
Dr. Rahul Deshpande, D10304, Dr. (Col.) Madan Deshpande, Dr. Kuldeep Dole
METHODOLOGY : 1691 patients with bilateral immature cataract were included in the study.The feasibility of these IOLs was calculated by studying ocular parameters like astigmatism, angle kappa , pupil diameter using visionix VX120 and subjective characteristics like their profession and personality. Acceptability was calculated by number of patients who agreed for these IOL implantation after counselling them about the cost and visual symptoms like glare and halos. A prospective study was then conducted in hundred and forty-eight eyes of 74 patients in which multifocal IOLs were implanted. Their visual outcome was assessed using LogMAR for distance and Snellen chart for near vision, contrast sensitivity by Pelli-Robson chart and satisfaction using VF-7 questionnaire .
RESULTS:
Considering ocular and subjective characteristics,it was feasible to implant the lens in 920 patients (54.40%) and the acceptability rate was 8.04%,most common reason for decreased acceptability was cost(78.91%) of lens.The median distance UCVA at day 7 and at 4 weeks was LogMAR 0.2 (0.1-0.3) and 0.15(0.1-0.2) respectively which was statistically significant compared to preoperative distance UCVA(P<0.001).The median near UCVA at day 7 and 4 weeks was N6(N6-N8) for both,was statistically significant (P<0.001) compared to preoperative near UCVA. 93.2% patients had distance UCVA of LogMAR(0.0-0.2) and 91.8% had near UCVA of N6-N8 at 4 weeks.The contrast sensitivity was decreased in all patients but it was >1.2 in all patients.The mean preoperative VF7 score was 51.33±7.87 which improved to 88.02±7.86 at 4 weeks post-op which was statistically significant(P<0.001).
CONCLUSION:
Appropriately selected patients can achieve spectacle independence and good visual satisfaction which begins with proper patient education , lifestyle and personality dynamics and individualized weighing of benefits and side effects of multifocal IOLs .
Keywords: Multifocal IOL,contrast sensitivity, feasibility,acceptability,VF-7 satisfaction.
INTRODUCTION
Visual performance of patients who have undergone cataract extraction depends on the type of Intraocular lens(IOL)that has been implanted. The “ideal” IOL is the one which allows the patients to regain their ability to see at all distanceswithout much difficulty1.Monofocal IOLs provide excellent visual function but limited depth of focus which means that they cannot provide clear vision at both distance and near2.Recently multifocal IOLs(MFIOL)have been developed to give good unaided near, intermediate and distance vision simultaneously and reduce dependence on glasses. There are three types of multifocal IOLs available:
1) Refractive –The first multifocal IOL approved by U.S Food and Drug Administration in 1997 is Advanced Medical Optics (AMO) Array multifocal IOL which has 5 refractive zones on anterior surface: a central zone for distance correction and 4 alternating zones giving near and distance power3, but the drawback of this type of lens is that it is dependent on pupil size for its full effect.
2) Diffractive – It is based on Huygens Fresnel principle.It has pattern of rings which produces 2 primary focal points and is independent of the pupil size.
3) Apodized diffractive – it incorporates both the refractive and diffractive principles. They are designed with a soft transition (phase zones) between the“main zones’. The advantage is a significant reduction in disturbing light phenomena such as scattered light or halos. The positive spherical aberration of human cornea is corrected with an aberration correcting optic incorporated in these lenses and influence the visual acuity as well as depth of focus. Though these multifocal IOL give better near, intermediate and distance visual acuities, spectacle independence and two to threefold increase in depth of visual field, there is decrease in contrast sensitivity in addition to photic phenomena like glare and halos. The visual disturbances like photic phenomena, waxy vision, dysphotopsia ,blurred vision and excessive expectations of patients has led to dissatisfaction amongst few patients sometimes even requiring IOL explantation.4 Thus, .proper selection of the patients by assessing various anatomical and physiological ocular characteristics, individual lifestyle choices and personality dynamics before multifocal IOL implantation is important for better visual satisfaction of patients in post-operative period1.
Nowadays cataract surgery is gaining importance as a refractive surgery and we aim to give the best possible visual comfort by implantation of new intraocular lens. It is crucial to assess patients before implantation in order to decrease post-operative discomfort and the need to explant them. Thus, greater patient satisfaction levels are achieved and likelihood of legal actions or compensations is decreased. This study helps in assessing the number of patients suitable for multifocal IOL(MFIOL) implantation after proper evaluation of pre-operative ocular and personal characteristics and also study visual outcomes and satisfaction in post-operative period.
Subjects and Methods:
We prospectively examined 1691 patients with bilateral immature cataract visiting our OPD.Out of which 74 patients underwent multifocal IOL implantation after assessing feasibility and acceptability for MFIOL implantation.The inclusion criteria were all patients with bilateral senile immature cataract willing to undergo cataract surgery within a gap of 7-90 days after first eye surgery,while exclusion criteria was patients with unilateral cataract and those patients not willing to participate in study.Patients fulfilling inclusion criteria underwent feasibility assessment for implantation of MFIOL using subjective and ocular variables.
A) Subjective assessment was done by determining certain personal characteristics1 (annexure1).
B) Ocular variables included: Visual Acuity by LogMAR visual acuity chart for distance vision and near acuity chart at 33 cms and at 60 cms for near and intermediate vision respectively5.Slit lamp examination of anterior segment,grade of cataract,fundus examination,Keratometry –by Visionix VX120 machine.Optical Biometry by Lenstar LS 900 for axial length (AL), Anterior chamber depth (ACD), Lens thickness (LT).IOL formulas (SRK/T for axial length ≥ 22mm, Hoffer Q <22mm).Corneal topography byVisionix VX120 machine(astigmatism <1 D for MFIOL) Pupil size by Visionix VX 120 machine.(3.5 mm±0.8 mm for MFIOL6). Angle kappa by Visionix VX120 machine.(<70 for MFIOL7).
