
Dr. Manjula V, V18857, Dr. Muralidhar N S, Dr. Hemanth Murthy
Abstract
Purpose: To determine the effect of targeted retinal laser photocoagulation (TRP) in patients with macular edema (ME) in retinal vein occlusions (RVO)
Method: Retrospective analysis of 12 patients of CRVO and 16 patients of BRVO. Main outcome measures were change in BCVA and number of injections required post laser
Results: Mean age was 60 years (range of 50-75). Mean duration of follow-up was 16.5 months (range of 3-30). Mean baseline logmar BCVA for BRVO patients was 1.1 and post treatment was 0.3 (p = 0.03). Mean number of injections before laser was 3.1 and post laser 1.0 (p = 0.004). Mean baseline BCVA for CRVO patients was 1.2 while post treatment was 1.05. Mean number of injections required pre laser was 4.02 and post laser 3.5 (p= 0.06)
Conclusion: Statistically significant improvement was noted in BCVA and reduction in number of injections in the BRVO group by adding laser but no long term benefit in BCVA or reduction in number of injections obtained in the CRVO group
Key words: TRP – targeted retinal laser photocoagulation, ME – macular edema, CRVO – central retinal vein occlusion, BRVO – branch retinal vein occlusion, CNP – capillary nonperfusion, BCVA – best corrected visual acuity, VEGF – vascular endothelial growth factor
Introduction
Retinal vein occlusions are the second most common cause of vision loss after diabetic retinopathy. They can be broadly classified into central retinal (CRVO) and branch retinal vein occlusions (BRVO) depending on the site of blockage.
The predominant cause of vision loss in patients with CRVO or BRVO is macular edema. It is well established that vascular endothelial growth factor (VEGF) is an important contributor to macular edema In fact, although suppression of VEGF is highly effective in the treatment of neovascular age-related macular degeneration (AMD) and diabetic macular edema, effectiveness is probably greatest in patients with macular edema resulting from retinal vein occlusion (RVO) early in the course after occlusion.
Initially, it was believed that intravitreal injections of anti-VEGF would be needed in patients with RVO for only a relatively short period until re-canalization or collateral formation eliminated the need for treatment; however, long-term follow-up demonstrated that this was not the case.
In the RETAIN (Extended follow up of patients with macular edema due to bRanch rETinal vein cclusion or centrAl retinal veIn occlusioN previously treated with intravitreal ranibizumab) study (5), with a mean follow up of 49 months, 14 of 32 CRVO patients (44%) and 17 of 34 BRVO patients (50%) had edema resolution and no longer required ranibizumab injections.
Targeted retinal laser photocoagulation can ablate nonperfused retina and potentially decrease the production of VEGF within the eye. This offers the theoretical possibility of decreasing the VEGF load. This may have two possible consequences. The first is with less VEGF being produced, it is possible that the injection frequency may be reduced. The second possibility is that with the decreased production of VEGF, the macula may experience less severe attacks of edema and function better as a consequence.
In this study, we analysed whether targeted laser photocoagulation reduces the need for anti-VEGF injections and improves outcomes in patients with RVO
Methods: Data of 16 patients of BRVO and 12 patients of CRVO with macular edema were analysed.
Eligibility criteria:
- Ischemic central or branch RVO
- Best-corrected visual acuity (BCVA) 2/60 to 6/12 Snellen equivalent
- 2 consecutive monthly anti-VEGF injections with recurrent CME
- CNP on fluorescein angiography outside of the macula amenable to TRP
- All patients received 0.05 ml intravitreal injection of 0.3 mg ranibizumab/1.25mg of bevacizumab on pro re nata (PRN) regimen in the presence of intraretinal or subretinal fluid on OCT and decrease in BCVA. Fundus fluorescein angiography was done to assess the extent of retinal ischemia. TRP was applied to areas of CNP outside the macula. Laser was applied in a single session in patients with BRVO and in 2-3 sessions in the CRVO group. Spacing between spots was 1.0 spot diameter.
Results: Mean age was 60 years (range of 50-75). Mean duration of follow-up was 18 months (range of 6-30).
In the BRVO group, 5 patients did not require any injection post laser. 8 patients stabilized after 1-3 PRN antiVEGF injections. 3 patients are still under treatment because of recurring macular edema even though the retreatment frequency is less. There was no change in the retreatment frequency in the CRVO group post laser.
