
Dr. Kamalakannan Damodaran, D20046, Dr. Rathinam Sivakumar R
INTRODUCTION: Acute retinal necrosis (ARN) is distinct ocular inflammatory condition, with constellation of clinical features and vision threatening complications. Acute retinal necrosis is visually devastating disease, prompt diagnosis and good therapeutic approach is a must for better visual recovery. Akira urayama et al [1]in the year 1971, reported six cases of a unique form of uveitis that had not been described before. They named this clinical entity as “kirisawa uveitis” after their professor Nagamori kirisawa. There report was the first documentation of ARN syndrome. The first international literature on acute retinal necrosis was by Willerson et al [2]in American journal of ophthalmology in the year 1977. The term bilateral acute retinal necrosis (BARN) was coined by Young and Bird[3] in the year 1978. Culbertson et al[4] in 1982 demonstrated presence of herpes virus in an enucleated eye of an ARN patient by electron microscopy, in the year 1986. Varicella zoster was cultured from ARN patient. In 1994 American uveitis society proposed a diagnostic criteria[5] for ARN syndrome.
STANDARD DIAGNOSTIC CRIETERIA FOR ACUTE REINAL NECROSIS[5]
The American uveitis society recommended diagnostic criteria to be used for all clinical and laboratory studies in acute retinal necrosis in the year 1994.
- Focal, well demarcated areas of retinal necrosis located in the peripheral retina (outside the major temporal vascular arcade).
- Rapid, circumferential progression of necrosis ( if antiviral therapy has not administered)
- Presence of evidence of occlusive vasculopathy
- Prominent inflammatory reaction in vitreous and anterior chamber
Characteristics that supports but not required for diagnosis are 1.optic atrophy 2.scleritis 3.pain.
ARN was first reported in Japan, now reported throughout the world. ARN affect both gender, but has slight male preponderance. Acute retinal necrosis affects all age group, a bimodal distribution in age exist which peaks at 16-25 and 45-65 age groups. Bilateral involvement occurs in one third of patients, usually fellow eye involvement occurs between 1-6 weeks. A delay of several weeks to years had been reported in manifestation to occur in fellow eye.
The main etiological factor for acute retinal necrosis is the herpes family virus of which alpha herpes virus Herpes simplex virus 1 (HSV1), Herpes simplex virus 2 (HSV2) and Varicella zoster (VZV) causes ARN most commonly. Rarely Epstein barr virus (EBV) and Cytomegalovirus (CMV) implicated to cause ARN. ARN may be a result of a dormant HSV1, HSV2 or VZV viral reactivation in retina. Since the causative viruses are neurotropic, the probable route for reaching the retina is to travel down the optic nerve. Alternatively, one of other cranial nerves supplying the eye may transport the virus. The exact etiology of this reactivation still remain elusive, however an immuno genetic predisposition to the disease is likely. HSV1, HSV2 and VZV were found in ocular samples in high copy numbers suggesting active viral replication in patients with ARN. Evidence suggests that primary viral infection, in addition to a secondary reactivation, can cause ARN, I such cases virus can reach through haemtogenous route, with infected lymphocytes enabling the virus to cross blood retinal barrier.
CLINICAL FEATURES
At presentation, a patient with ARN typically complains of ocular or periocular pain mild to moderate grade. Irritation, foreign body sensation, usually associated with red eye. Pain is worse with ocular movement due to coexisting myositis and optic neuritis. In some patients pain, redness and photophobia is absent. Hazy vision, floaters and occasionally decreased peripheral vision seen in early course of the disease. Central vision loss is rare, seen as a result of centre involving retinal detachment and optic neuritis.
During active disease mild to moderate conjunctival injection with cilliary flush is noted. Chemosis, lid edema, subconjunctival haemorrhage and even mild proptosis may been seen. Diffuse episcleritis , scleritis can develop. . Mild to moderate anterior chamber reaction with fine or Granulomatous keratic precipitates are seen. In ARN intraocular pressure (IOP) is frequently elevated. Alternatively, IOP may be reduced in ARN patients with chronic retinal detachment(RD). iris neovascularisation may occur due to chronic retinal detachment. Cataract may occur mainly a posterior sub capsular cataract.
The triads of posterior segment findings are retinal and choroidal vasculitis, retinal necrosis and vitritis. Retinal vasculitis typically affect the arteries and is severe and oblitrative in nature. Retinal necrosis appears ophthalmoscopically as confluent area of retinal whitening as small patches, broad zones of retinal necrosis are termed as “thumbprints”. The border between necrotic and normal retina tends to appear quite well defined, smooth and geographic. There is prefference for peripheral retina initially, with spread to macula occurring late, if at all, in the course of disease. Several noncontiguous patches of necrosis, each involving between one half to four clock hours of retina, in other instance the entire360 degrees peripheral retina is affected. As the disease progress the patches of retinal necrosis coalesce into broad geographic area. As a result visualization of posterior segment can be difficult at this stage. Severe vitreous fibrosis with traction resembling proliferative vitreoretinopathy is a common late complication.
Other posterior segment findings with ARN include optic disc swelling, branch arterial or venous obstruction can be seen at any point in the clinical course, secondary to severe vasculitis. Macular edema is reported to occur. ARN optic neuritis is heralded by optic disc edema, associated with decreased central vision. Along with presumed direct viral infection of the neural cells of the optic nerve as well as marked secondary ischemic necrosis due to widespread intra neural vasculitis, it is suggested that loculated exudates within the optic nerve sheath may cause central vision loss in ARN. Typical optic neuritis due to ARN have swollen disc, acquired dyschromatopsia, a relative afferent papillary defect, central or arcuate field defect enlargement of optic nerve sheath. Retinal detachment corresponding to the site of necrosis occurs at a very high rate, ranging from 50% to 75% during the course of the disease. Necrotic retina is very thin with extremely weak adhesion and highly prone to tear in the area between the healthy posterior retina and necrotic peripheral retina.
