
Dr. Meenakshi CT, T18801, Dr. Harsha Rao, Dr. Zia Sultan Pradhan, Dr. Sathi Devi A V
Abstract
Purpose
To evaluate the causes, risk factors and treatment of ocular hypertension (OHT) following posterior chamber phakic implantable collamer lens (ICL) surgery.
Methods
Retrospective analysis of 470 eyes (287 patients) with refractive myopia which underwent ICL implantation of the following types between 2011 and 2016-
- Visian ICL V4B without Aquaport by STAAR Surgical, USA (PI done intra-operatively.)
- Visian ICL V4C with central Aquaport by STAAR Surgical, USA.
- Implantable Phakic Contact Lens(EyePCL) with peripheral Aquaport by Care Group, India
Comparison was done between eyes which did not develop OHT and eyes which developed OHT following ICL implantation. Statistical analysis was performed (STATA) with Student’s t-test for continuous data and Pearson’s chi-squared test for categorical data.
Results
Seventy-nine of 470 eyes (16%) developed OHT of which 30 of 256 eyes (11.7%) were with V4B ICL, 41 of 194 eyes (21.1%) with V4C ICL and 8 of 20 eyes (40%) with EyePCL.Eyes with greater myopia (P=0.0005) and thicker corneas (P=0.0002) were more likely to develop OHT.The etiology was retained viscoelastic in 29 eyes (36.7%), steroid response in 44 eyes (55.7%), both mechanisms in 4 eyes (5.1%) and pupillary block in 2 eyes(2.5%). The median time for normalization of IOP was 7 days (IQR 2,60)in eyes with retained viscoelastic and 60 days(IQR 21,270) in eyes with steroid response. The mean number of IOP lowering medications used was 1.9(IQR 1,4). Long term IOP lowering therapy (>3 months) was required in 13 eyes (16.4%) with 5 eyes continuing treatment at the last followup. Two eyes which developed pupillary block were effectively managed with laser iridotomy. One eye with Urrets-Zavalia syndrome underwent anterior chamber wash for retained viscoelastic.
Conclusion
Secondary OHT was seen in 16% of eyes following ICL surgery. Eyes with higher myopia, thicker corneas and eyes with EyePCL implantation had higher incidence of OHT. Following ICL surgery, early detection of Ocular hypertension and its causes are important for appropriate management.
Key words
Implantable collamer lens (ICL), Ocular hypertension (OHT), Intra-ocular pressure (IOP), Peripheral Iridotomy (PI).
Introduction
Posterior Chamber Phakic Implantable Collamer lens implantation (ICL) has become one of the most commonly performed refractive surgeries for high myopia1 .It is considered a relatively safe procedure and effective especially in patients when conventional refractive procedures are not feasible due to thinner corneas, formefruste keratoconus, very high myopia and astigmatism.
Increase in intraocular pressure has been a noted complication observed following ICL implantation4, 8.We also know that myopia has been associated with steroid response and is also a risk factor to develop glaucoma2. Therefore, the purpose of our study was to identify the incidence of secondary Ocular hypertension (OHT) following ICL implantation, its causes, risk factors and management.
Implantable Collamer lens of the following types were used in our study.
1.V4B Visian ICL which is a posterior chamber Implantable Collamer Lens (ICL; Staar Surgical Co.,Monrovia,CA,USA) which is FDA approved for surgical correction of myopia. It is a single piece collamer lens with plate haptic design and anterior lens vaulting. Hence a peripheral iridotomy either pre-operative or intra-operative is indicated to prevent pupillary block.
2.V4c Visian ICL(CentraFLOW technology) which has a 0.36mm central aperture (KS-AquaPORT) in the optic to facilitate the aqueous flow. Hence a PI is not indicated.
3.EyePCL (Implantable Phakic Contact lens; Care group,India)is made of hybrid hydrophilic material. It has holes in the marginal peripheral area to assist aqueous flow.
Materials and methods
Retrospective analyses of the medical records of 287 patients (470 eyes) who underwent poster chamber phakic implantable collamer lens implantation between January 2011 and June 2016 was done. The written informed consent was taken from all the patients for analysis of medical records.
All patients underwent routinerefraction, slit lamp examination and dilated fundus examination along with slit lamp photo, Optical Biometry (LENSTAR LS 900,Haag-Streit,USA), topography (Pentacam; OCULUS, Inc, Arlington, WA), (OrbscanIIz; Bausch and Lomb), Specular microscopy(TOMEY EM 3000,Japan), Anterior segment Optical coherence tomography (ASOCT;VisanteOCT;Carl Zeiss Meditec, CA,USA), Ultrasound biomicrosopy (UBM; OTI ; Ophthalmic Technlogies, Toronto, Canada).