Mean baseline logmar BCVA for BRVO patients was 1.1 and post treatment was 0.3 (p = 0.03, statistically significant). Mean number of injections before laser was 3.1 and post laser 1.0 (p = 0.004, statistically significant).
Mean baseline BCVA for CRVO patients was 1.2 while post treatment was 1.05 (p = 0.4). Mean number of injections required pre laser was 4.02 and post laser 3.5 (p= 0.06), both are statistically not significant.
BCVA 6/60
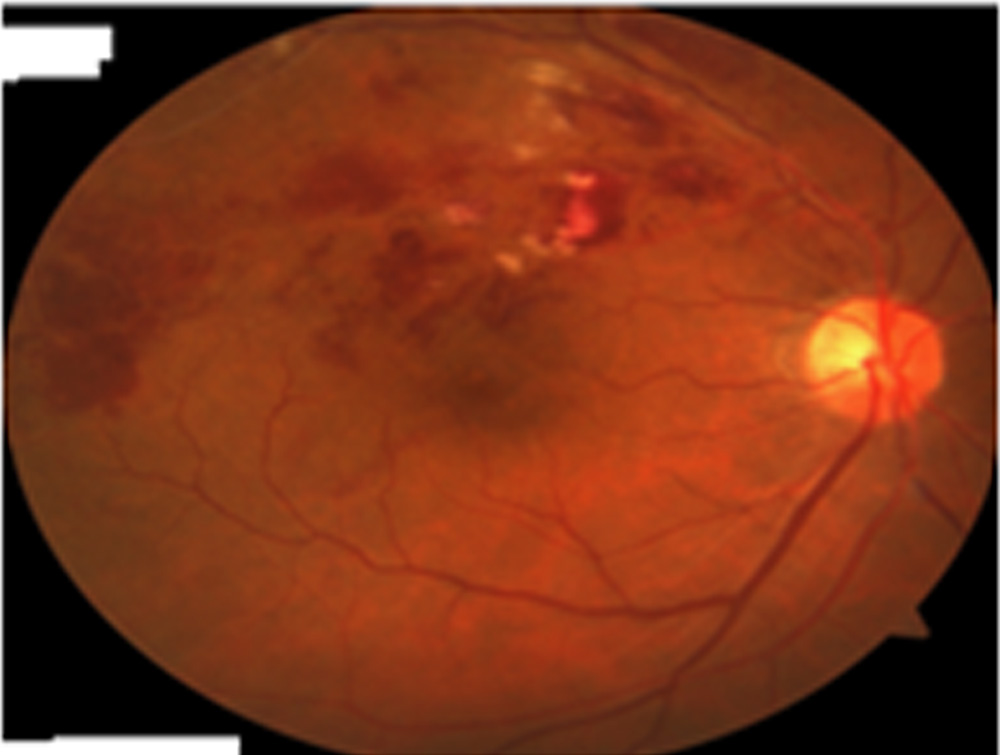
