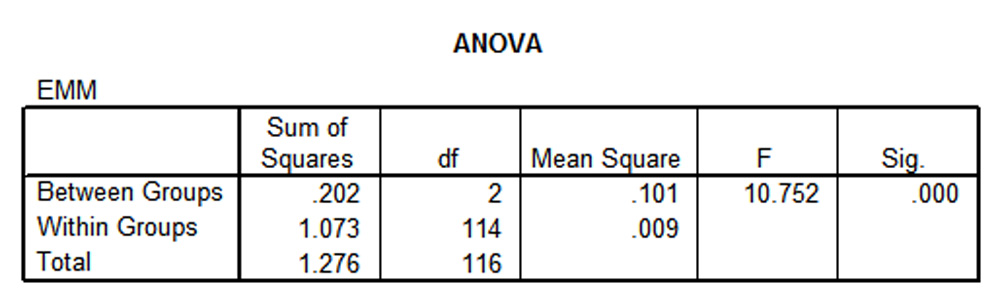
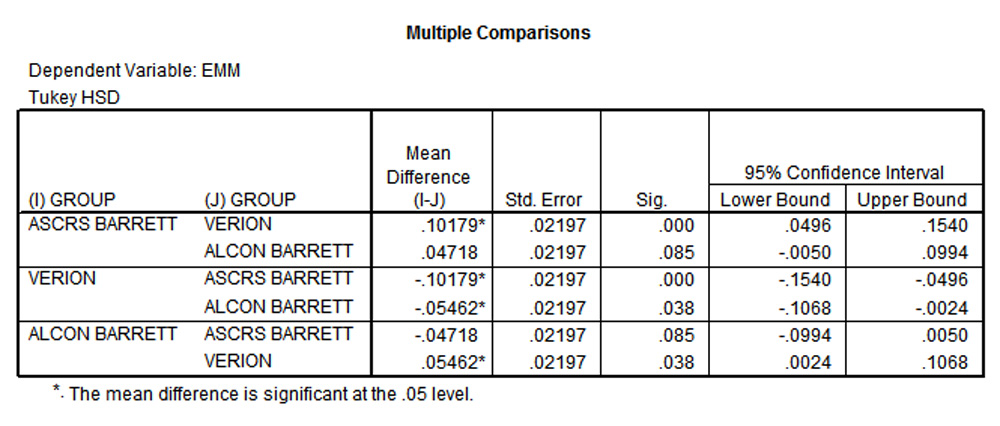
Post Hoc Tests
Results
There was a male preponderance(65 %) in our study as shown in Fig 1.Preoperative astigmatism of the eyes(Fig 2 ) were as follows based on the Verion reference unit. 6 eyes (14.6 %) had oblique astigmatism,29 eyes (70.7 %) had with the rule astigmatism, 6 eyes (14.6%) had against the rule astigmatism. Mean standard error of target refraction were 0.1927 +/- 0.17221 and 0.0917 +/- 0.04732 by ASCRS Barett and Verion respectively. A statistically, significant difference in target refraction between ASCRS Barrett and Verion (Holladay) was observed (P<0.01), with latter being more accurate.
Mean standard error in Toric cylinder power were 0.1769 +/- 0.11963, 0.0751 +/- 0.07574, 0.1297 +/- 0.10486 by ASCRS Barett, Verion and Alcon Barrett respectively. In terms of Toric cylinder power, statistical difference was more (P < 0.001) with Verion and less accurate with ASCRS Barrett.