ASSOCIATED SYSTEMIC FINDINGS
ARN has close temporal association with herpes zoster skin infections, herpes simplex ulcer. Concurrent aphthous ulcer reported in few patients. ARN may be accompanied with low grade fever, head ache, sinus pain and neck stiffness. CSF analysis revealed pleocylosis. Following ARN labyrinthine deafness and diffuse cerebral atrophy had been reported. In light of this ARN is termed as “ uveo-meningeal syndrome”. Immunosuppressed patient present with concurrent viral encephalitis with ARN.
INVESTIGATIONS
PCR has proven to be a valuable test for diagnosis of ARN, PCR can be done with aqueous humour by anterior chamber paracentesis, vitreous sampling can be obtained by vitreous aspirate or by vitreous biopsy using vitreous cutter. PCR analysis can also be used for monitoring disease course and assessing response to therapy. PCR analysis of ocular fluid can also be supplemented with calculation of a Goldmann-Witmer coefficient (GWC) in the diagnosis of ARN. Nested PCR is highly sensitive, as small amount of targets are detected using 2 sets of primers. A double amplification process is used in this method. First set of primer is used for amplification, the product of this PCR is subjected to another PCR with second set of primer. The second primer used are specific to an internally amplified sequence to the first PCR, there by increasing the specificity of the test.
Ultrasonography (USG B scan) is very useful for detecting the presence of retinal detachment when the degree of vitritis hinders ophthalmoscopic examination of the posterior segment. Fundus photography is very important in documentation of ARN. Serial Fundus photography helps to assess treatment outcome. Spectral domain (SD-OCT) or swept source (SS-OCT) helps to understand the functional consequence of ARN may be useful to monitor early sign of retinal detachment and to monitor macular involvement [6].
TREATMENT
In the years following the initial break through linking herpes virus to ARN antiviral agents became the main stay of treatment along with adjutants like oral and topical corticosteroids, anticoagulants and topical cycloplegics.
The standard of antiviral therapy is intravenous (iv) administration of acyclovir, newer oral antiviral agents are emerging as alternatives to high-dose intravenous acyclovir, avoiding the need for invasive and as an inpatient treatment. . Combined oral and intravitreal antiviral therapy is gaining popularity. Drug resistant is uncommon and also be difficult to identify. Antiviral drugs have few side effects, but special attention needs to be paid to patient who have underlying renal disease, in pregnant and in immunocompromised patients.
The exact duration of treatment is still not conclusive. Newer methods, such as quantitative assays for viral DNA, may provide additional information and guide treatment in future.[7]
ACYCLOVIR:
The antiviral effect of acyclovir was first described in 1977,The affinity for acyclovir for virus specific thymidine kinase is approximately 200 times greater than for cellular thyamidine kinase. . Acyclovir triphosphate inhibit viral replication by acting as a competitive inhibitor for viral DNA polymerase, which ultimately get incorporated in viral DNA chain and result in obligate chain termination. Gastrointestinal absorption is slow, highly variable and incomplete. Oral bioavailability is 15% to 30%. Peak plasma concentration of acyclovir is 1.5times to 2.5 hours after oral administration and short plasma half life of 3 hours which necessitates frequent (5 times per day) dosing. The plasma concentration of 10-20microgram/ml can be achieved by intravenous (iv) administration of acyclovir of 5-10mg/ml, regular oral dose of 200-800mg yield 0.6-1.6microgram/ml. acyclovir is metabolized by liver and excreted by kidney. 15% of acyclovir is protein bound.
Acyclovir is highly sensitive to herpes simplex virus. Intermediately sensitive to Varicella zoster and EBV, acyclovir is least sensitive to CMV.
VALACYCLOVIR:
Valacyclovir is the oral prodrug of acyclovir and has the same mode of action as acyclovir. Valacyclovir, the L-valyl ester of acyclovir, create a substrate for active transport in human intestine. After absorption valacyclovir under goes rapid and complete first pass metabolism in the intestine and liver to form acyclovir and essential aminoacid L-valine. This process is cytochrome P450 independent. Increase uptake and rapid hydrolysis of valacyclovir to acyclovir results in significant greater systemic levels of acyclovir following oral valacyclovir ingestion compared with oral acyclovir. It had been found 3-5 fold increase in bioavailability of valacyclovir compared to oral acyclovir. Administration of valacyclovir 250mg 4 times daily results in acyclovir Cmax and area under the concentration- time curve (AUC) values comparable to oral acyclovir 800mg 5times daily. Daily acyclovir AUC for valacyclovir at a dose of 1000mg 3 times are similar to those obtained with intravenous acyclovir 5mg/kg administration 3times/day. Valacyclovir 2000mg 4times daily produce a daily 109microgram/hour/ml of AUC which is similar to AUC achieved by iv acyclovir 10mg/kg 3 times daily (107microgram/hour/ml)[7].