Those patients who were feasible for MFIOL implantation were further counselled about cost, need to undergo bilateral surgery within 90 days and about side effects of MFIOL to assess acceptability rate of these lenses,patients who accepted MFIOL underwent surgery.
SURGICAL PROCEDURE
Phacoemulsification surgery will be done either under topical or local anaesthesia. Surgery will be performed by standard operative techniques. Clear corneal 2.8 mm main port will be used to avoid conjunctival dissection.Two side ports about 0.8mm will be fashioned.
LENS USED: will depend upon patient’s choice
NEAR ADD: as per patient’s need.
OUTCOME MEASURES:
Primary measures of efficacy were uncorrected and best corrected visual activity (logMAR for distance and Snellen’s chart for near and intermediate visual acuity) was measured by 1 ophthalmologist preoperatively and at 1 week and 1 month postoperatively.
Secondary efficacy outcome were contrast sensitivity measured by Pelli-Robson chart by 1 ophthalmologist,visual function was evaluated using 7-item visual function test(VF-7)which measures difficulties in vision dependent activities of everyday life and is a modification of the VF-148.
Figure 1- showing flow chart for feasibility and acceptability assessment
STATISTICAL ANALYSIS
All statistics will be calculated using Statistical Package for the Social Sciences 20.0 for Windows software package (SPSS Inc, Chicago, IL). Continuous data will be expressed in mean +/- standard deviation and compared using student t-test or Mann-Whitney U test as appropriately required. Categorical data will be expressed in percentages and compared using Chi square test. P value of < 0.05 will be considered statistically significant.
Results: In our study, 1691 patients with B/L immature cataract feasibility was – 54.40 %(920/1691) Acceptability in 920 patients was 8.04 %(74/920).
Figure 2- feasibility rate
Figure3-acceptabilityrate
Figure 4- reasons for non-feasibility
Figure 5- reasons for non-acceptability
VISUAL ACUITY:
Table 1: showing mean uncorrected and best corrected visual acuity (near and distance).
Table 2: showing percentage of different type lens used in our study.
In majority of patients (68.9%), the type of lens used was of Diffractive type.
Figure 6- Comparison of UDVA at day 7 and day 30.
Figure7:Comparison of UNVA at day 7 and day 30
Table 3: Mean UDVA in different types of MFIOLs
Post hoc analysis using Mann-Whitney test, revealed that there was statistically significant difference in the outcome with respect postoperative distant UCVA at 30 days, between diffractive lens and Refractive lens (p=0.011). Similarly, there was statistically significant difference in the outcome with respect postoperative distant UCVA at 30 days, between Apodized diffractive lens and Refractive lens (p=0.001).
Figure 8: Comparing post-operative UDVA at day 30 between different types of MFIOLs.
Figure 9: Comparing post-operative UNVA at day 30 between different types of MFIOLs.
Table 4: Mean UNVA in different types of MFIOLs
CONTRAST SENSITIVITY:
The decreased contrast sensitivity with Multifocal IOL’s is explained by the division of the light rays into two or more foci by the IOL’s.
Contrast sensitivity using Pelli-Robson chart was > 1.2 in all patients who underwent apodized diffractive, refractive and extended depth of focus IOLs.
Figure 10: Comparing Contrast sensitivity between different types on MFIOLs at day 30.
Figure 11: VF7 score assessment at baseline against that at 30 days
(Paired t test; ***p<0.001)
Discussion:
MFIOL patients are not feasible in patients having type A personality because of hypercritical nature the visual satisfactionwill always be low, angle kappa > 70 can cause increased photic phenomenon like glare and halos 5, pupil size < 3.5 mm 6, night drivers, patients with posterior segment pathology like ARMD, glaucoma, diabetic retinopathy because real benefits of multifocality may not be produced or appreciated by them and partial contrast loss due to MFIOL may add on the visual handicap of the patient.
Acceptability was low 8.04 % primarily due to the high cost of these lenses(78.91%)comfortable wearing Near glasses -5.91%Did not want Glare halos-4.72% Not willing for bilateral cataract surgery within 90 days – 3.54% Out of 1691 only 74 patients underwent bilateral cataract surgery with MFIOL implantation Eyes with small angle kappa, a fovea centric ray may pass through the central area of MFIOL(a),while in those with higher angle kappa , a fovea centric ray may pass close to the edge of the ring ,thus causing photic-phenomena(b). (Figure 12)
Visual Outcome:
UCVA for distance at day 7 was logMAR 0-0.3 in 85.7% patients,UCVA for distance at day 30 was logMAR 0-0.3 in 93.2 % patients (p<0.001) UCVA for near at 7 day was N6-N8 in 87.2% patients, UCVA for near at day 30 was N6-N8 in 91.8% (p<0.001). The gradual improvement in vision can be attributed to the presence of inflammation immediately after surgery which eventually subsides over few days. Similar study by H.Nida Sen et al showed that Multifocal IOLs have better distance and near visual acuity and range of accommodation with decreased contrast sensitivity9 . Contrast Sensitivity:The decreased contrast sensitivity with Multifocal IOL’s is explained by the division of the light rays into two or more foci by the IOL’s Contrast sensitivity using Pelli-Robson chart was > 1.2 in all patients who underwent apodized diffractive, refractive and extended depth of focus IOLs. Similar results were found in study by Robert Montes-Mico et all which showed decrease in contrast sensitivity at near and distance2. Improvement in VF7 Score (Subjective Visual Satisfaction) Post-Operatively At Day 30. Average preoperative VF-7 score showed 72.5 % increase post operatively.