Fig 1:
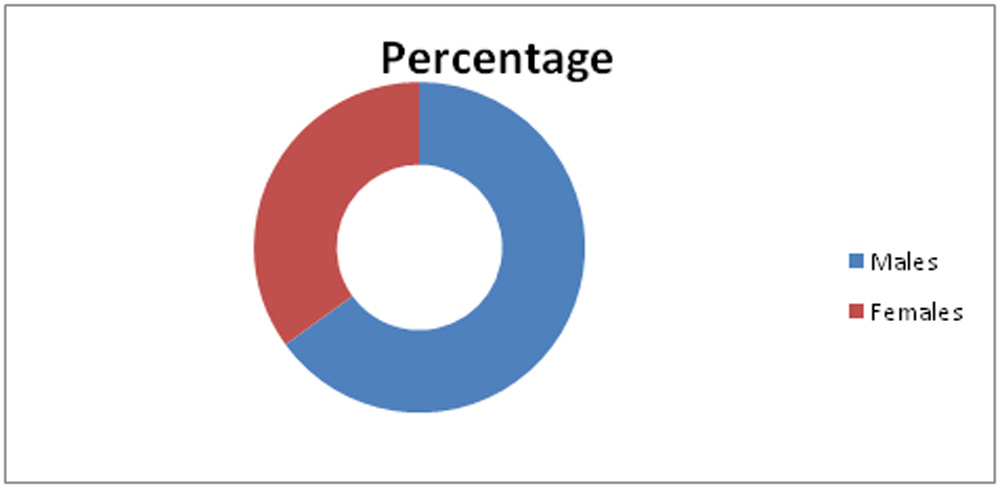
Fig 2:
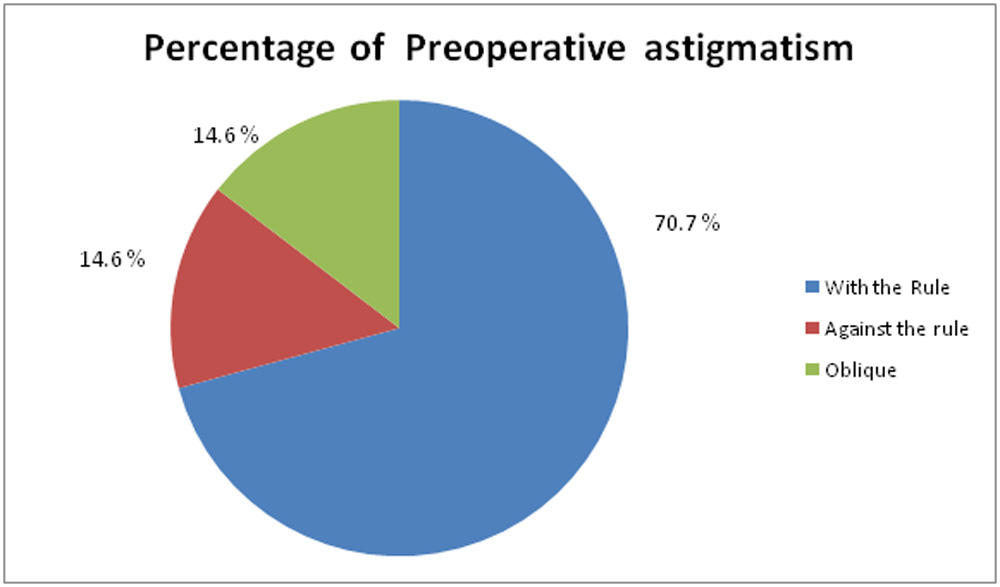
Fig 3: Comparison of target refraction of IOL power between Verion and ASCRS:
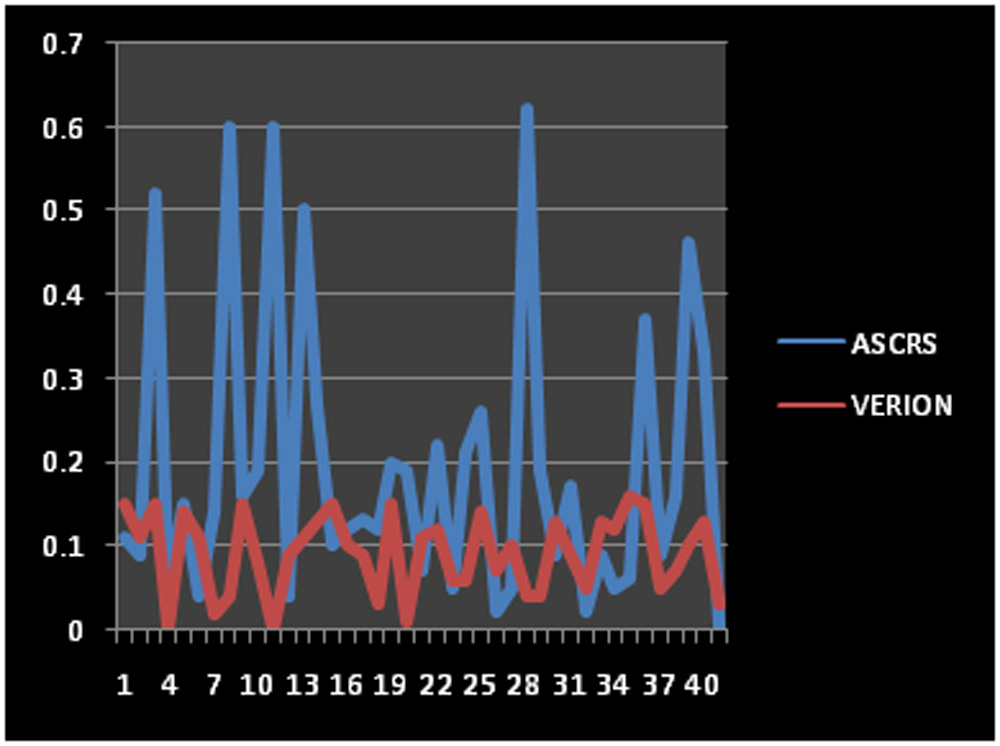
Y AXIS : TARGET REFRACTION
X AXIS : Number of patients
Fig 2: Comparison of Toric Cylinder power between Verion and ASCRS :
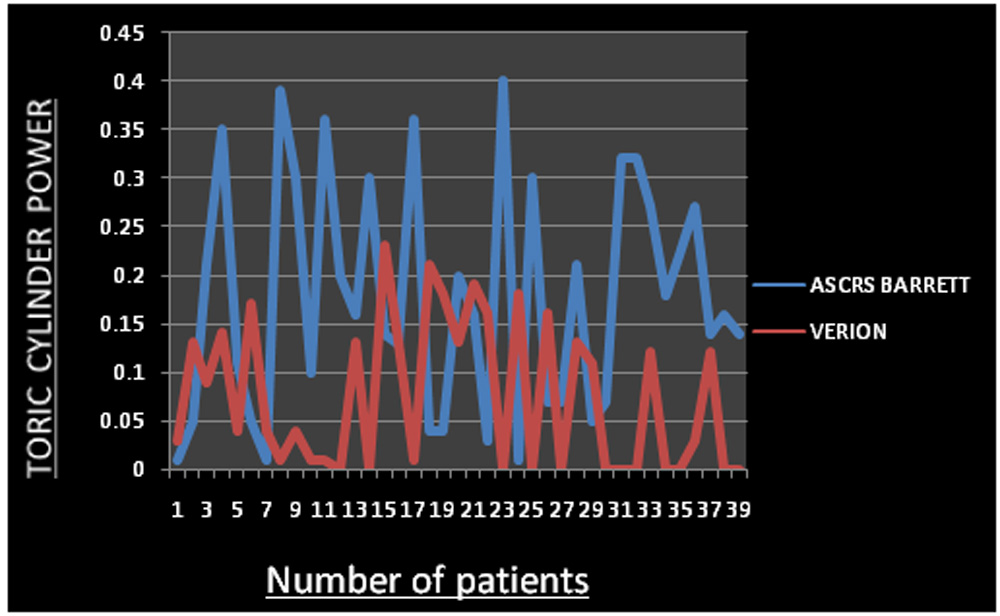
Fig 3: Comparison of Toric cylinder power between Verion and ALCON :
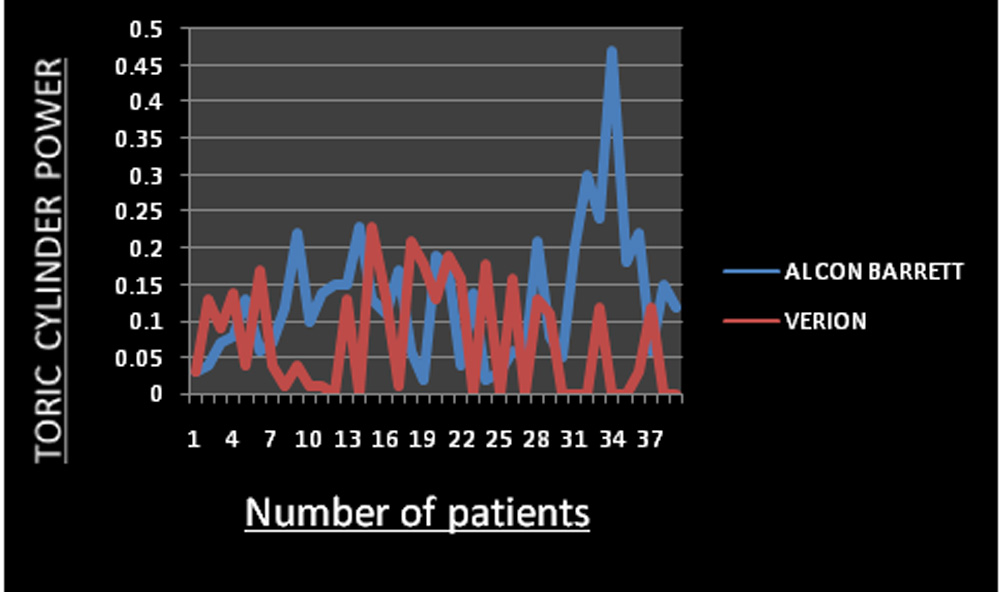
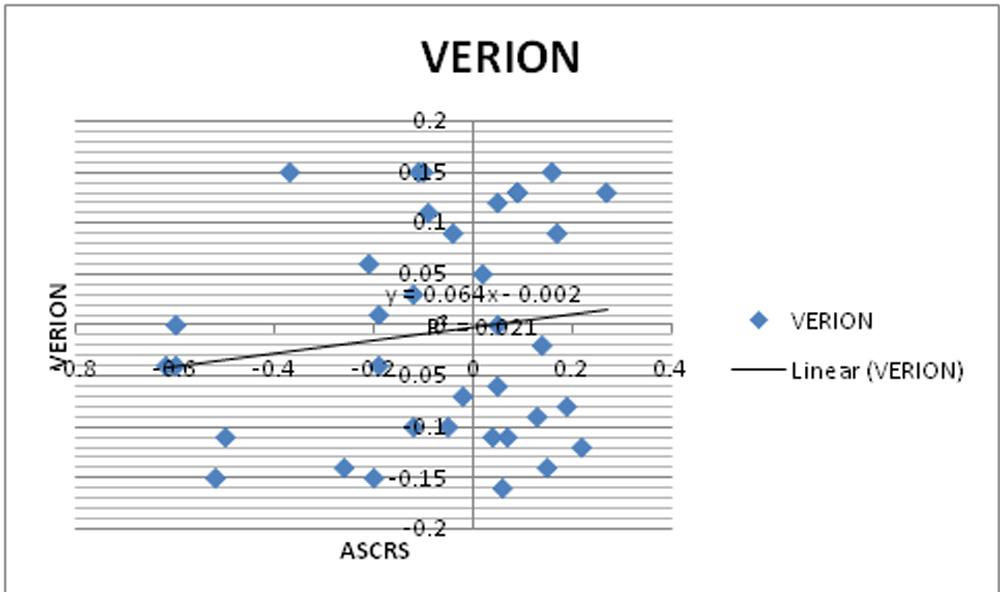
Fig 4: Scatter plot showing positive correlation of target refraction between ASCRS and VERION:
Discussion