GANCYCLOVIR:
Gancyclovir is a synthetic nucleoside analogue of guanine which inhibits the precipitation of herpes virus both in-vivo and in-vitro. Intracellular gancyclovir is
phosphorylated to gancyclovir triphosphate. Gancyclovir triphosphate is 100 times more concentrated in CMV infected cells than non infected cells. After, one hour iv injection of 5mg/kg gancyclovir sodium, total gancyclovir AUC 26.8microgram/kg/ml and Cmax 9.0microgram/ml. intravitreal dose of gancyclovir 2000microgram in 0.1ml.Compared to acyclovir, gancyclovir has similar activity against HSV and VZV. The enhanced anti CMV activity is due to the lack of a hydroxyl group on the acyclic side chain.[8]
Early intravitreal injection with gancyclovir can yield satisfactory therapeutic effect and better visual acuity if applied before occurrence of retinal detachment.[9]
COMPLICATION
The ocular inflammation associated with the ARN syndrome is generally a self limiting process. Without treatment, the active posterior segment inflammation eventually subsides. The host immune response controls the infecting virus. One feature of ARN syndrome that sets it apart from other infectious and inflammatory retinal condition is frequent development of full thickness retinal hole. Most observers note that retinal holes in ARN develop at the junction of normal and affected retina. Retinal tears accompanied by vitreous fibrosis and traction lead to rhegmentogenous retinal detachment and proliferative vitreoretinopathy in 75% of ARN patients.
Retinal detachment accounts for the bulk of ocular morbidity associated with the ARN syndrome. As retinal tears do not form during active inflammation, retinal detachment occurs between 6-12 weeks following the onset of symptoms but it had reported as early as one week following onset of symptoms. Exudative retinal detachment can develop in early stage of disease in conjunction with the active inflammation. Other complications like of retinal and optic neovascularization with vitreous hemorrhage, phthisis bulbi, ARN optic neuritis, Secondary glaucoma, Cataract and fellow eye involvement.
DIFFERENTIAL DIAGNOSIS
Progressive outer retinal necrosis syndrome (PORN), CMV retinitis, Ocular syphilis, Toxoplasmosis, Acute multifocal hemorrhagic retinal vasculitis, Large cell lymphoma, Behcets disease, Sarcoidosis, Endogenous or exogenous bacterial and fungal endophthalmitis and Commotion retinae (Berlins edema).
AIM OF THE STUDY
To compare the treatment outcomes and long term complications in ARN patients treated with only oral and combined antiviral therapy.
OBJECTIVES:
- Find rate of occurrence of retinal detachment in Acute retinal necrosis patients treated with oral and combined antiviral therapy.
- To study the treatment outcome in terms of visual acuity in Acute retinal necrosis patients treated with oral and combined antiviral therapy.
TYPE OF STUDY
Prospective, observation, hospital based case series study.
INCLUSION CRITERIA
All patients diagnosed to have acute retinal necrosis and had clinical features as described in standard diagnostic criteria by American Uveitis Society 1994[5] and given informed consent to take part in the study.
EXCLUSION CRITERIA
Patients diagnosed to have ARN, but not willing to take part in study.
METHODOLOGY
Source of data
All patients who attended Uvea clinic from a tertiary eye care hospital in India.
Period of study
The study period was from 1st December 2015 to 30th May 2017. Patient was recruited for a period of one year ( 1st December 2015 to 31st December 2016) and subsequently each case was followed up for 6 months duration.
METHOD
Patient recruitment started after institute review board (Ethical committee) approval of the study. Informed consent was obtained from all participants of the study. Patient was recruited into the study if they had clinical features as described in standard diagnostic criteria by American Uveitis Society 1994[5]. A detailed history was obtained from the patient regarding is ocular complains mainly his symptoms at presentation and history regarding any viral infection suffered by the patient and if present the type of viral infection was documented. Associated systemic illness was documented, in particular AIDS, as patients with AIDS are grouped as immunocompromised otherwise patients are grouped as immunocompetent.
Data sheet was prepared to record the demographic data of the patient like 1.Age, 2.Gender and 3.laterality of eye involved.
Patients after diagnosed to have Acute retinal necrosis clinically if needed investigated with USG B scan to rule out retinal detachment, ocular coherence tomography (OCT) to look for any macular involvement. Systemic investigation like Hemoglobin, total blood count, differential blood count, erythrocyte sedimentation rate, platelet count, urine analysis was done. ELISA for Human immunodeficiency virus was done to find patient’s immune status with patients consent if needed.
Serial Fundus photography was taken to document the improvement of the disease after treatment.
Treatment
Patients was given oral antiviral therapy as a sole antiviral or combined antiviral therapy as per treating physician discretion. In Oral antiviral therapy(Group1), T.Valacyclovir 1000mg tds/ day was given for 8 to 12 weeks. Combined antiviral therapy(Group2) include a combination of oral antiviral along with intravitreal antiviral are oral antiviral along with intravenous antiviral and intravitreal antiviral. Intravitreal antiviral given in the form of Gancyclovir 2000µg in 0.1ml and intravenous antiviral as Inj.Acyclovir 5-10mg/kg tds/ day for 5days. All patients are treated with cycloplegic and T.Prednisolone 1mg/kg per day in titrated dose as per the response.
Complications And Its Managments:
The most common complication occurring in Acute retinal necrosis was RETINAL DETACHMENT. The time gap of occurrence of retinal detachment from onset of acute retinal necrosis was documented.
Follow Up:
All patients followed up for 6 months. Visual acuity, intraocular pressure, and a complete ocular examination was carried out during all follow up visit Complication if any was documented and treated appropriately. At the end of six months final best corrected visual acuity was recorded.
DATA COLLECTION TECHNIQUE AND TOOLS
All data from primary source was collected by an individual interview, observation, and complete ophthalmic examination of the subjects as per the present proforma and any additional information like complication and its management was mentioned in detail. Later these primary data was entered in a Microsoft excel sheet for a complete database. Data was also collected from secondary sources like Pubmed, Medline and various other journals for comparison of the primary data. Visual acuity was measured using standard Snellens chart, converted to LogMar for statistical analysis.