CONCLUSION:
Despite obvious advantages of multifocal practical application is limited. Meticulous pre-operative evaluation and strict selection criteria is essential before advising MFIOL. Visual outcome as well as patient satisfaction is excellent in appropriately selected patients. The final choice for a patient depends on his or her motivation to be free of spectacles guided by realistic expectations and understanding of the compromises involved.
ANNEXURE 1
PREOPERATIVELY PATIENTS WILL BE ASSESSED FOR FOLLOWING PERSONAL CHARACTERISTICS AND PRESENCE OF ANY 1 OF THEM WILL EXCLUDE THE PATIENTS FROM THE STUDY:
- Hypercritical patients with unrealistic expectations.
- Sharpest clearest vision is their main concern.
- Those with a heavy dependence on intermediate vision, night vision, or specific job require requirements (commercial pilots, public service vehicles, and taxi or truck driver).
IMPRESSION-
O SUITABLE O NOT SUITABLE
ANNEXURE 2
EVALUATION OF PATIENT SATISFACTION AFTER MFIOL IMPLANTATION BY VF-7 QUESTIONNARE15.
- How much difficulty do you have driving at night because of your vision? Do you have i)yes ii)No iii)Not applicable
-
- No difficulty
- A little difficulty
- A moderate amount of difficulty
- A great deal of difficulty
-
- Do you have any difficulty, even with glasses, reading small print, such as labels on medicine bottles, a telephone book, or food labels?i)yes ii)No iii)Not applicable
If yes, how much difficulty do you currently have?- A little
- A moderate amount
- A great deal
- Are you unable to do the activity?
- Do you have any difficulty, even with glasses, watching television?
i)Yes ii)No iii) Not applicable
If yes, how much difficulty do you currently have?- A little
- A moderate amount
- A great deal
- Are you unable to do the activity?
- Do you have any difficulty, even with glasses, seeing steps, stairs, or curbs?i)Yes ii)No iii)Not applicable
If yes, how much difficulty do you currently have?- A little
- A moderate amount
- A great deal
- Are you unable to do the activity?
- Do you have any difficulty, even with glasses, reading traffic signs, street signs, or store signs?i)Yes ii)No iii)Not applicable
If yes, how much difficulty do you currently have?- A little
- A moderate amount
- A great deal
- Are you unable to do the activity?
- Do you have any difficulty, even with glasses, cooking?
i)Yes ii)No iii)Not applicable
If yes, how much difficulty do you currently have?- A little
- A moderate amount
- A great deal
- Are you unable to do the activity?
- Do you have any difficulty, even with glasses, doing fine handwork such as sewing, knitting, or carpentry?
i)Yes ii)No iii)Not applicable
If yes, how much difficulty do you currently have?- A little
- A moderate amount
- A great deal
- Are you unable to do the activity?
REFERENCES
- Braga-Mele R, Chang D, Dewey S, Foster G, Henderson BA, Hill W, Hoffman R, Little B, Mamalis N, Oetting T, Serafano D, Talley-Rostov A, Vasavada A, Yoo S; ASCRS Cataract Clinical Committee. Multifocal intraocular lenses: relative indications and contraindications for implantation. J Cataract Refract Surg. 2014 Feb; 40(2):313-22.
- Montés-Micó R, España E, Bueno I, Charman WN, Menezo JL. Visual performance with multifocal intraocular lenses: mesopic contrast sensitivity under distance and near conditions. Ophthalmology. 2004 Jan; 111(1):85-96.
- Cillino S, Casuccio A, Di Pace F, Morreale R, Pillitteri F, Cillino G, Lodato One-year outcomes with new-generation multifocal intraocular lenses. Ophthalmology. 2008 Sep; 115(9):1508-16.
- Kamiya K, Hayashi K, Shimizu K, Negishi K, Sato M, Bissen-Miyajima H; Survey Working Group of the Japanese Society of Cataract and Refractive Surgery. Multifocal intraocular lens explantation: a case series of 50 eyes. Am J Ophthalmol. 2014 Aug; 158(2):215-220.e1.
- Blaylock JF, Si Z, Vickers C. Visual and refractive status at different focal distances after implantation of the ReSTOR multifocal intraocular lens. J Cataract Refract Surg. 2006 Sep;32(9):1464-73.
- Karhanová M, Pluháček F, Mlčák P, Vláčil O, Šín M, Marešová K. The importance of angle kappa evaluation for implantation of diffractive multifocal intra-ocular lenses using pseudophakic eye model. ActaOphthalmol. 2015 Mar;93(2):e123-8
- Alfonso JF, Fernández-Vega L, Baamonde MB, Montés-Micó R. Correlation of pupil size with visual acuity and contrast sensitivity after implantation of an apodized diffractive intraocular lens. J Cataract Refract Surg. 2007 Mar;33(3):430-
- Uusitalo RJ, Brans T, Pessi T, Tarkkanen A. Evaluating cataract surgery gains by assessing patients’ quality of life using the VF-7. J Cataract Refract Surg. 1999 Jul; 25(7):989-94.
- Sen HN, Sarikkola AU, Uusitalo RJ, Laatikainen L. Quality of vision after AMO Array multifocal intraocular lens implantation. J Cataract Refract Surg. 2004Dec;30(12):2483-93.