The ICL power calculation was performed according to the manufacturer’s instructions and all eyes were targeted for emmetropia. The size of the ICL was calculated based on the white to white corneal diameter, sulcus to sulcus measurement and anterior chamber depth.
All ICL surgeries were done by skilled cataract and refractive surgeons. All patients with V4B ICL implantation underwent surgical peripheral iridectomy (PI) during surgery. The surgical and post-operative topical medications protocol was the same among all surgeons. A temporal clear corneal section was made followed by 2 side port entries with MVR blade.The anterior chamber was filled with viscoelastic (Appavisc; 2% w/v injection hydroxypropylmethylcellulose).ICL was injected into the anterior chamber by Micro-STAAR injector (STAAR Surgical Co.,Monrovia,CA) through the clear corneal section and the footplates were tucked in behind the iris. In case of ToricICL,the ICL was aligned along the required axis. Viscoelastic was washed from the anterior chamber by co-axial irrigation aspiration.The corneal section and side ports were hydrated.
Post-operatively, patients were prescribed topical moxifloxacin 0.5% ophthalmic solution (Vigamox; Alcon Laboratories,Inc.FortWorth TX, USA) four times daily for 2 weeks and topical prednisolone acetate 1% (Pred Forte; Allergan,Inc., Irvine, CA) four times daily, on a tapering schedule over a month.
The scheduled post-operative visits were first day, first week and 6 weeks after surgery. Slit lamp photo and ASOCT were repeated at every followup visit.
Intra-ocular pressure (IOP) measured >21 mmHg at any time following surgery with healthy disc was considered as ocular hypertension and IOP >21mmHg with glaucomatous optic nerve head changes was considered as Glaucoma. Intraocular pressure was measured by Goldmann Applanation tonometer and four mirror indentation gonioscopy was done to assess the angle status.
Statistical Analysis
Statistical analysis was performed (STATA 13.1,StataCorp LP, Texas, USA) with Student’s t-test for continuous data and Pearson’s chi-squared test for categorical data. Comparison was done between the groups which developed OHT with the group which did not develop OHT.
Results
Four hundred and seventy eyes which underwent ICL implantation were reviewed, of which 79 eyes (16%) developed ocular hypertension.
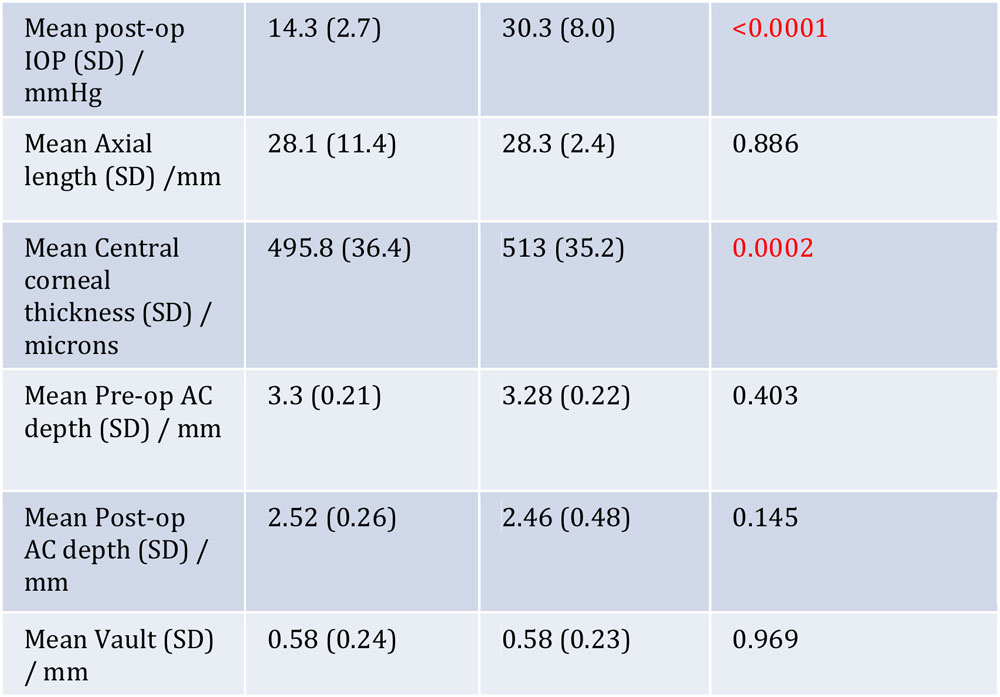
The comparison of demographic data between eyes which developed OHT and the group which did not develop OHT is listed in Table 1.