Visual acuity which ranged from gain one line or more between initial and final vision was considered as improved visual acuity and visual acuity that dropped below 1 line or more between initial and final was considered detoriated visual acuity.
STATISTICAL METHODS
Mean (SD) and frequency (percentage) was used for continuous and categorical variable respectively. Fisher’s extract test or chi-square test was used to assess the difference between the categorical variable. Student t-test or Mann-Whitney U test was used to test mean difference between the two continuous variables. P-value of less than 0.05 considered as statistically significant. All statistical analysis was done by statistical software STATA 11.0
RESULTS
21 eyes of 18 patients studied, 11patients (61.11%) were males and 7patients (38.89%) were females. Bilateral involvement was seen in 3patients (14.28%). The mean age of presentation was 40.05±12.27 years (1SD). One patient (5.56%) out of 18 was immunocompromised, all other patient was immunocompetent.
Previous history of viral infection was given by 6 patients (33.33%). The most common viral infection being chicken pox seen 3 patients (50%).herpes zoster ophthalmicus in 1 patient (16.67%), viral keratitis in 1 patient (16.67%) and shingles in 1 patient (16.67%). Most common symptom found was defective vision (100%) reported in all 21 eyes studied followed by redness of eyes (87.1%), ocular pain (61.3%), photophobia (40%), floaters (35.5%), headache (3.5%). Keratic precipitates, cells & flare in anterior chamber, vitritis and retinal necrosis seen in all patients (100%), complicated cataract seen in 4 eyes (19.04%)
TREATMENT
15 eyes was given oral valacyclovir as sole antiviral (Group1), 6 eyes was given combined antiviral therapy (Group 2)
Group 1(oral therapy) = 71.43%
Group 2(combined therapy) = 28.57%
PROGRESSION TO RETINAL DETACHMENT
Graph 1
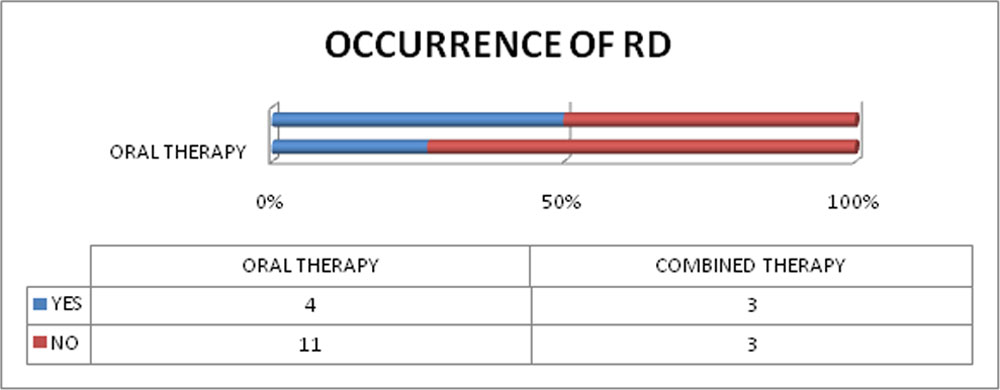