LEGEND:
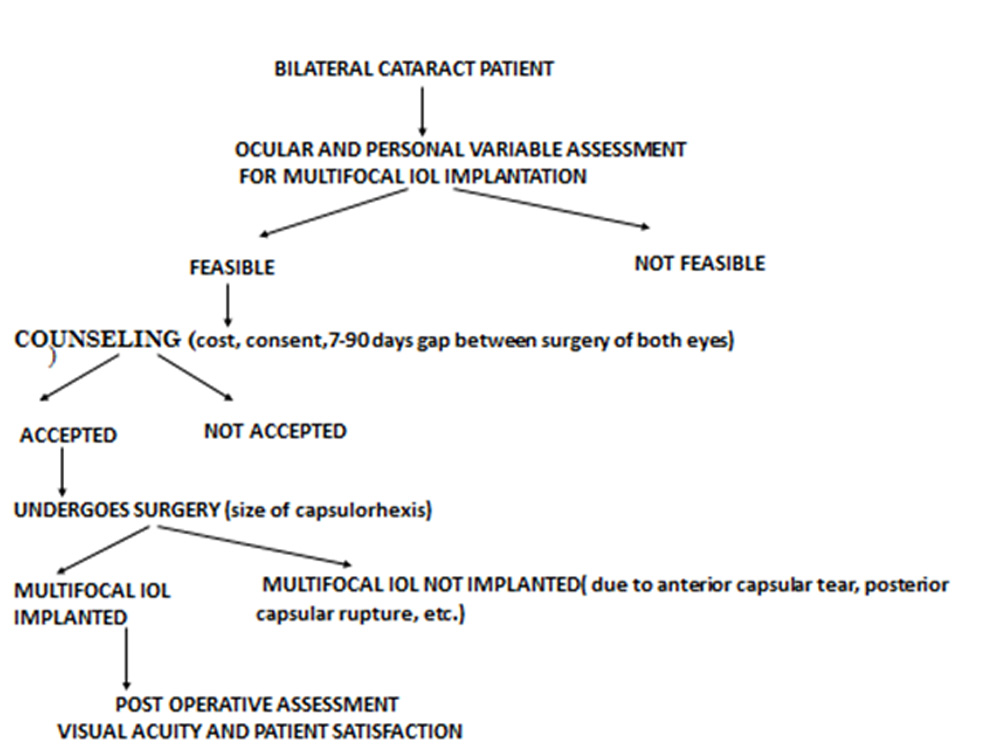
Figure 1- showing flow chart for feasibility and acceptability assessment
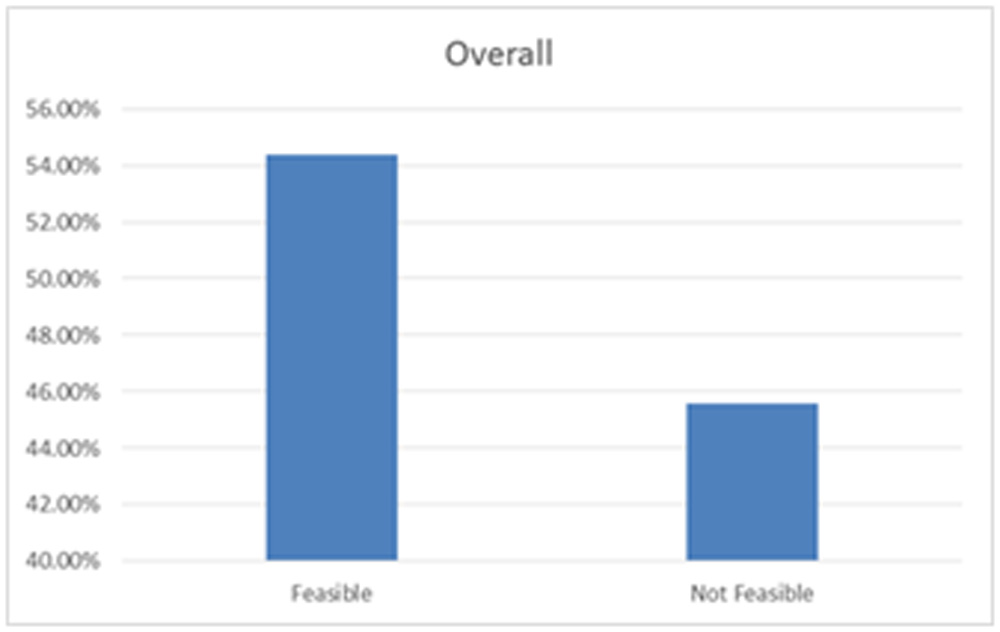
Figure 2- feasibility rate
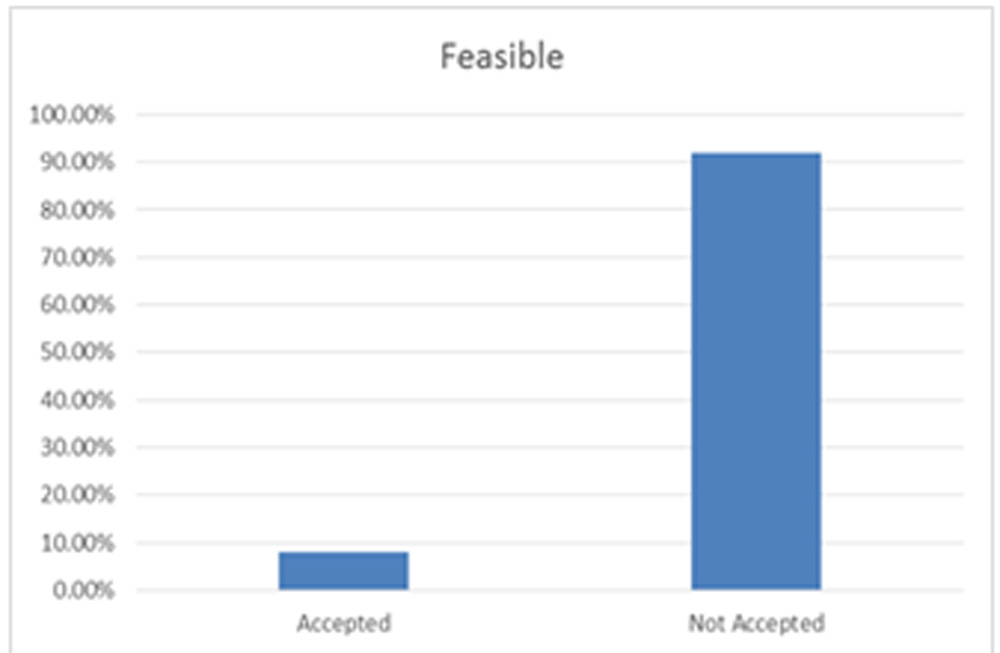
Figure 3 – Acceptability rate