Table 1- Comparison of Demographic and clinical characteristics between the two groups
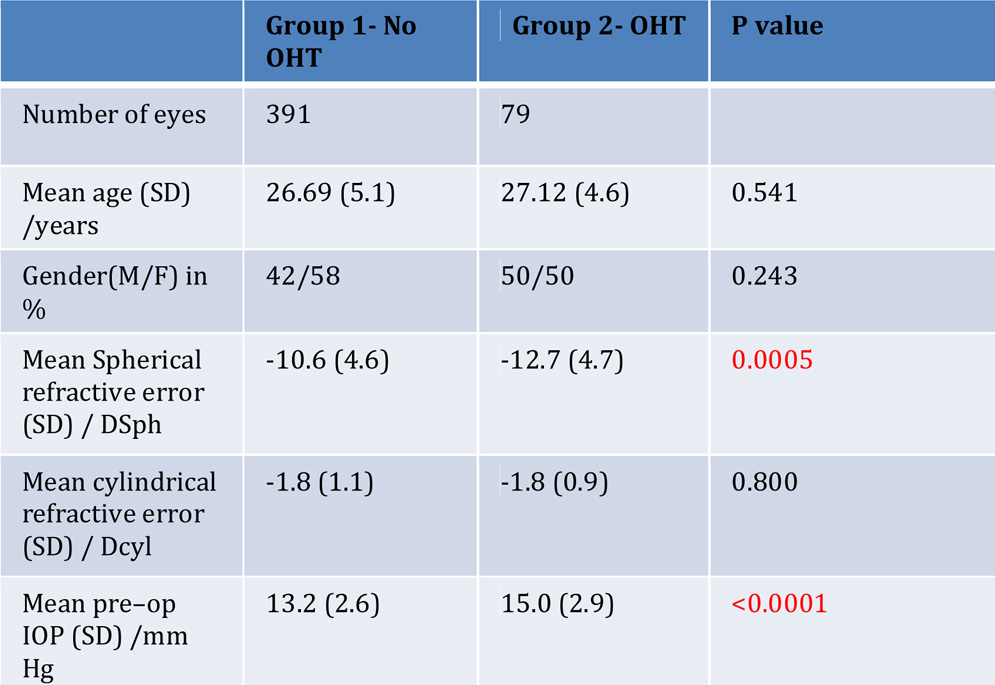
The difference in the mean age (p=0.54) and gender (p=0.24) among patients who did not develop OHT and eyes which developed OHT were not statistically significant.
The mean pre-operative spherical refractive error was -10.69 Dsphere in eyes which did not develop OHT and -12.72 Dsphere among eyes which developed OHT and the difference was statistically significant (p =0.0002). However there was no significant difference when the cylindrical power was compared between the two groups (p=0.80). The axial length was also found to be comparable between the two groups (p=0.88). There was statistically significant difference (p=0.0002) between the central corneal thickness of the group which did not develop OHT (495 microns) and the group which developed OHT (513 microns). There was no statistically significant difference in the pre-operative anterior chamber depth (ACD), post-operative vault and post operative anterior chamber depth between the two groups. There was statistically significant difference (p=0.004) in the incidence of OHT in eyes which did not have either a PI or aquaport.
There was no significant difference in the incidence of OHT among the different years of study or among the different surgeons.