It is more challenging to choose the correct Toric IOL than a spherical IOL power as the magnitude and axis of cylinder power are required.The Barrett Toric calculator is made available on the ASCRS website which is a fifth generation formula.Patient’s data required for calculation includes keratomtery, axial length, optical ACD, surgically induced astigmatism and its location, desired spherical equivalentpost-operative refractive outcome, A constant for Toric IOL. The Toric calculator menu displays the Toric IOL and Axis alignment,preferred IOL power for post-operative spherical refractive outcome, preferred Toric power for post-operative residual astigmatism. The thickness of lens and white to white diameter (WTW) are optional data6.
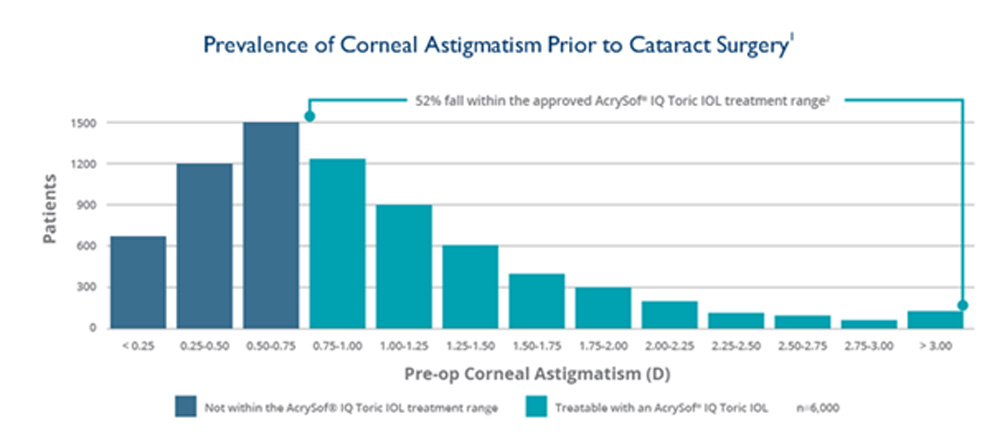
An online Toric calculator is also made available by Alcon which incorporates a Barrett Toric algorithm.We can derive best preoperative prediction of residual astigmatism based on this algorithm7. The posterior corneal astigmatism is taken into account with this calculator.Anatomically,the horizontal diameter is always greater than the vertical, therefore, the radius of the posterior cornea is more steep in the vertical than the horizontal meridian. Posterior corneal curvature behaves as a minus lens, hence its steepness contributes to against the rule astigmatism of the magnitude of 0.50 D.Corneal astigmatism≥ 0.75 D is seen inmore than 50 percent of the patients who undergo cataract surgery.This limits optimal visual outcome if left uncorrected as shown8 in fig 5.
