
![]()
Dr. Sunandini Bose, B16073, Dr. Gautam Singh Parmar, Dr. Ashok kumar Meena, Dr. Sachin Arya
Introduction
Peripheral ulcerative keratitis (PUK) is usually characterized by crescent shaped destructive inflammation of the juxtalimbal corneal stroma which is associated with an epithelial defect, presence of stromal inflammatory cells, and progressive stromal degradation and thinning1.PUK is often contiguous with adjacent conjunctival,episcleral, and scleral inflammation. The presence of such adjacent tissue inflammation aggravates the course of PUK and causes potentially serious complications, such as perforation of the cornea.2-4.
Local and systemic autoimmune diseases are the various etiologies to be considered and thus immunosuppressive therapy is the mainstay of treatment along with antibiotics, cycloplegic and lubricating agents. If not controlled with medical therapy, complications occurs despite the same surgical procedures may be required in the form of conjunctival resection, cyanoacrylate glue or more invasive procedures such as lamellar or penetrating keratoplasties.5-10
Irregular shape and peripheral location of such lesion pose a big challenge for ophthalmic surgeons to perform the keratoplasties in such patients. The keratoplasty options for these lesions are round or shaped grafts. The round grafts are may be eccentric and thus prone for rejection and sutures may involve optical center result in high astigmatism. To avoid visual axis suture related complications, large diameter round graft can be applied which are again prone for rejection and secondary glaucoma. There have been studies showing various round, biconvex or crescentic graft with promising results in various peripheral corneal diseases.9-11
So the choice of keratoplasty procedure for such lesions is eccentric shaped corneal grafts.
In this study, we report a novel “print & prick” technique to facilitate preparation of corneal graft in perforated peripheral ulcerative keratitis.
Methodology
A retrospectivechart review of 15 eyes of 13 patients with perforated or non-healing PUK due to any reason, who underwent a penetrating or lamellar crescentic shaped graft, was done.A minimum follow up of 3 months post keratoplastywere only included.
Patients’ demographic data were collected. Primary outcome measures were intra operative complications, graft apposition and tectonic integrity. Secondary outcome measures were visual acuity and postoperative complications.
Preoperatively, complete blood count, Mantoux test, chest X-ray, renal function test, RA factor, HbsAG,C reactive protein, sputum examination were done.Hepatic evaluation(r/o toxicity was done in subsequent follow-up visits to rule out toxicity with immunosuppressive therapy.
Patients were started on systemic immunosuppression, topical antibiotic,topical lubricants, systemic doxycycline
Preoperative evaluation and postoperative evaluation were done by a single observer (GSP).
Surgical technique
The novel “Prick and Print” technique was performed in all cases,which is a stencilling based technique in which we first performed peritomy adjacent to PUK followed by cauterisation of bleeding vessels. The outline of ulcer was marked using ink. A sterile transparent sheet of plastic from any source (drapes, suture wrappers etc.) was placed over ulcer and pricked with 26G needle along the ink marking. The sheet allowed to dry and placed over dried donor button mounted on artificial anterior chamber. The ink was applied along the pricking and imprint of the shape was made on the donor button. The donor was cut along the printed outlines partially with 15 degree lance knifeand then cut full thickness with curved Vanna’s scissors. The diseased host tissue was excised along the marking and the graft was then secured to the host with interrupted 10-0 nylon sutures.
Postoperative regime of patients comprised of topical moxifloxacin 0.5% ,topical prednisolone 1%,topical lubricants, topical cycloplegics, oral immunosuppressive and oral doxycycline.