Figure 1: Colour fundus photograph of a 65 year old gentleman, showing superotemporal BRVO

Figure 2: OCT of the same patient showing cystoids macular edema
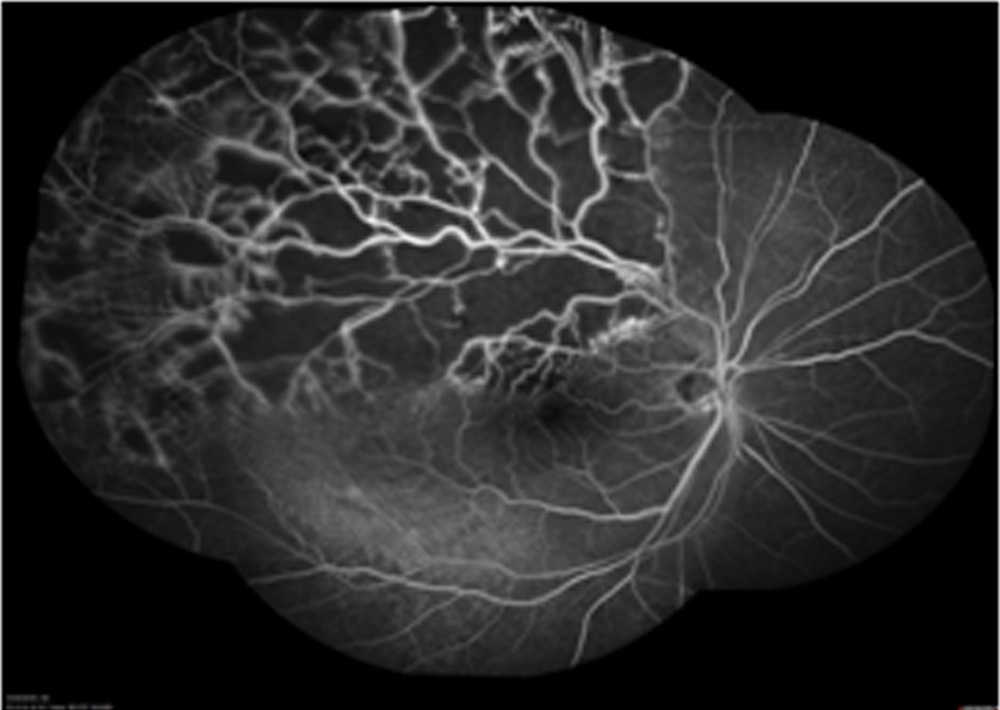
Figure 3: FFA showing significant CNP areas in the superotemporal quadrant
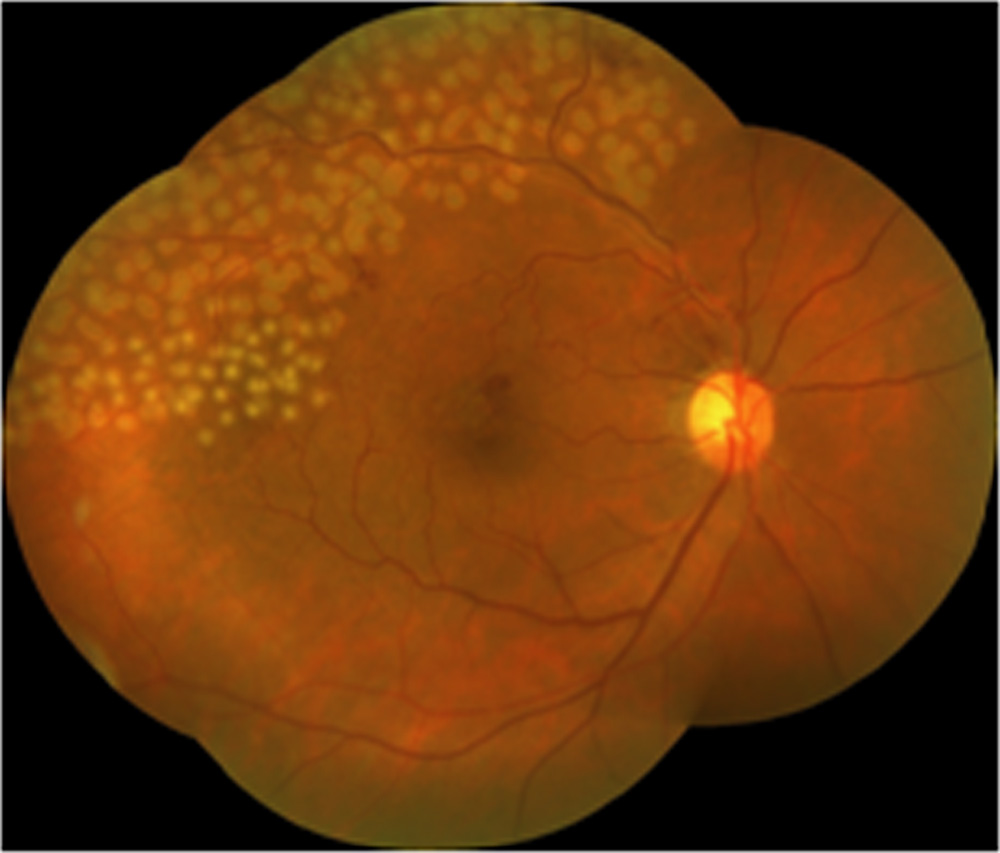
Figure 4: Colour fundus photograph of the same patient showing the area covered with laser
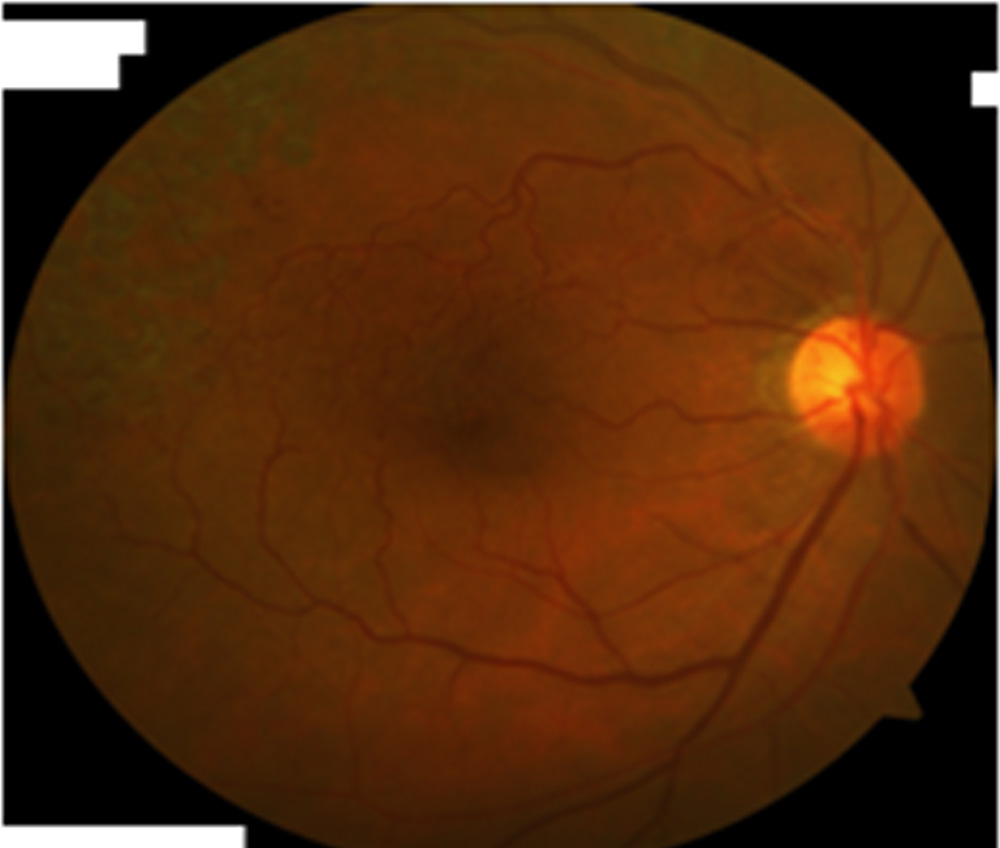
Figure 5: Colour fundus photograph after 6 months post laser and last PRN injection. BCVA 6/9. Macula dry