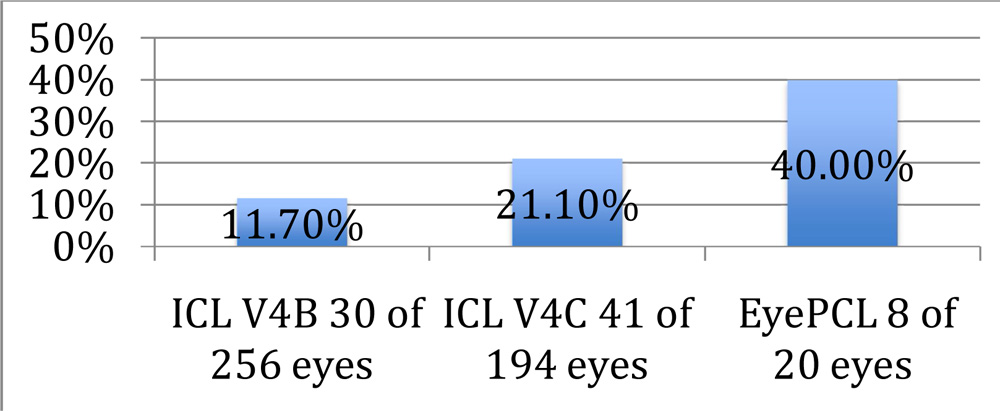
Of the 470 eyes reviewed, 256 eyes were with V4B ICL, 194 eyes were with V4C ICL and 20 eyes were with EyePCL. Seventy nine eyes developed OHT of which 30 eyes (11.7%) were with V4B ICL, 41 eyes (21.1%) with V4C ICL and 8 eyes (40%) with EyePCL. This difference on incidence of OHT between the three types of ICL was statistically significant (p<0.001).(Table 2)
Table 2- Incidence of OHT in different types of ICL
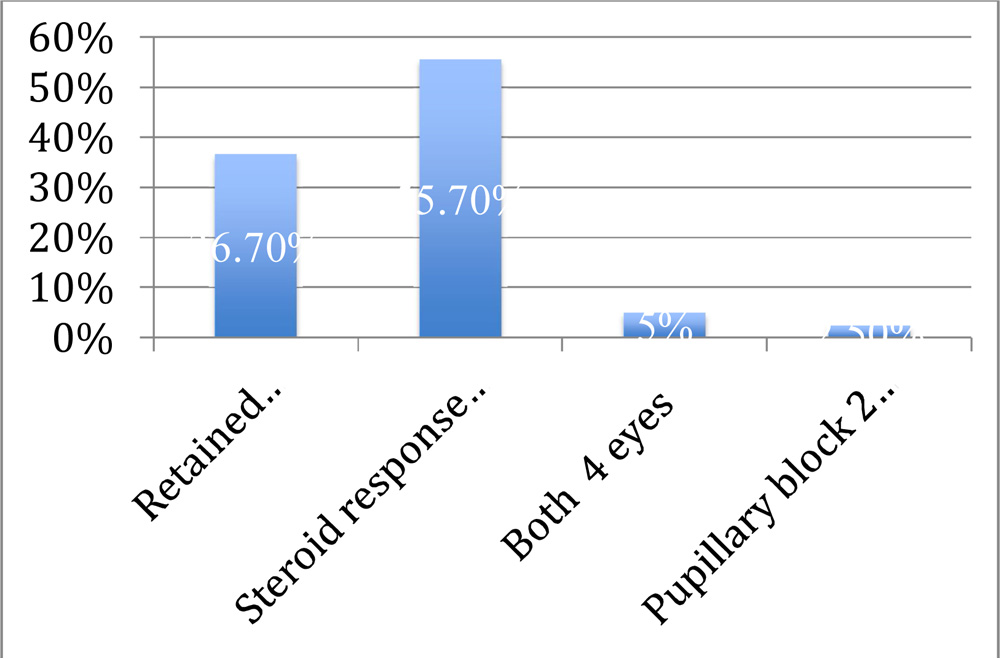
Steroid response was the most common cause of OHT (44 of 79 eyes -55.7%) followed by retained viscoelastic (29 of 79 eyes-36.7%), both mechanisms (steroid response and retained viscoelastic) in 4 eyes (5.1%) and pupillary block in 2 eyes (2.5%).(Table 3 )
Table 3- Etiology of OHT
The median time of onset of raised IOP was 16 days (IQR 7,180) in eyes with steroid response and the median time for normalization of IOP was 60 days (IQR 21,270). The median time of onset of raised IOP due to retained viscoelastic was 1 day and the median time for normalization of IOP was 7 days (IQR 2,60).
All patients were started on topical AGM with or without oral hypotensive agents depending on the magnitude of raised IOP. One eye with V4B ICL with lamellar PI and one eye with IPCL but without PI developed pupillary block on first post-operative day. They were effectively managed with YAG laser peripheraliridotomy (PI)and ocular hypotensive agents. The median number of IOP lowering medications used was 1.9 (IQR 1,4). Long term IOP lowering therapy (> 3 months) was required in 13 eyes (16.4%) with 5 eyes continuing treatment at the last followup. One eye developed Urrets Zavalia syndrome which underwent anterior chamber wash for retained viscoelastic.
Her IOP was successfully controlled with topical anti-glaucoma medications.
None of the eyes which developed OHT progressed to glaucoma.
