
Dr. Anup Kumar Goswami, G08117, Dr. Nidhi, Dr. (Col) B L Goswami
Painless progressive nodule in eyelid alongwith cervical lymphadenopathy typically brings to mind diagnosis such as Tuberculosis, with the typical associated sign/symptoms.However, this is not always the case and Rosai-Dorfman disease is a condition which mimics the same and is not easy to diagnose. Rosai-Dorfman disease is a rare, idiopathic, benign proliferative histiocytic disorder,characterized by massive painless cervical lymphadenopathy,fever,leukocytosis, and elevated ESR[1].Extranodal involvement occurs in skin, nasal cavity and paranasal sinus, orbit,eyelid, bone, salivary gland and central nervous system[2].Eye involvement is infrequent and most often seen in the orbit or eyelid and rarely in lacrimal gland[3].We report a case of Rosai-Dorfman disease that had ocular involvement in eyelid and orbit.
CASE REPORTA 30-yr-old woman presented with complaints of painless lump in left lower lid,which was slowly progressive, and protrusion of left eye.History revealed that patient was consulting ENT specialist for nasal polyp.and was advised to get an opinion of ophthalmic surgeon for lid swelling. There were no other ocular/ systemic complaints but for the presence of multiple nodules in neck.

Torch-light examination showed firm nodular rubbery swelling in lateral one third of leftlowerlid with axial and upwardsproptosis of left eye( Fig.1).The nodule was non tender with negative transillumination. The size was approx. 6mmx 5mmx 3mm with no change on valsalvamaneuver.The margins were identifiable all over except inferiorly while the nodule was adequately mobile. The swelling was non pulsatile without any bruit.There was mild fullness of lid medial to the swelling.BCVA was 6/6 both eye.Function and anatomy of lids was normal. Ocular motility was within normal limits without any diplopia.