In oral therapy 4 eyes ( 26.67%) out of 15 eyes progressed to retinal detachment, 3 eyes out of 6 (50%) progressed to retinal detachment in combined therapy group.
Table 1:
|
Group |
Progression to RD |
Total |
P value@ |
|
| No
F (%) |
Yes
F (%) |
|||
| ARN Oral Therapy | 11 (73.33) | 4 (26.67) | 15 (100) |
0.354 |
| Combined Therapy | 3 (50) | 3 (50) | 6 (100) | |
| Total | 14 | 7 | 21 (100) | |
@Fisher’s exact test
The P value 0.354 (>0.05) says that, there is no association in the Progression to RD between the groups.
A total 7(33.33%) patients progressed to retinal detachment on the whole.
VISION ANALYSIS
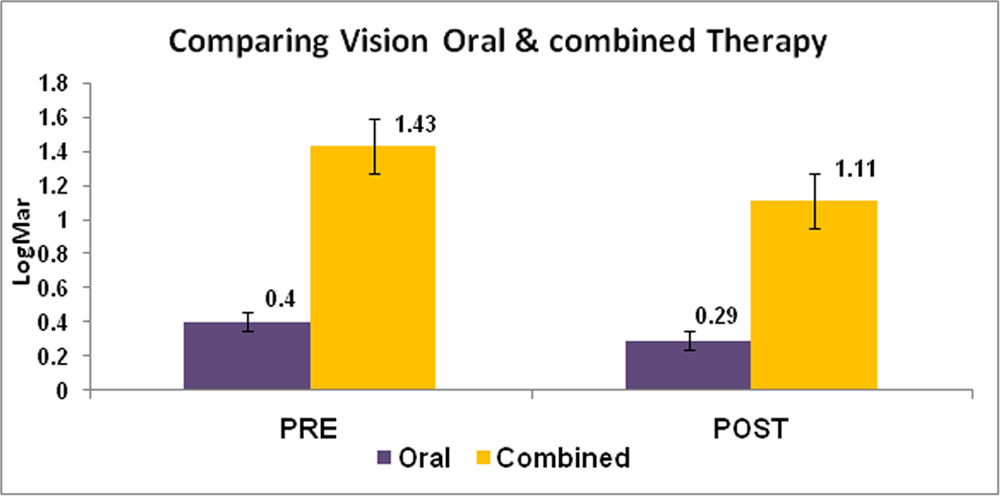
Graph 2:
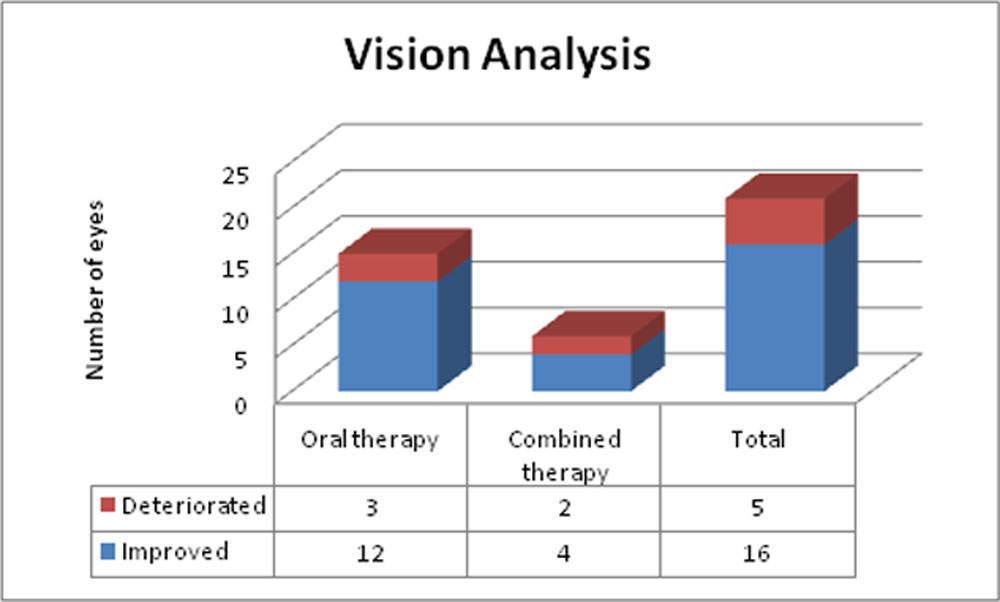
The final vision improved in 16 eyes (76.19%) out of 21eyes studied’
Table:2
|
Visual Acuity |
ARN Oral Therapy | Combined Therapy |
P value# |
||||
| N | Mean (SD) | Range | N | Mean (SD) | Range | ||
| Initial Vision | 15 | 0.4(6/15) 0.33 | 0(6/6) – 1(6/60) | 6 | 1.43(6/150)
1.14 |
0.6(6/24) – 2.9(PL) | 0.02 |
| Final Vision | 15 | 0.28(6/12) 0.27 | 0(6/6) – 0.78(6/36) | 6 | 1.1(6/75) 1.06 | 0.18(6/9) – 2.6(HM) | 0.04 |
| P value @ | 0.033 | 0.07 | |||||
# Mann Whitney U test; @ Wilcoxon Sign rank test
The P value 0.02 and 0.04 are less than 0.05 which says that there is a statistical significant difference between the initial vision and final vision of the two groups.
The P value 0.033 <0.05 says that there is a statistical significant difference between the initial vision and final vision of the ARN oral therapy group. The P value 0.07>0.05 says that there is no statistical significant difference between the initial vision and final vision of the combined therapy group.
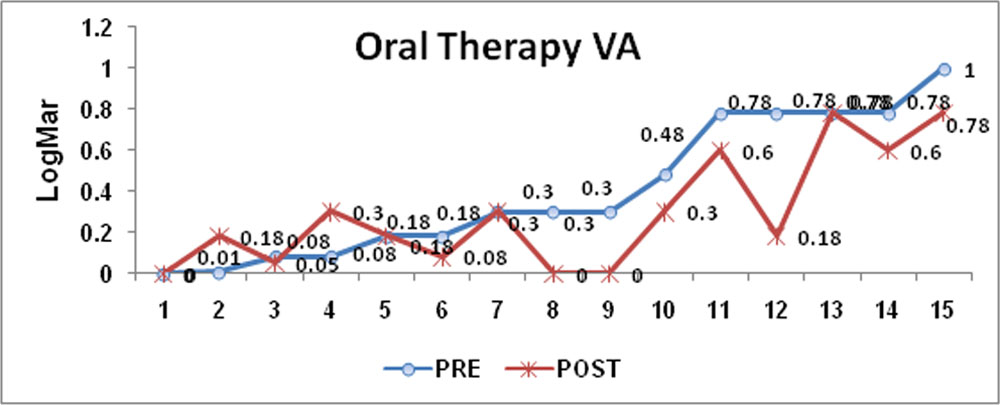
Graph 3:

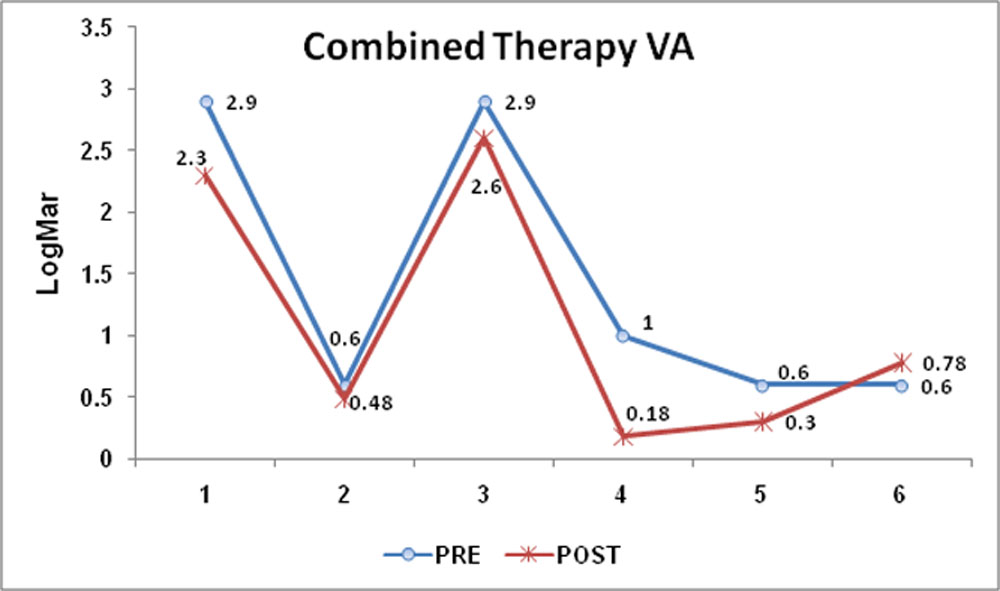
Graph 4:
Graph 5:
DISCUSSION
GENDER: Our study reveals that there exists no gender prelidiction between males and females in occurrence of acute retinal necrosis, but a slight male preponderance was observed as reported in various literature.