Results
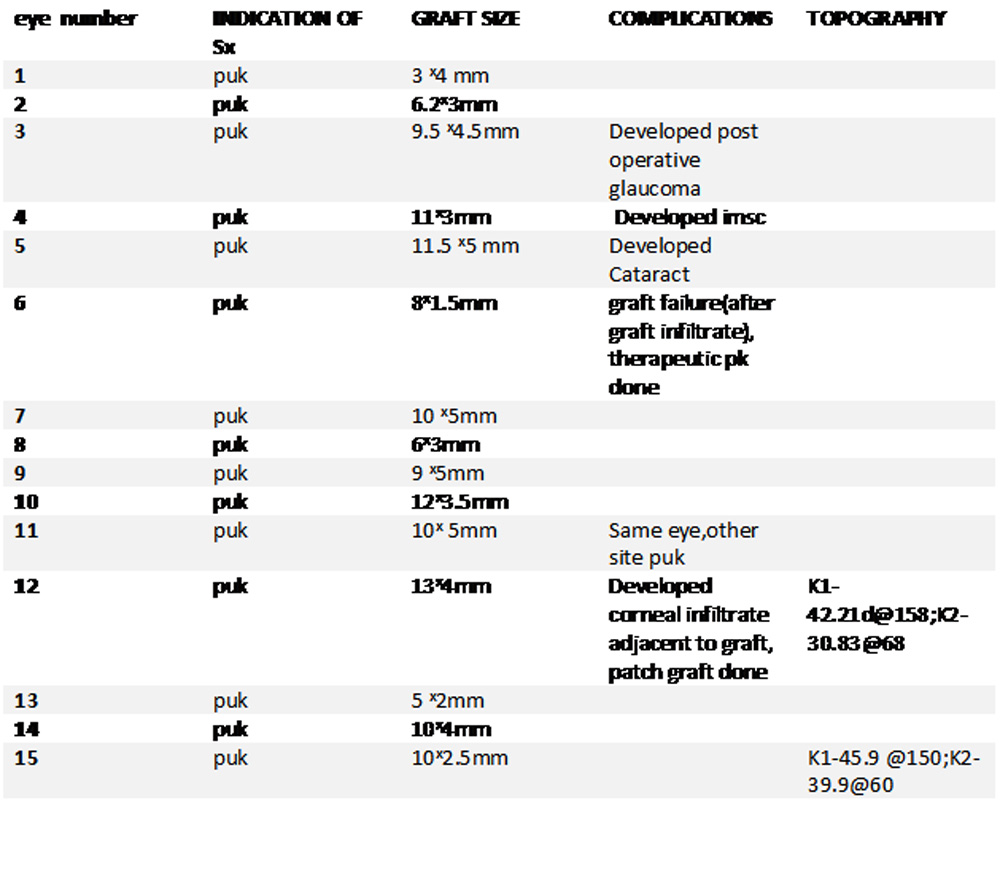
15 eyes of 13 patients underwent shaped corneal graft.The mean age of the patients was 40.61±19.44 years. The male: female ratio was 9:4. The mean follow up was 10.07 months. All surgeries were performed by a single surgeon (GSP).The demographic details, indication of surgery, graft details, results and complications are summarized in Table 1 &2
TABLE 1
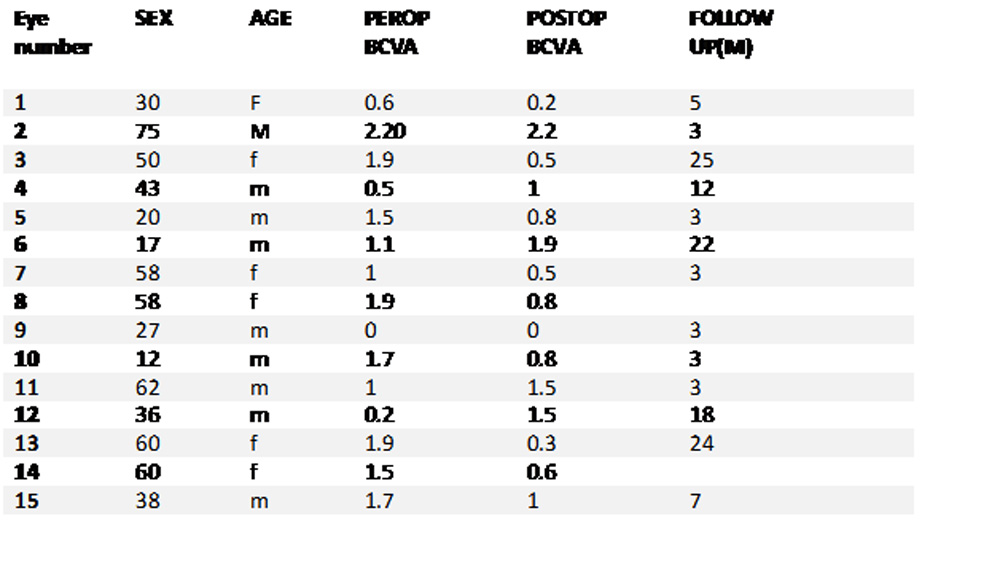 TABLE 2
TABLE 2
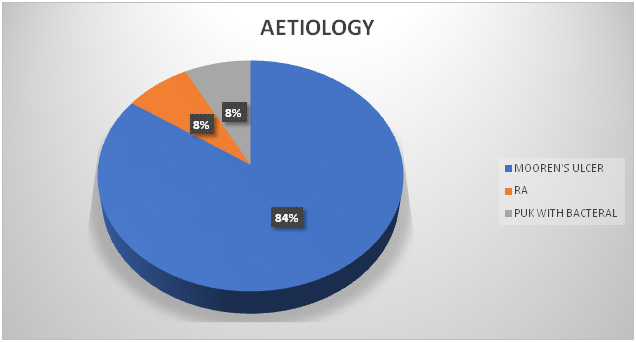
11(84.61%) patients were diagnosed with Mooren’s ulcer due to no underlying evidence of any systemic or other ocular disease and the typical clinical characteristics.While 1 (7.69%) patient met with