FIG 5:
(My Alcon.com)
A centroid value for surgical induced astigmatism (SIA)is designed to improve refractive predictability6,8. The SIA is influenced by the incision size and location.Parameters such as the radius, thickness and rigidity of cornea also varyfrom one patient to another. Hence a centroid value of 0.10 to 0.20 is taken into account to enable calculations to a great extent. Also this enables calculation of patient-specific effective lens position.
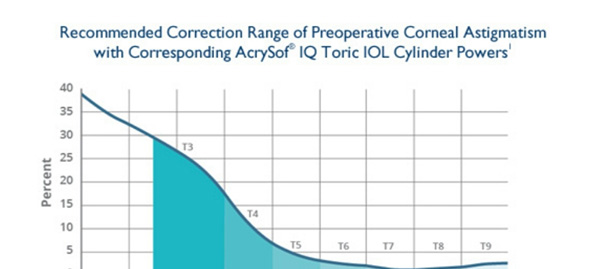
Candidates who are selected for Toric IOL implantation should have astigmatism greater than or equal to 0.75 D, should present with preoperative regular astigmatism,have an intact capsular bag,no pre-existing ocular pathology,no previous refractive surgery,desire improved distance vision with less dependence on glasses.The Acrysof IQ Toric lenses feature a wide range of different cylinder powers as shown in Fig 6.
FIG 6:
(My Alcon.com)
The reference point that many surgeons use for determining the astigmatism is the SIA which is created by incisions in cataract surgery and can be useful in Toric IOL selection.According to Dr Hill,‘the SIA is the change in both the power and, to a lesser degree, the orientation of the principal meridians following a corneal incision9’.We determine the amount of SIA on the basis of incision location, size, architecture,corneal radius, thickness, rigidity and the stretching of the incision as the folded IOL passes through it9.
There are 2 major componentsof the Verion image-guided system: the reference unit and the digital marker. There is a measurement module in the reference unit that provides the biometric data (K values, limbus–pupil position, and diameter) and captures a high-resolution image of the eye for later intra-operative use. Patient fixation is done with the help of 1 light-emitting diode (LED) (red, wavelength 624 nm). By observing the position and shape of 15 projected light reflexes created by 3 infrared LEDs (830 nm) and 12 white LEDs (450 nm), the corneal curvature and cylinder are calculated. The 3 infrared reflexes cover a diameter of approximately 1.0 mm during the focusing phase and the 12 reflections of the white LEDs approximately 2.8 mm centred on the cornea for a standard eye with a regular cornea at the time of the snapping phase. This Image guided system is devised for standardized surgical planning which in turn helps provide more consistent surgical outcomes10.
Intraoperative assistance and keratometry performance are guaranteed with the Verion Image – guided system. Keratometry comparability and repeatability data for this new system are sparse.Surgically induced astigmatism and Toric IOL implantation are planned with this system.The three phases inthe image- guided system are namely preoperative measurements, imaging, surgical planning andsurgical guiding. The biometric data in the vision planner software are processed in the reference unit.IOL power calculation using various formulas can be done with this software. An astigmatism planner for the surgical procedure helps to plan the location of corneal and limbal incisions. After the surgical procedure is planned, the data collected are exported to a Universal Serial Bus Stick or uploaded onto a network and then transferred to the digital marker. On the basis of vessel features, the digital marker in the image-guided system assists the surgeon in planning and performing surgical procedures on the eye.A digital overlay in the surgeon’s microscope,helps track the patient’s eye, allowing compensation for the cyclotorsional rotation. It visually guides the surgeon while placing planned corneal incisions and creating the capsulorhexis. The digital marker also helps correct IOL centration and performs precise IOL alignment if a Toric IOL is to be implanted. At the end of the measurement, a reference image of the patient’s eye is taken and the indication lights provide a quality estimate for the measurement of astigmatism, vessel, and corneal power. Each measurement is given a traffic light sign like red, yellow or green which grades the quality of the image.After evaluating the quality of the measurement, the examiner decides to accept it as sufficient or to perform another one11.