Comparison of BCVA pre and post laser
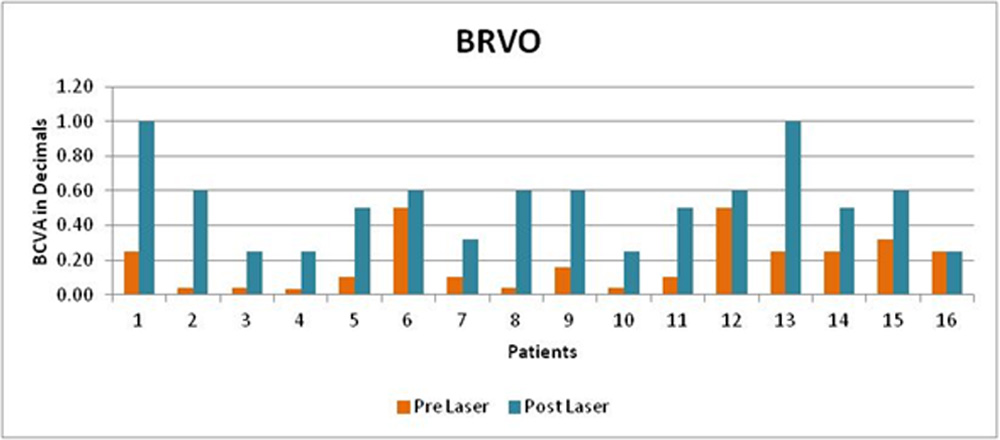
p = 0.03 (statistically significant)
Comparison of BCVA pre and post laser
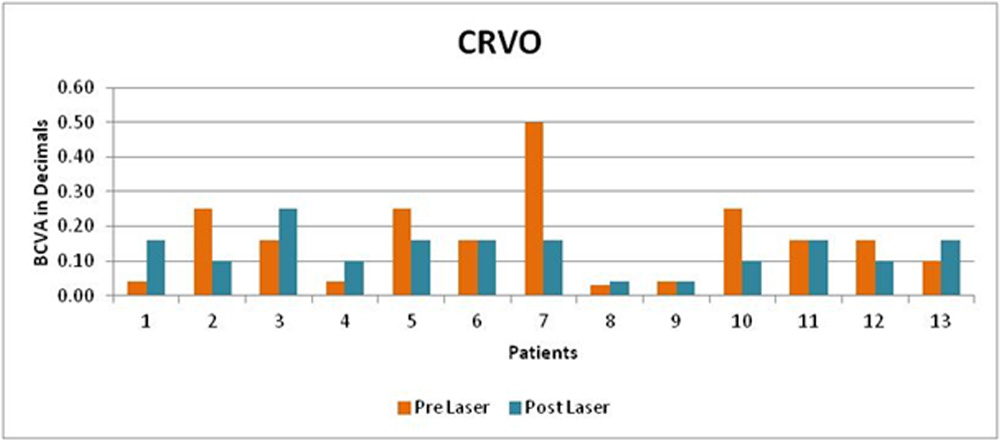
p = 0.4 (statistically not significant)
Comparison of number of injections pre and post laser
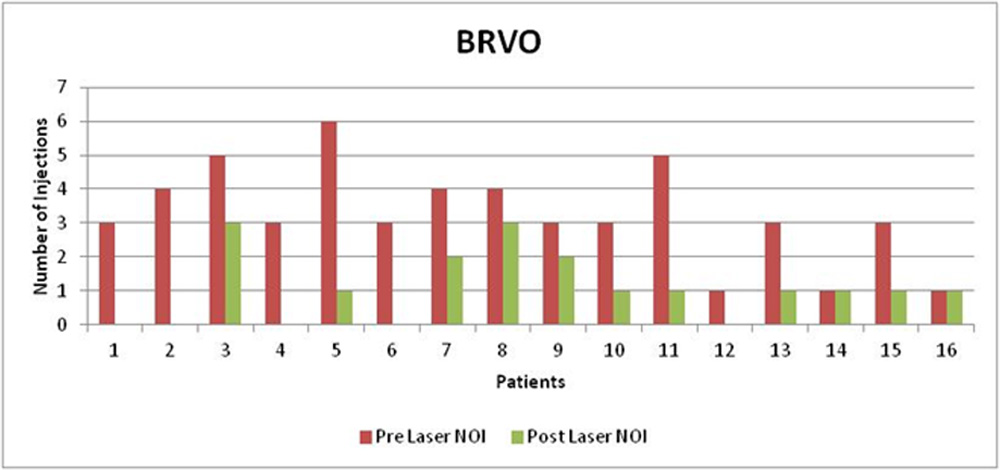
p = 0.004 (statistically significant)
Comparison of number of injections pre and post laser
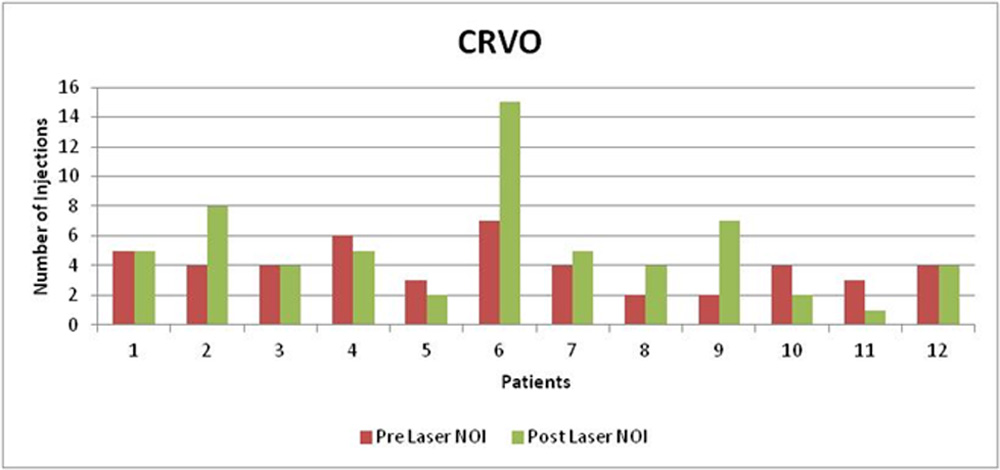
p = 0.06 (statistically not significant)
Discussion: Hypoxia causes increased expression of VEGF which is a potent inducer of vascular permeability that has been shown to cause vascular leakage. While intravitreal anti-VEGFs rapidly improve macular thickening, repeated injections are often required to maintain the initial effect. The transient nature of the effect may be explained by the relatively short intravitreal halflife of anti-VEGFs, which results in a rapid decrease in the intra-ocular concentration.