Fig1. : Nodule in lateral one third of left lower lid with axial and upwards proptosis
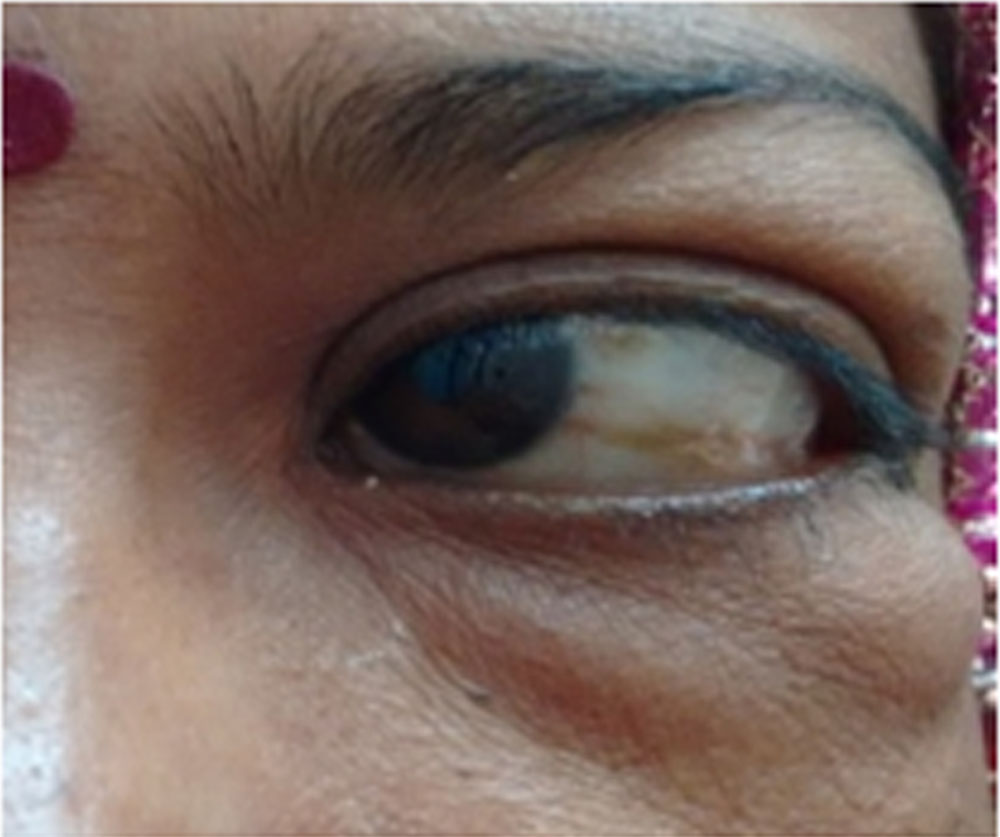
Slit-lamp examination revealed a normal forniceal and conjunctivalconjunctiva with scattered patches of melanosis in bulbar conjunctiva(Fig.2).No sentinel vessel seen. Pupillary reactions were brisk with quiet anterior chamber and normal anterior vitreous.Intraocular pressures were 15mmHg and 16 mmHg on applanation in Right and left eye respectively with normal fundus oculi.Fig2. :melanosis in bulbar conjunctiva, normal ocular motility
Systemic examination: showed presence of widespread cervical and pre auricular lymphadenopathy (Fig.3) with large sized nodes.Rest of the examination was within normal limits. There was no history of fever, weight loss or any other systemic complaint.There was no history of any treatment for systemic disease, any vernacular treatment at home or a traditional healer.
Fig.3: massive cervical and pre auricular lymphadenopathy
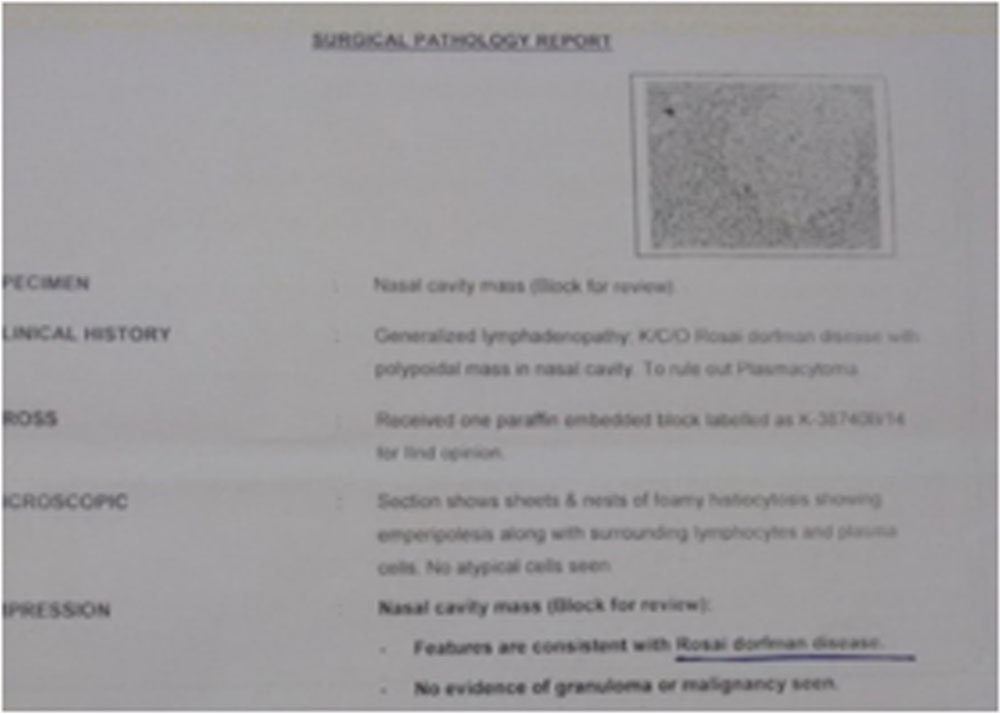
Records revealed that patient was consulting ENT specialist for difficulty in breathing through nose whence a diagnosis of nasal polyp was made.She was operated for the same and polyp was resected and sample sent for histopathological analysis. Laboratory testing revealed leukocytosis and elevated erythrocyte sedimentation rate (35 mm/h). Monteux test was inconclusive for Tuberculosis and X raychest was normal.Histopathology examination (Fig.4) of the nasal sample sent showed sheets and nests of foamyhistiocytosis withemperipolesisdiagnostic of RosaiDorfman disease and ruling out plasmacytoma /other malignant disease.