Discussion
Refractive surgery has been widely performed for high myopia and ICL implantation has emerged as an effective option when conventional refractive procedures are not feasible. Even though the safety of ICL has been studied, it does have some complications, one of which is raised intra-ocular pressure1. Myopia is a well known risk factor for glaucoma2. As ICL implantation is most commonly performed on eyes with high myopia, they are at higher risk of developing raised intra-ocular pressure following surgery.
The incidence of secondary OHT has been noted as 16% (79 of 470 eyes) in our study. Steroid response was the most common cause of OHT.Many clinical studies have showed the higher incidence of steroid response in myopic eyes3.The raised IOP was managed conservatively with the ocular hypotensive agents and quick tapering of topical steroids.
Retained viscoelastic6 was the second common cause of OHT. The presentation was usually on the first post-operative day with or without microcystic edema of the cornea. The transient rise in IOP was managed with oral and topical anti-glaucoma medications. The median time for normalization IOP was 14 days (IQR 2,60). Thorough wash of viscoelastic by coaxial irrigation aspiration has been advocated to prevent this complication.
Both mechanisms i.e retained viscoelastic and steroid response were observed in 4 eyes.
Two eyes presented with pupillary block5on first post-operative day with pain,redness and closed angles on gonioscopy. One eye had a V4b implantation with lamellar PI and the other eye was with EyePCL without a PI. Both the eyes were effectively managed with YAG PI(Figure1and 2) and topical ocular hypotensive agents.
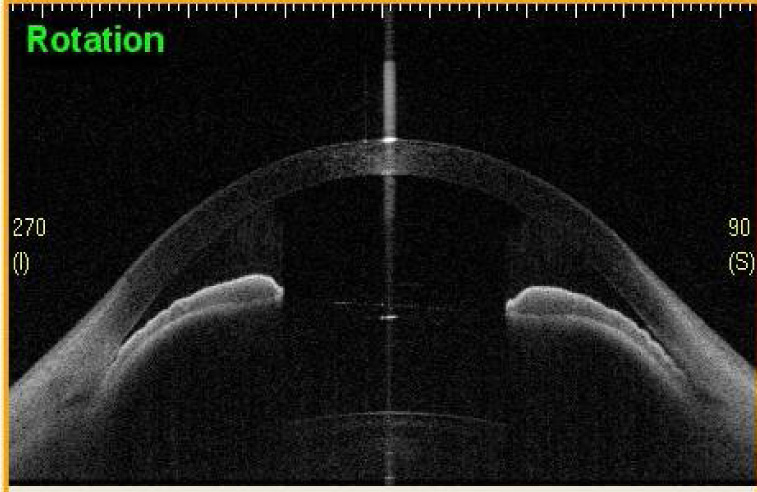
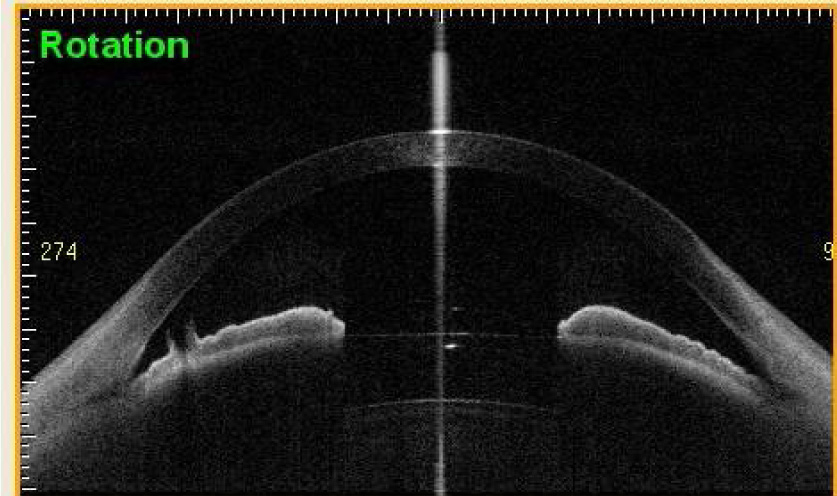
Figure 2- ASOCT image of pupillary block relieved following PI in EyePCL
Two eyes which underwent EyePCL with high vault and shallow AC and appositional closure of angles on gonioscopy also underwent prophylactic YAG peripheral iridotomy, despite normal IOP.