| STUDY | MALES | FEMALES |
| Muthiah et al [10] | 71% | 29% |
| Cochrane et al [11] | 55.6% | 44.4% |
| Flaxel et al [12] | 42% | 58% |
| Our study | 61.11% | 38.89% |
AGE: The mean age of occurrence of acute retinal necrosis in our study was 40.05±12.27(1SD)years, this is in accordance to Meghpara et al [13]they reported the mean age group to be 42 years.
IMMUNE STATUS: All patients with history of AIDS are considered immunocompromised. All immunocompromised patients reported in our study was males and one patient died during the follow up period. Our study reveals acute retinal necrosis is more common in immunocompetent patient than in immunocompromised patients. Previous studies also reported similar findings.
| STUDY | IMMUNOCOMPROMISED | IMMUNOCOMPETENT |
| Muthiah et al[10] | 23% | 77% |
| Cochrane et al[11] | 28% | 72% |
| Our study | 5.56% | 94.44% |
HISTORY OF VIRAL INFECTION: History of viral infection was found in 33.33% of patients in our study.
| STUDY | H/O VIRAL INFECTION |
| Cochrane et al[11] | 55.6% |
| Meghpara et al [13] | 45% |
| Flaxel et al[12] | 38% |
| Our study | 33.33% |
The most common viral infection reported was chickenpox (50%) followed by herpes zoster ophthalmicus, shingles and viral keratitis ( each 16.67%).No history of other herpes infection like HSV meningitis, genital ulcers was reported. Various other studies too reported chicken pox was the commonest viral infection preceded Acute retinal necrosis.
| STUDY | CHICKEN POX | HZO | SHINGLES | VIRAL KERATITIS |
| Cochrane et al [11] | 20% | 13.3% | – | 4.4% |
| Muthiah et al[10] | 70.6% | 20.7% | – | 9.7% |
| Flaxel et al[12] | 18% | 9% | 18% | |
| Our study | 50% | 16.67% | 16.67% | 16.67% |
TREATMENT: In our study, patients are treated with oral valacyclovir 1000mg per day ( given for approximately 8 to 12 weeks) or treated with intravenous acyclovir 10mg/kg 3times per day for 5days and followed with oral valacyclovir 1000mg 3 times per day. Few patients in addition to intravenous and oral acyclovir also given intravitreal Ganciclovir 2000µg in 0.1ml.Patients treated with oral valacyclovir as the sole antiviral administered are grouped as oral therapy patients and patients treated with 2 or more route of antiviral are grouped as combined therapy group. In our study 15eyes out of 21eyes (71.43%) treated with oral therapy and 28.57% of eye (6 eyes) treated with combined therapy. All patients in addition to antiviral received oral and topical prednisolone and cycloplegic. The treatment was administered as per the treating ophthalmologist discretion.
Emerson et al in the year 2006 reported about treating ARN with oral valacyclovir/ famicyclovir, as sole antiviral.
In our study no patients underwent prophylactic laser.
RETINAL DETACHMENT: The necrosis over time would progress to retinal detachment. The detachment may Exudative, reghmentogenous or combination of above mentioned two factors. Our study reports over all occurrence of retinal detachment to be 33.33% (7 out of 21 eyes suffered RD. In comparison to literature collected, occurrence of retinal detachment was lower in our study.
| STUDY | OCCURRENCE OF RD | TIME GAP OF OCCURENCE |
| Muthiah et al[10] | 75% | – |
| Cochrane et al[11] | 75% | 4-11 weeks |
| Hillenkamp et al [14] | 73% | 6-84 days |
| Flaxel et al[12] | 45% | 3wk-5 months |
| Roy et al [15] | 66.12% | |
| Our study | 33.33% | 1day- 14 wks |
OCCURRENCE OF RETINAL DETACHMENT BETWEEN PATIENTS TREATED WITH ORAL AND COMBINED ANTIVIRAL THERAPY:
On analysis of patients suffered retinal detachment, it was found that oral therapy patients progressed to retinal detachment lesser (26.67%) as compared to combined therapy patients (50%). It was also found a no statistically significance exists between both groups (P=0.354)
| STUDY | GROUP | OCCURRENCE OF RD |
| Emerson et al [16] | Oral therapy | 25% |
| Flaxel et al[12] | Combined therapy | 28.57% |
| Our study | Oral therapy | 26.67% |
| Our study | Combined therapy | 50% |
VISION ANALYSIS: Acute retinal necrosis is a potential blinding disease. Protection of vision is primary aim in treatment of the disease. Patients vision was monitored in all visits. Best corrected visual acuity is recorded by Snellens chart and converted to LogMar scale for statistical analysis. Patients vision is said to be deteriorated if his final vision is less than is vision at presentation and vision is said to be not deteriorated if patients final vision at the end of six months follow up remained the same or improved in comparison to his initial vision at presentation.