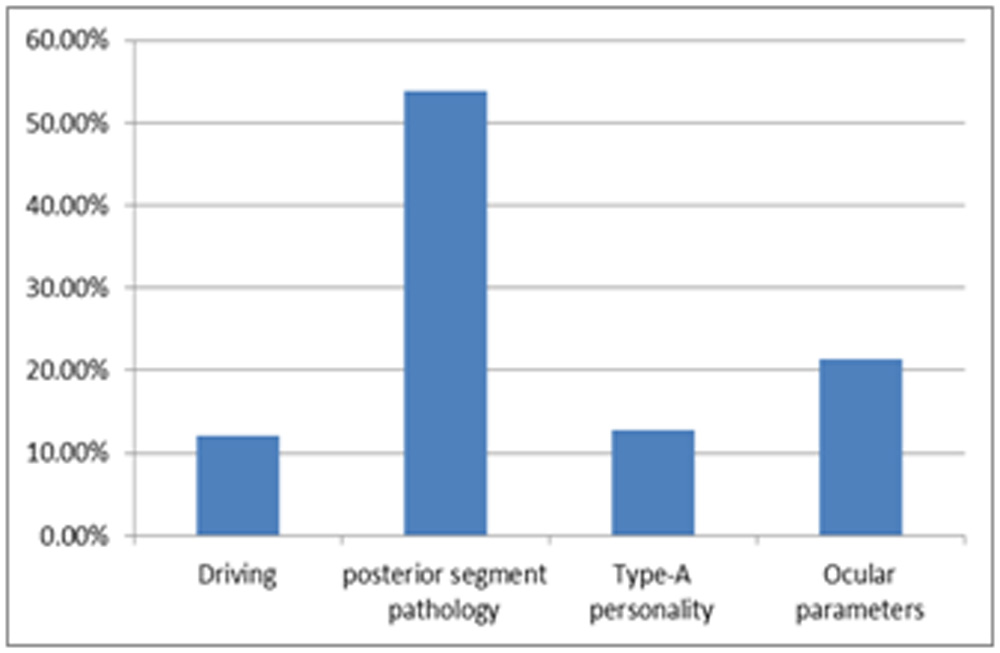
Figure 4- reasons for non- feasibility
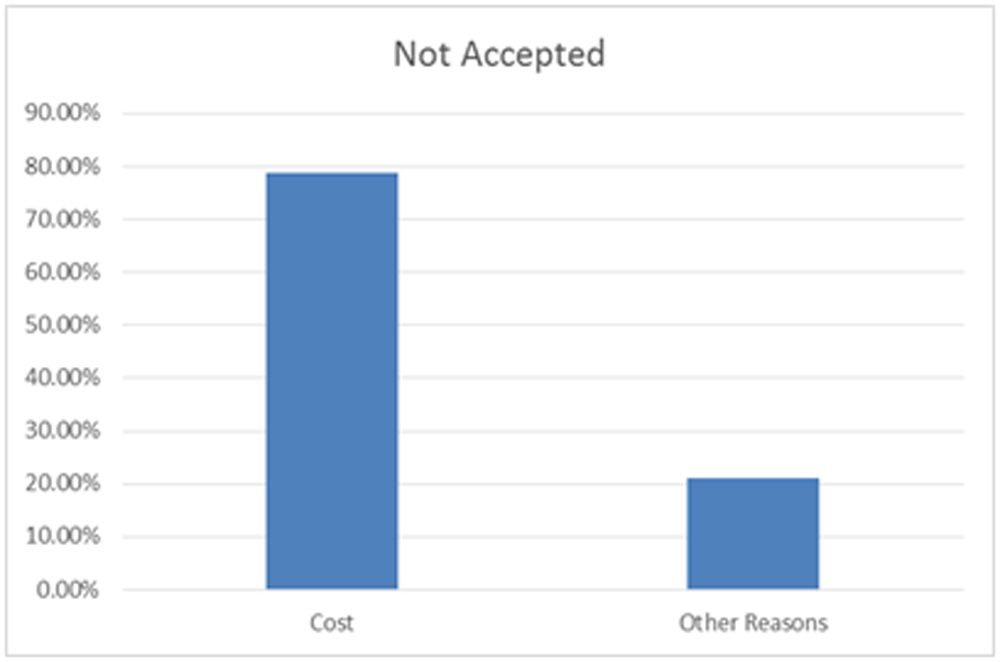
Figure 5- reasons for non-acceptability
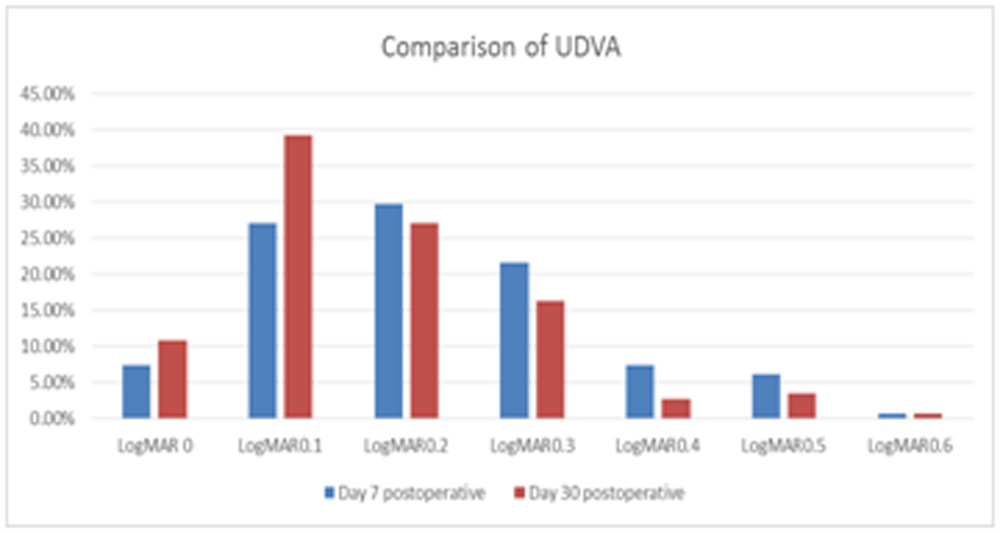
Figure 6- Comparison of UDVA at day 7 and day 30.