Fig.4:Histopathology report confirming presence of RosaiDorfman disease
CT scan of orbits revealed extent and involvement of tissues (Fig.5) with retrobulbar mass in left orbit extending to lower lid , leading to proptosis and lump in lid
Fig.5: CT scan showing involvement of left orbit

Literature was reviewed and patient was started on oral corticosteroids and referred to tertiary care center for expert management.
DISCUSSION
Rosai-Dorfman disease(RD) or more appropriately Rosai-Dorfman- Destombes (RDD) diseaseis a rare, idiopathic, benign proliferative histiocytic disorderand was described in 1969[1]Destombes in 1965[4] reported four cases of ″adenitis with lipid excess″, in children and young adults which went unnoticed till Rosai and Dorfman four years later characterized the pathological features of this disorder which they called sinus histiocytosis with massive lymphadenopathy[5]. It is common in children and adolescents and is characterized by massive cervical lymphadenopathy, fevers, leukocytosis, and elevated erythrocyte sedimentation ratewith a slight male predominance.No specific predilection for geographic location or race is attributed. The etiology is unknown and viruses like Epstein-Barr virus and Human Herpes virus 6, immune dysfunction, or an aberrant response to an unspecified antigenhave been implicated[6,7].Current hypothesis is that the defective Fas/FasL signaling leading to altered apoptosis may be an important mechanism whereby uncontrolled histiocytic proliferation is triggered. The presence of characteristic histiocyte, derived from circulating mononuclear cells, long history and an increased incidence of serum autoreactive antibodies during active disease suggest a possible pathogenic correlations with a dysregulatory process.
Extranodal disease has been reported in 43% of patients. In some casesextranodal manifestations represent the predominant or even exclusive manifestation of the disease. Lymphadenopathy, may or may not develop later in the disease course [5]. The most common extranodal sites, in the decreasing order of frequency, are skin, nasal cavity and paranasal sinus, orbit,eyelid, bone, salivary gland and central nervous system. Simultaneous involvement of multiple extranodal sites is possible [5]. Hepatosplenomegaly, unlike in other histiocytic disorders, is uncommon [5].In the present case extranodal involvement occurred in nasopharynx , eyelid and orbit along with massive cervical lymphadenoparthy. Uvea, lacrimal gland , optic nerve (compression) involvement have also been reported in many cases. Orbital involvement is the most common of ophthalmic manifestations[3].
It is important to be familiar with the clinical and diagnostic histopathologic features of this entity especially when the disease presents extra-nodally in an isolated form.Clinical course of Rosai-Dorfman disease is chronic and variable with episodes of exacerbation alternating with periods of remission, where the timing and duration of each phase is entirely unpredictable .Typically, RD disease undergoes spontaneous remission after a protracted course but may develop recurrences.