diagnostic criteria for rheumatic arthritis,1 (7.69%) met with diagnostic criteria for peripheral corneal ulcer with bacterial involvement.
All the eyes presented with perforation of varying sizes. 2 patients underwent conjunctival resection before corneal grafting.While one eye underwent lamellar keratoplasty,14 eyes underwent penetrating keratoplasty
CHART 1
Intraoperatively there was no overriding or shortening of any graft. All sutures were of equal length and depth. There was good graft host junction apposition. Tissue gaping or flattening were not noticed.
Post operatively anatomical integrity, limbal architecture and corneal contour were well maintained in all the grafts. All eyes had well-formed anterior chamber with no leak from any graft host junction (figure 1) with excellent postoperative results.
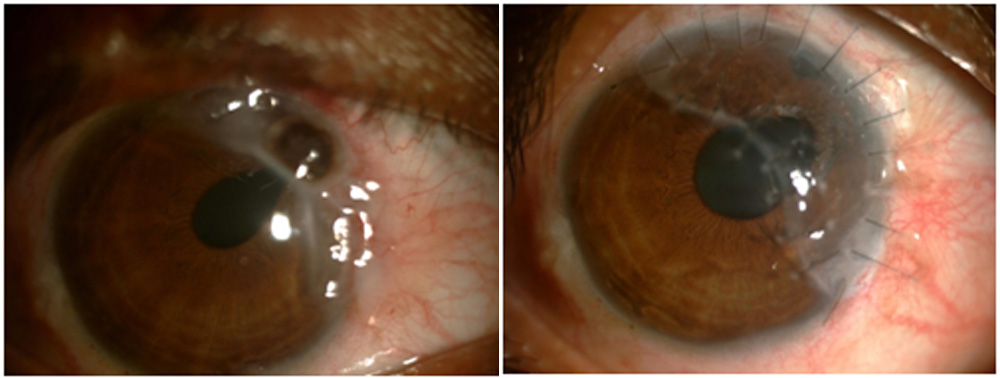
Figure 1;Pre and post operative 6 months apart;showing good maintained corneal contour,limbalarchitecture,formed anterior chamber
Postoperative vision was variable. Nine eyes experiencedimproved BCVA postoperatively, while four eyes experienced worsening of BCVA and two eyes BCVAremained unchanged.(eye number 2&9)(Chart 2,3)
CHART 2
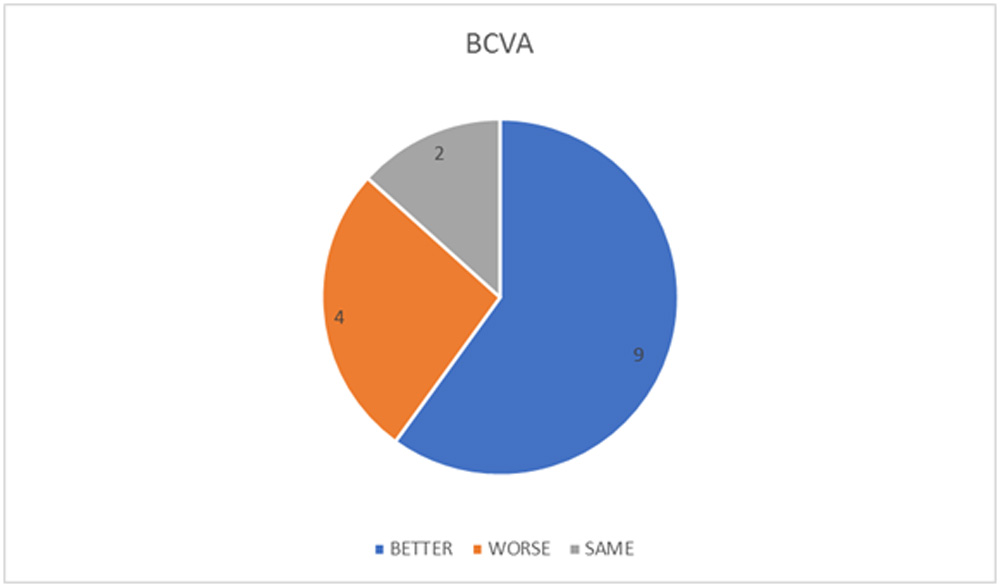
CHART 3(pre & postoperative BCVA)
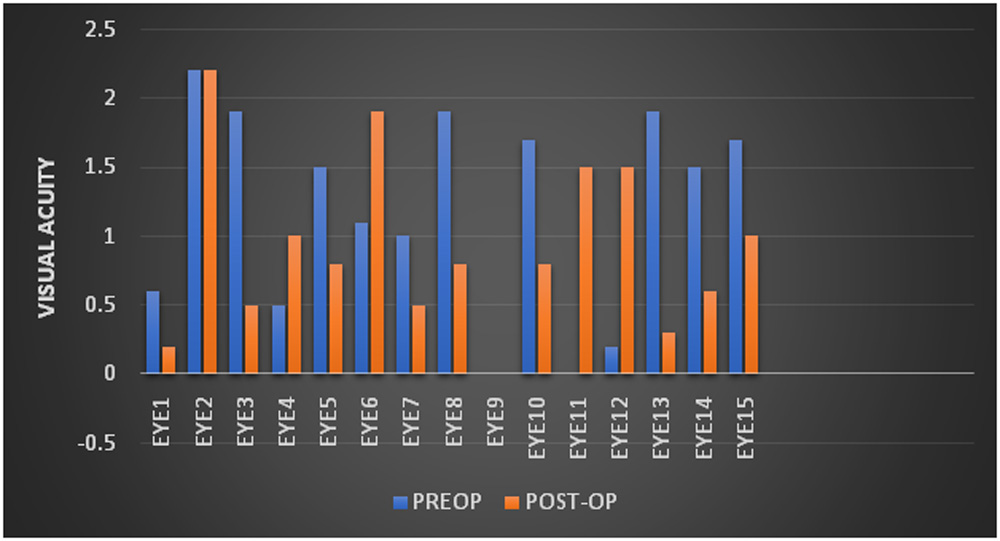
The mean BCVA changed from 1.18 Log Mar preoperatively to 0.93 Log Mar post operatively (p<0.34).