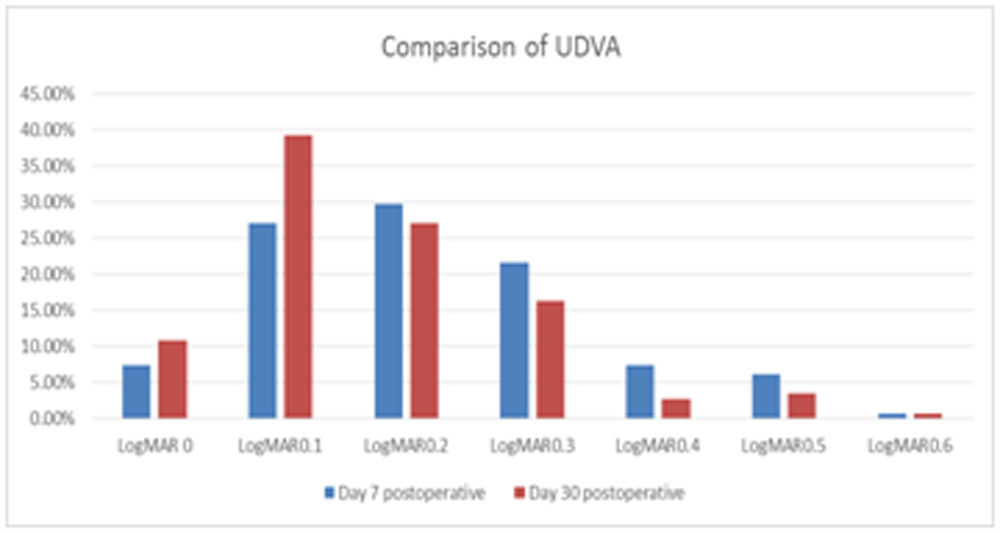
Figure 7: Comparison of UNVA at Day 7 and Day 30.
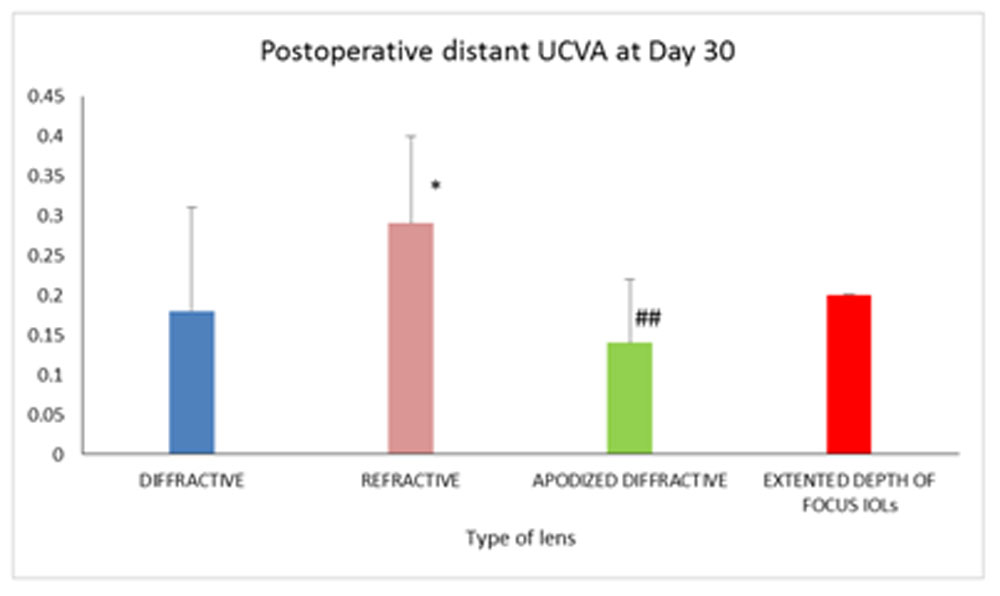
Figure 8: Comparing post-operative UDVA at day 30 between different types of MFIOLs.