In addition, it is also possible that ischemic areas of the peripheral retina release VEGF continuously after injection of anti-VEGFs. Even if intraocular VEGF levels were reduced by them with amelioration of ME, it could recur if ischemic areas of the retina continue to produce VEGF and leakage from retinal vessels continues.
Several trials(3,4) have investigated the efficacy and safety of targeted laser photocoagulation in reducing treatment burden in RVO patients. Both Wave (1) and Relate (2) trials demonstrated that peripheral photocoagulation did not appear to decrease the treatment burden.
In Relate trial (2), laser was applied in multiple sessions where the areas of the retina that were not treated with laser were hypoxic and secreted sufficient VEGF to cause recurrent and persistent leakage.
Limitations of this study are retrospective nature, lack of control group and small sample size.
Conclusion: In our analysis, targeted retinal laser photocoagulation showed statistically significant improvement in BCVA and reduced number of PRN injections in the BRVO group. There was no significant difference in BCVA or number of PRN injections in the CRVO group. No initial exacerbation of macular edema or decline in BCVA was observed in both the groups immediately after laser.
References:
Wycoff CC, Ou WC, Wang R, Brown DM, Sadda SR, Wang K, Zamora D
Peripheral Laser for Recalcitrant Macular Edema Owing to Retinal Vein Occlusion: The WAVE Trial
Ophthalmology 2017: 124(6)
Peter A. Campochiaro, MD, Gulnar Hafiz, MD, Tahreem A. Mir, MD, Adrienne Scott, MD, Sharon Solomon, MD, Ingrid Zimmer-Galler, MD, Akrit Sodhi, MD, PhD, Elia Duh, MD, Howard Ying, MD, PhD, Adam Wenick, MD, PhD, Syed Mahmood Shah, MD, Diana V. Do, MD, Quan D. Nguyen, MD, Saleema Kherani, MD, Raafay Sophie, MD
Scatter Photocoagulation Does Not Reduce Macular Edema or Treatment Burden in Patients with Retinal Vein Occlusion: The RELATE Trial
Ophthalmology 2015;122:1426-1437
Spaide RF
Prospective study of peripheral panretinal photocoagulation of areas of nonperfusion in central retinal vein occlusion
Retina 2013; 33: 56 – 62
Yoko Tomomatsu, Takeshi Tomomatsu, Yoshihiro Takamura, Makoto Gozawa, Shogo Arimura, Yuji Takihara and Masaru Inatani Department of Ophthalmology, Faculty of Medical Sciences, University of Fukui, Yoshida-Gun, Fukui-Ken, Japan
Comparative study of combined bevacizumab/ targeted photocoagulation vs bevacizumab alone for macular oedema in ischaemic branch retinal vein occlusions
Acta ophthalmologica 2016; 94(3)
Campochiaro PA, Sophie R, Pearlman J, et al.
Long-term outcomes in patients with retinal vein occlusion treated with ranibizumab: the RETAINstudy.
Ophthalmology 2014;121:209–19.
Leave a Comment