The VERION Reference Unit takes up diagnostic digital measurements and creates a high-resolution digital image of the patient’s eye, capturing scleral vessels, limbus and iris.This “fingerprint”of the eye is used throughout the procedure, allowing you to precisely position all incisions and alignment in real time according to your surgical plan.This device supports the export of the reference image, preoperative measurement data, and surgical plans for use with the VERION Digital Marker devices through a USB memory stick12.
The Holladay 2 formula is incorporated in the Verion reference unit .The seven variables taken into account are namely the age of patient,previous refraction of the patient,axial length, limbal white to white,anterior chamber depth, central corneal power and lens thickness.The astigmatic sliding scale is an option in the reference unit which displays optimal balance between corneal surface and IOL astigmatism by IOL or arcuate cuts and thereby determines the SIA.By moving the scroll along the astigmatic sliding scale, the amount of residual astigmatism will change. A diagram is displayed which shows the planned incision position represented as blue arcs andIOL placement axis represented as red solid line, The SIA in the Verion Reference unit display is checked to calculate the IOL placement axis and the closest IOL astigmatism correction.An optimize option when clicked after feeding all data will display the IOL power, Toric power, expected residual astigmatism,expected post K reading and IOL placement which can then be exported to an external device13.
Some of the considerations are as follows.The WTW measurements generally show lower accuracy; therefore, the measurement should be used cautiously and should also be assessed with other biometric devices.The manufacturer of the image-guided system also states that the determination of axis alignment works best with an astigmatism power above approximately 0.75 D. One disadvantage of the image-guided system is that it does not perform an AL measurement.Hence,it is necessary to measure the value using a different device and importing the data (e.g., from the IOL Master) or manually transferring it to the Vision Planner software.
References
-
- Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J.,Toric intraocular lenses in thecorrection of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016; 123(2):275–286.
- Hirnschall N, Hoffmann PC, Draschl P, Maedel S, Findl O, Evaluation of factors influencing the remaining astigmatism after Toric intraocular lens implantation, J Refract Surg. 2014;30(6):394–400
- Toric intraocular lenses: Historical overview, patient selection, IOL calculation, surgical techniques, clinical outcomes, and complications, J Cataract Refract Surg 2013; 39:624–637.
- Toric IOLs: Four Options for Addressing Residual Astigmatism, Eyenet magazine,American academy ofOphthalmology, April 2012.
- Alpins N, Barrett GD, Hansen MS, Berdahl JP, Hardten DR, Holladay JT. Innovative toric IOL calculators and how to use them: Barrett Toric Calculator. Cataract Refract Surg Today Europe. May 2015 supplement.
- Noel Alpins,Graham D.Barrett, John.P Berdahl, Jack T. Holladay, Innovative Toric IOL calculators and how to use them, cataract & refractive surgery today Europe , May 2015
- Abulafia A, Barrett GD, Kleinmann G, et al. Prediction of refractive outcome with Toric intraocularlens implants. J Cataract Refract Surg. 201; 41(5):936-944.
- Hill Distribution Data. Provided courtesy of Dr. Warren Hill,https://www.doctor-hill.com/iol- main/astigmatism_chart.htm. Accessed September 29, 2015.
- Erin L. Boyle EyeWorld Senior Staff Writer,Surgically induced astigmatism caused by multiple factors, Cataract editor’s corner of the world, Ophthalmology news, Eyeworld, February 2014.
- Exploring the Cataract Refractive suite featuing The Verion image guided system, Insert to Cataract and Refractive surgery Today, June 2014.
- Abdel Hamid ElhofiHany Ahmed Helaly,Comparison Between Digital and Manual Marking for Toric Intraocular Lenses,a randomized trial,Medicine (Baltimore). 2015 Sep; 94(38)
- Cheryl Guttman Krader, New system helps cataract surgeons improve refractive precision,OphthalmologyTimes , January 01, 2014
- Stephen S. Lane, Improving refractive outcomes with the verion system, Cataract and Refractive surgery Today, September 2014.
Leave a Comment