Investigations usually performedto know the extent of affection of tissues and/or to plan treatment are ophthalmic ultrasound; head and neck CT scan and biopsies of epibulbar, nasal and tracheal tissues.Rosai-Dorfman disease can be difficult to diagnose and requires histopathologic examination. Characteristic histology includes a polymorphous infiltrate with a predominance of proliferating histiocytes.2 The histiocytes usually contain prominent vesicular nucleoli and abundant pale, eosinophilic cytoplasm and exhibit lymphophagocytosis or emperipolesis.2 Immunohistochemisry is useful in differentiating RDD disease from other histiocytic disorders. The RDD histiocytes are strongly positive for S-100 and CD 68 proteins. Impression cytology technique for rapid intraoperative diagnosis of Rosai-Dorfman disease based on known cytological characteristics can be adopted.Laboratory findings in Rosai-Dorfman disease include hematological abnormalities such as normocytic or microcytic anemia, hemolytic anemia, elevated erthrocyte sedimentation rate and polyclonal hypergammaglobulinemia.Scintigraphyand bronchoscopy may also be done in diagnostically difficult cases.
Treatment depends on the site, extent and nature of the lesion.Only about 50% of patients with Rosai-Dorfman disease need some form of treatment[8]. The ideal treatment protocol for Rosai-Dorfman disease is not etablished and options include, observation for mild manifestations with no cosmetic or functional abnormality, surgical excision or debulking for lesions in surgically accessible locations, and systemic corticosteroids, chemotherapy or radiotherapy in patients with severe symptoms where vital organ function is compromised [9].Our patient underwent surgical removal of lesion in nose and sinus at a private practioner followed by resection from eyelid and orbit at a tertiary center whence she was lost to followup.Orbital involvement, being surgically accessible can be considered for surgical treatment,if also cosmetically distressing.Residual lesion following surgical debulking may be treated with systemic corticosteroids, chemotherapy or radiotherapy. Local recurrence responds to systemic corticosteroids. Disease involving multiple organ systems requires careful assessment,often by a team of specialists that may include a Paediatrician,Otolaryngologist, Radiologist and Surgeon besides an Ophthalmologist to plan the treatment.Prognosis is generally good anddisease is not considered fatal. In many cases, RD disease undergoes quick and complete spontaneous resolution. In cases with widespread extranodal involvementit follows a protracted clinical course for years or decades.
To conclude, a comprehensive ophthalmologist should suspect Rosai-Dorfman disease in young patients with unilateral or bilateral slowly progressive proptosis and lid mass, with or without massive cervical lymphadenopathy. Biopsy helps in confirming the diagnosis.Finally, meticulous ophthalmologic and systemic assessment for associated extranodal involvement has to be done thereby preventing wrong diagnosis and treatment.
REFRENCES
- Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy. A newly recognized benign clinicopathological entity. Arch Pathol. 1969;87:63–70.
- Vemuganti GK, Sekhar GC, Indira K. Multifocal Rosai-Dorfman disease of periorbital tissues spanning 15 Years – a case report. Orbit. 2001;20:297–300. doi: 10.1076/orbi.20.4.297.2614.
- Vemuganti GK, Naik MN, Honavar SG. Rosai dorfman disease of the orbit. Journal of Hematology and Oncology. 2008;1:7. doi:10.1186/1756-8722-1-7.
- 4. Destombes P. Adenitis with lipid excess, in children or young adults, seen in the Antilles or Mali (4 cases) Bull Soc Pathol Exot Filiales. 1965;58:1169–75.
- Foucar E, Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): review of the entity. Semin Diagn Pathol. 1990;7(1):19–73.
- Harley EH. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease) in a patient with elevated Epstein-Barr virus titers. J Natl Med Assoc. 1991;83:922–924.
- Mehraein Y, Wagner M, Remberger K, Füzesi L, Middel P, Kaptur S, Schmitt K, Meese E. Parvovirus B19 detected in Rosai-Dorfman disease in nodal and extranodal manifestations. J Clin Pathol. 2006;59:1320–6. doi: 10.1136/jcp.2005.029850.
- McClain KL, Natkunam Y, Swerdlow H. Atypical cellular disorders. Hematology Am Soc Hematol Educ Program. 2004;1:283–96.
- Komp DM. The treatment of sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease) Semin Diagn Pathol. 1990;7:83.
Leave a Comment