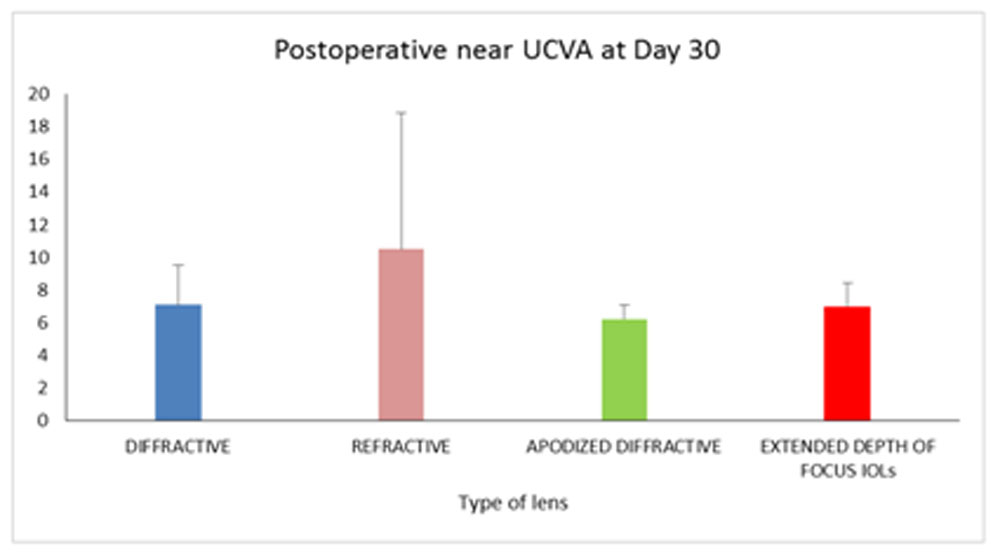
Figure 9: Comparing post-operative UNVA at day 30 between different types of MFIOLs.
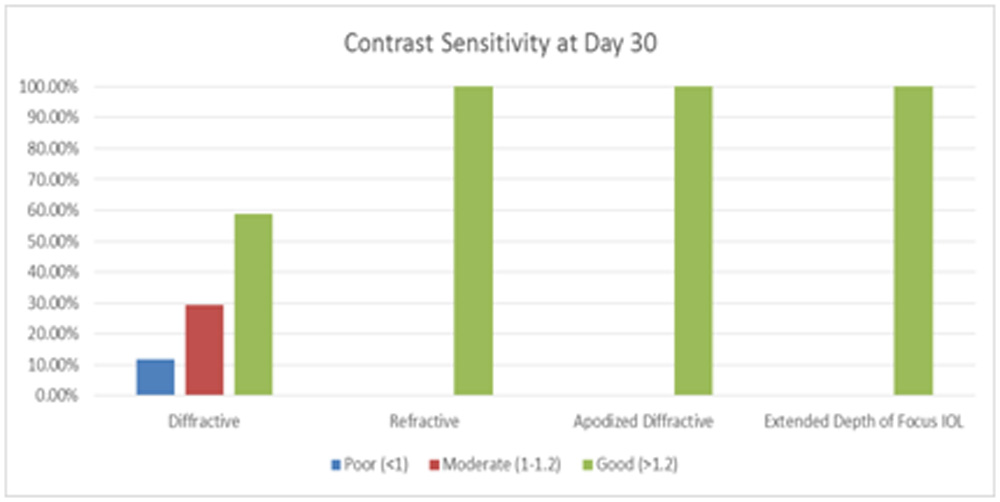
Figure 10: Comparing Contrast sensitivity between different types on MFIOLs at day 30
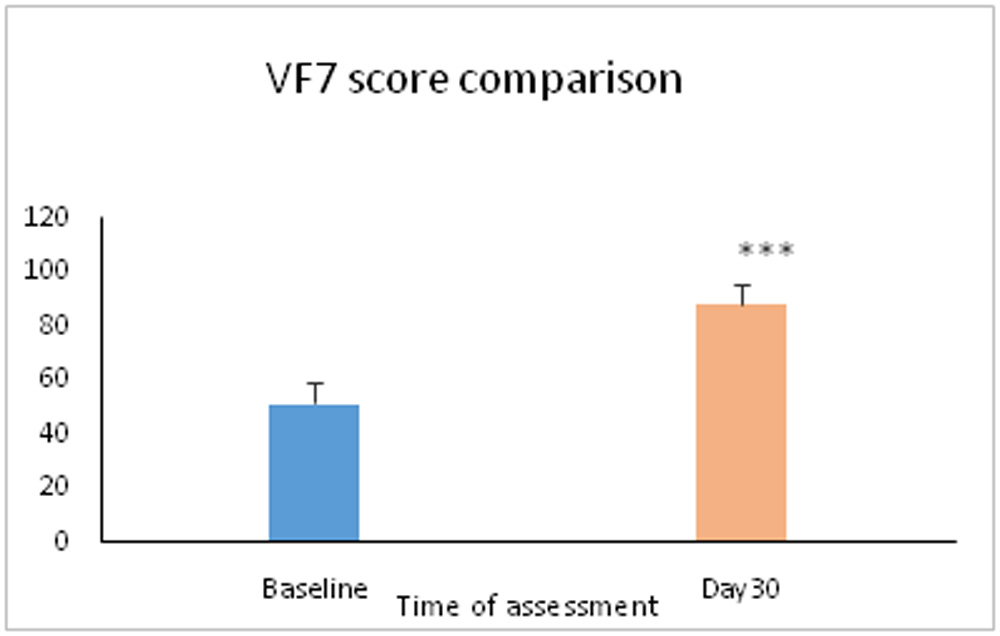
Figure 11: VF7 score assessment at baseline against that at 30 days
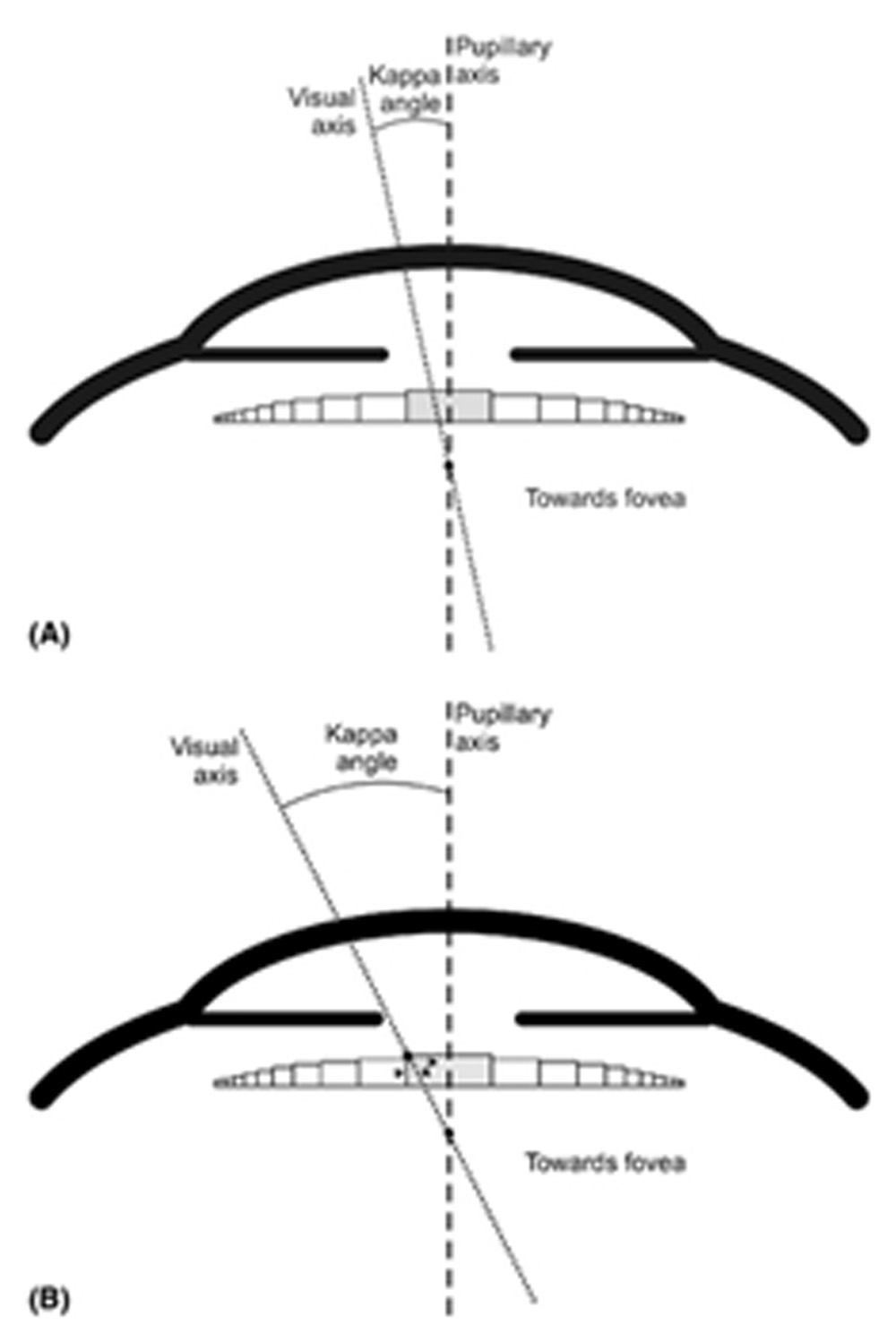
Figure 12: Role of angle kappa.
| Type of vision on Day 30 | Mean+SD | Range |
| Postoperative UCVA distance | 0.17+0.12 | 0-0.6 |
| Postoperative UCVA near | 7.07+2.91 | 6-24 |
| Postoperative BCVA distance | 0.08+0.09 | 0-0.5 |
| Postoperative BCVA near | 6.09+0.59 | 6-12 |
| Postoperative spherical equivalent (D) | -0.18+0.56 | -2.25-2.25
|
Table 1: showing mean uncorrected and best corrected visual acuity (near and distance)
| Type of lens | Frequency | Percentage |
| Diffractive | 51 | 68.9 |
| Refractive | 4 | 5.4 |
| Apodized diffractive | 36 | 24.3 |
| Extended depth of focus IOL | 2 | 1.4 |
| Total | 148 | 100 |
Table 2: showing percentage of different type lens used in our study.
| Type of IOL | Distant UCVA (Mean+SD) | Test | P value | Interpretation |
| diffractive | 0.18+0.13 | Kruskal Wallis test | 0.011
χ2(2) = 11.2 |
The postoperative distant UCVA was significantly different in groups according to type of IOL used. |
| Refractive | 0.29+0.11 | |||
| Apodized diffractive | 0.14+0.08 | |||
| Extended depth of focus IOL | 0.2+0 |
Table 3: Mean UDVA in different types of MFIOLs
| Type of IOL | Near UCVA (Mean+SD) | Test | P value | Interpretation |
| Diffractive | 7.08+2.46 | Kruskal Wallis test | 0. 11
χ2(2) = 5.98 |
The postoperative near UCVA was comparable in groups according to type of IOL used. |
| Refractive | 10.5+8.33 | |||
| Apodized diffractive | 6.23+0.85 | |||
| Extended depth of IOL | 7+1.41 |
Table 4: Mean UNVA in different types of MFIOLs
Leave a Comment