Four patients developed complications.One patientexperienced diminished vision due to development of cataract(eye number 4 ) .One patient developed PUK at other site in the same eye even with medical therapy(eye number 11). One patient developed graft infiltrate for which a patch graft was performed,but patient developed graft infiltrate again for which a repeat therapeutic penetrating keratoplasty was performed (eye number6) .One patient developed corneal ulcer at a site adjacent to the graft for which a patch graft was performed but graft melting developed for which a repeat therapeutic penetrating keratoplasty was performed (eye number 12).
DISCUSSION
Peripheral ulcerative keratitis presents with excessive tissue necrosis and involvement of the corneal limbus. Although interventional therapies with tissue adhesives as cyanoacrylate glue, conjunctival resection and amniotic membrane transplantation with systemic immunosuppression have been shown to have promising results, once perforation is present with excessive tissue necrosistectonic keratoplasty either penetrating or lamellar appears to be the best option.
Being a tertiary eye care center most of the patients that presented in our institute were on topical antibiotics and topical corticosteroids, despite this a significant number presented with perforated or impending perforation.
Although tissue adhesive can be performed in small perforation, proper sticking and tectonic stability is of great challenge in these peripheral perforations.
While a large diameter eccentric corneal graft can provide good tectonic support there are chances of sutures coming into pupillary/visual axis and more chances of graft rejection due to more area covered with grafted tissue. Small diameter round grafts have been shown to have promising results emphasizing the advantages of over large grafts, which include lower risk of graft rejection, peripheral anterior synechiae formation and secondary glaucoma, and good visual acuity despite graft failure because of eccentric location and noninvolvement of the pupillary area.11-12. When there is extensive or more clock hour involvement of limbus, a small diameter round eccentric graft will be insufficient to cover the required limbal involvement without sutures coming into the visual axis.
In such cases a customizedshaped corneal graft can be beneficial to spare as far as optical axis as possible and at same time involve more limbal clock hours in grafting.
As our primary goal was not to report better visual outcome than other techniques that have already been described but to describe a surgical technique that appears to be simpler to perform than already described technique and has good repeatability.
In previous studies by Parmar Pet al10 both biconvex and crescentic graft have been performed for various disease entities. There hasbeen use of corneal trephine to mark the corneal arc of host tissue and limbal arc was cut freehand. Also the donor tissue was cut in similar pattern with the limbal arc cut freehand after securing the graft at the host tissue limbus with two interrupted sutures. Cheng et al 13,in the management for severe astigmatism for peripheral corneal degeneration did a lamellar keratoplasty, while the donor tissue dissection was done using four corneal trephine to mark out the exact size and shape. Two corneal trephines 9mm and 14 mm were used to mark the inner and outer diameter while two trephines 2-3mm were used to mark the ends of arc.
Not only the use of multiple trephines has higher cost per case, but also the free hand dissection of the donor tissue can lead to graft host disparity and cause malapposition. In our technique the use of minimal instruments and only plastic drape makes it cost effective as well as can be performed by any beginner surgeon without the use of much surgical instruments or technical issues.
An eccentric crescentic corneal graft with the proposed technique not only ensures the limited proximity to the central optical axis but also rest of the cornea. Optical axis remains clear in case of graft failure ensuring good BCVA.Secondly, marking the exact ulcer on a surface helps in making out the exact shape and size of graft without causing any disparity. Thirdly, as the technique is similar for all cases of varying sizes and shapes , repeatability is good even with a lamellar keratoplasty. Even inexperienced surgeon can perform the technique with ease.(figure 6) Despite the marked central asymmetry caused by the eccentric graft in some cases, the surface of the central cornea may be relatively regular, allowing acceptable visual outcome.