The overall visual acuity of all eyes studied had improved significantly at the end of six month of treatment. Our study found that 23 eye(79.39%) vision had not deteriorated and in 6 eyes (28.61%) vision had deteriorated.
| STUDY | VISION DETORIATED | VISION IMPROVED |
| Muthiah et al [10] | 44.1% | 26.5% |
| Emerson et al[16] | 25% | 75% |
| Our study | 23.81% | 76.19% |
Our study found the mean initial visual acuity in oral antiviral therapy group was 0.40LogMAR±0.33(1SD) and mean final visual acuity was 0.28±0.27LogMar. A statistically significant (P=0.033) improvement in visual acuity between initial and final vision in oral therapy. Cochrane et al [11] reported final mean visual acuity of patients treated with oral antiviral only was 0.89± 0.79 LogMar.
No statistical significant (P=0.0.07)improvement in visual acuity was noted between initial (mean= 1.43LogMar±1.14 (1SD)) and final visual acuity ( mean 1.10±1.03LogMar in combined antiviral therapy group. Flaxel et al [12] reported in combined antiviral therapy mean visual acuity improved from 1.01±0.61 LogMar to 0.59±0.51LogMar.
A statistically significant (P=0.02) exists between mean initial visual acuity between oral and combined therapy. Mean initial visual acuity was better in oral group than combined group.
LIMITATIONS IN OUR STUDY
- Acute retina necrosis is a rare disease, the study sample was small and follow up period was short. If the follow up period was extended more complications may be found.
- Sole oral antiviral therapy was started on patients with indolent acute retinal necrosis and combined therapy was started in more severe cases. This results in difference in both initial and final visual acuity.
CONCLUSION
Acute retinal necrosis is rare but potential blinding disease, polymerase chain reaction on ocular fluids helps to identify viral DNA and appropriate treatment can be instituted. Prompt diagnosis and good therapeutic approach is a must for better visual recovery. Vision threatening complication like retinal detachment can be prevented with judicious monitoring of ARN patients and prompt treatment. Oral antiviral and intravitreal antiviral are increasingly used in treatment of ARN. Primary treatment with oral antiviral for indolent ARN is an effective alternate to combined therapy as the later is invasive and requires hospitalization.
Clinical pictures
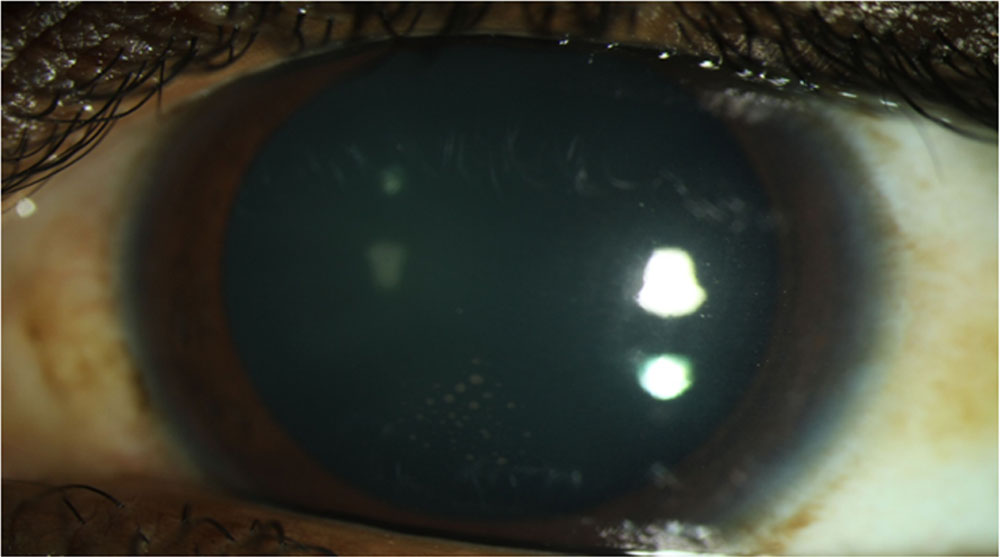
PICTURE 1: Arrow indicating fresh Granulomatous keratic precipitates in ARN patient
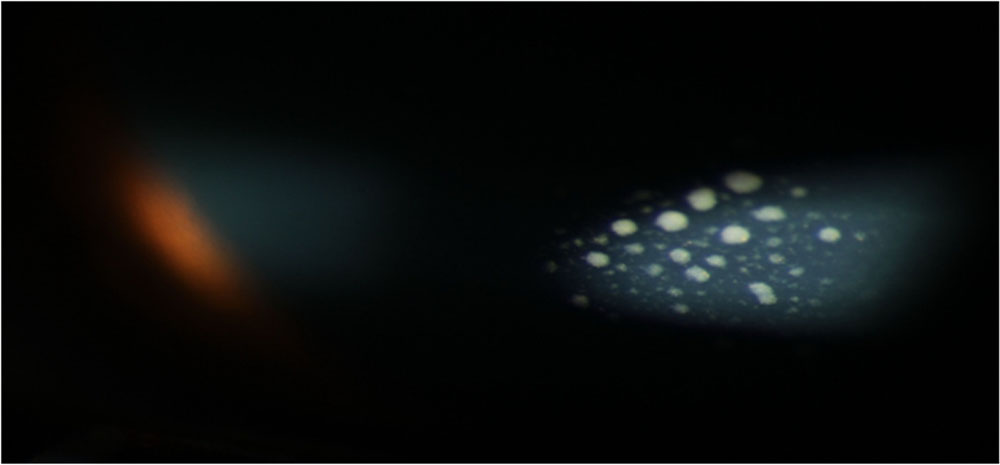
PICTURE 2: Magnified view of Granulomatous keratic precipitates with cells and flare in anterior chamber

PICTURE 3: Fundus photo of ARN patient showing vitritis. (i) slender arrows indicating occlusive vasculitis (ii) broad arrow white patch of retinal necrosis at periphery of retina.
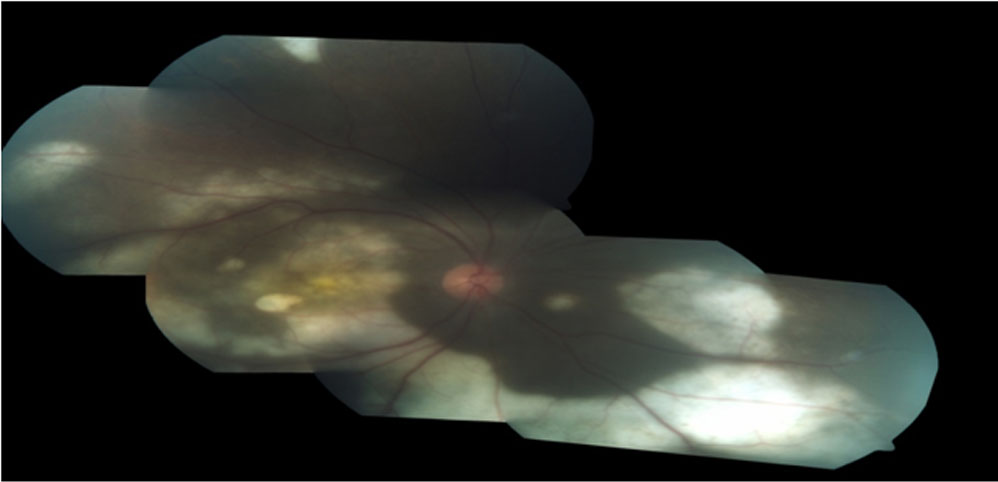
PICTURE 4: Fundus montage of ARN patient showing Retinal necrosis
KEY WORDS
- ARN: Acute retinal necrosis
- AIDS: Acquired immuno deficiency syndrome
- CMV: Cytomegalo virus
- FFA: Fundus fluorescein angiography
- HIV: Human immuno virus
- HSV: Herpes simplex virus
- LogMar: Logarithm of the minimum angle of resolution
- OCT: Optical coherence tomography
- PCR: Polymerase chain reaction
- USG-B scan: Ultra sonography B scan
- VZV: Varicella zoster
REFERENCES
- Urayama, A., Unilateral acute uveitis with periarteritis and detachment. Jpn J Clin ophthalmology, 1971. 25: p. 607-619.
- Willerson, D., Jr., T.M. Aaberg, and F.H. Reeser, Necrotizing vaso-occlusive retinitis. Am J Ophthalmol, 1977. 84(2): p. 209-19.
- Young, N.J. and A.C. Bird, Bilateral acute retinal necrosis. Br J Ophthalmol, 1978. 62(9): p. 581-90.
- Culbertson, W.W., et al., The acute retinal necrosis syndrome. Part 2: Histopathology and etiology. Ophthalmology, 1982. 89(12): p. 1317-25.
- Holland, G.N., Standard diagnostic criteria for the acute retinal necrosis syndrome. Executive Committee of the American Uveitis Society. Am J Ophthalmol, 1994. 117(5): p. 663-7.
- Ohtake-Matsumoto, A., et al., Spectral domain and swept source optical coherence tomography findings in acute retinal necrosis. Graefes Arch Clin Exp Ophthalmol, 2015. 253(11): p. 2049-51.
- Tam, P.M., C.Y. Hooper, and S. Lightman, Antiviral selection in the management of acute retinal necrosis. Clin Ophthalmol, 2010. 4: p. 11-20.
- Abe, T., et al., Interferon gamma expression and clinical features in patients with acute retinal necrosis syndrome. Graefes Arch Clin Exp Ophthalmol, 2003. 241(12): p. 982-7.
- Guo, L.B., et al., [Intravitreal injection of Ganciclovir in the treatment of acute retinal necrosis]. Zhonghua Yan Ke Za Zhi, 2007. 43(7): p. 631-7.
- Muthiah, M.N., et al., Acute retinal necrosis: a national population-based study to assess the incidence, methods of diagnosis, treatment strategies and outcomes in the UK. Br J Ophthalmol, 2007. 91(11): p. 1452-5.
- Cochrane, T.F., et al., Acute retinal necrosis in the United Kingdom: results of a prospective surveillance study. Eye (Lond), 2012. 26(3): p. 370-7; quiz 378.
- Flaxel, C.J., S. Yeh, and A.K. Lauer, Combination systemic and intravitreal antiviral therapy in the management of acute retinal necrosis syndrome (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc, 2013. 111: p. 133-44.
- Meghpara, B., et al., Long-term follow-up of acute retinal necrosis. Retina, 2010. 30(5): p. 795-800.
- Hillenkamp, J., [Diagnosis and therapy of acute retinal necrosis]. Ophthalmologe, 2009. 106(12): p. 1057.
- Roy, R., et al., Acute retinal necrosis: clinical features, management and outcomes–a 10 year consecutive case series. Ocul Immunol Inflamm, 2014. 22(3): p. 170-4.
- Emerson, G.G., et al., Primary treatment of acute retinal necrosis with oral antiviral therapy. Ophthalmology, 2006. 113(12): p. 2259-61.
Leave a Comment