In our study, 9 patients improved in BCVA, while 4 worsened. While two patients suffered from graft infiltrate and infiltrate adjacent to graft, one patient (eye number 12)maintained a BCVA of 20/20 prior to developing infiltrate for one-year post keratoplasty. One patient developed cataract and was satisfied with the tectonic effect of penetrating keratoplasty,but refused cataract surgery with IOL implantation. 2 eyes maintained the same BCVA, in which one patient had cataract in the eye preoperatively and refused a cataract extraction with IOL implantation.
Limitations of our study are small follow up month and unavailability of corneal topography in some patients.
Conclusion
This novel technique is simple & has good reproducibility in preparing a graft in PUK. It also provides optimum tectonic stability
References
1. Krachmer JH; PrashantGarg,Virender S. SangwanMooren’sulcer.chapter 95.Elsevier2011.
2. Galor A, Thorne JE. Scleritis and peripheral ulcerative keratitis. Rheum Dis Clin N Am. 2007;33:835–854. [PMC free article] [PubMed]
3. Odorcic S, Keystone EC, Ma JJ. Infliximab for the treatment of refractory progressive sterile peripheral ulcerative keratitis associated with late corneal perforation: 3-year follow-up. Cornea. 2009;28:89–92. [PubMed]
4. Bartly J, Mondino BJ. Inflammatory diseases of the peripheral cornea.Ophthalmology. 1988;95:463–472. [PubMed]
5. Fogle JA. Kenyon K R, Foster CS. Tissue adhesive arrests stromal melting in the human cornea.mn J Ophthalmol
6. Wagoner MD. Kenyon K R, Foster CS. Management strategies in peripheral ulcerative keratitis. IntOphthalmolClin
7. Foster CS, Forstot SL, Wilson LA. Mortality rate in rheumatoid arthritis patients developing necrotizing scleritis or peripheral ulcerative keratitis.Effects of systemic immunosuppression.Ophthahmology 1984;91: 1253—63.
8. Foster CS. Systemic immunosuppressive therapy for progressive bilateral Mooren’s ulcer. Ophthamology 1985; 92:1436-9
9. James A. Cameron; Results of Lamellar Crescentic Resection for Pellucid Marginal Corneal Degeneration . AMERICAN JOURNAL OF OPHTHALMOLOGY 113:296-302, MARCH, 1992
10. PragyaParmar, MS, Amjad Salman, MS, and Christdas A. Jesudasan, MS, FRCS .Visual Outcome and Corneal Topography After Eccentric ‘‘Shaped’’ Corneal Grafts (Cornea 2009;28:379–384)
11. Kenneth C. Chern, MD,l David M. Meisler, MD,l Steven E. Wilson, MD,l Marian S. Macsai, MD,2 Ronald H. Krasney, MD3. Small diameter, Round, Eccentric Penetrating Keratoplasties and Corneal Topographic Correlation .Ophthalmology 1997; 104:643-647.American Academy of Ophthalmology
12. Soong HK, Meyer RF, Sugar A. Small overlapping tectonic keratoplasty involving graft-host junction of penetrating keratoplasty. Am J Ophthalmol. 2000;129:465–467.
13. Ching-Li Cheng, FRCS (Ed), MMed (Ophth),1 Julian T. S. Theng, FRCS (Ed), FRCOphth,1Donald T. H. Tan, FRCS (Ed), FRCOphth1,2.Compressive C-Shaped Lamellar Keratoplasty-A SurgicalAlternative for the Management of Severe Astigmatism from Peripheral Corneal Degeneration. Ophthalmology 2005;112:425–430. American Academy of Ophthalmology.
Leave a Comment