One eye with V4B ICL developed Urrets Zavalia syndrome. She had acute elevation of IOP on post-operative day 1 with a patent surgical PI and oval dilated pupil with iris tuck nasally. She was started on oral and topical anti-glaucoma medications. She underwent anterior chamber wash for removal of any retained viscoelastic. She also developed anterior uveitis and was treated with topical steroids. Gonioscopy revealed angles open in all quadrants except in the nasal quadrantwhich opened upto anterior trabecular meshwork with increased pigmentation in the inferior quadrant. UBM showed asymmetric placement of haptic and the iris tuck nasally(Figure 3).Iris tuck was released surgically.Iris fluorescein angiogram showed patchy and delayed filling of iris vessels pathognomonic of Urrets Zavalia syndrome(Figure 4). She developed severe anterior uveitis and was treated with topical steroids. Her IOP normalized at one month following surgery. At 3 months post surgery, her IOP was normal off AGM but the pupil remained dilated with sphincter atrophy(Figure 5 and 6).
Urrets Zavalia syndrome7 is an uncommon post-operative complication where there is acute post-operative raised IOP leading to pupillary sphincter ischemia and a fixed dilated pupil. It can occur secondary to retained viscoelastic or pupillary block with recurrent post-operative uveitis. Treatment is with topical steroids and ocular hypotensive agents. Other treatment options described in literature are a regime of sympatholytic drop (guanethidine) q4h for a day followed by Pilocarpine 2% for several days, soft colored contact lens, phakic IOL explantation with clear lens extraction and IOL implantation with either capsule tension rings (CTR) with opaque iris segments or intracapsular Hermeking iris prosthetic implants.
None of these that developed secondary OHT required ICL explantation due to secondary OHT. None of the eyes developed glaucomatous disc changes.
The limitations of our study include the retrospective nature of the study and the comparatively fewer eyes in the EyePCL group. (asEyePCL was introduced much later than the other lenses).
Conclusion
Secondary OHT is a common complication following phakic ICL implantation with 16% incidence in our study. Eyes with higher myopia and thicker CCT had higher incidence of OHT. Though eyes which underwent EyePCL implantation had significantly higher incidence of OHT, it cannot be considered a risk factor due to lesser number of patients in this group and shorter follow-up period. All the eyes with EyePCL implantation, despite having peripheral holes9 have a tendency to develop pupillary block as the holes are covered by the iris. Hence a peripheral iridotomy either prior to or during surgery is recommended.Monitoring the IOP at every post-operative visit is important. Early detection and understanding the mechanism causing ocular hypertension helps us decide the appropriate management. Early and effective management of ocular hypertension helps prevent progression to glaucoma.
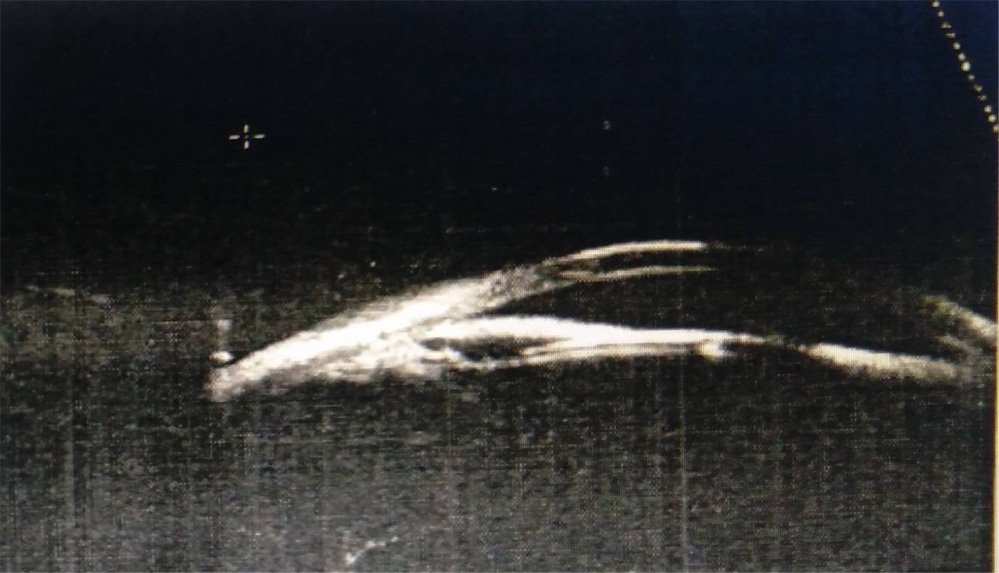
Figure 3- UBM showing asymmetric placement of haptic in the sulcus in the eye which developed Urrets Zavalia syndrome
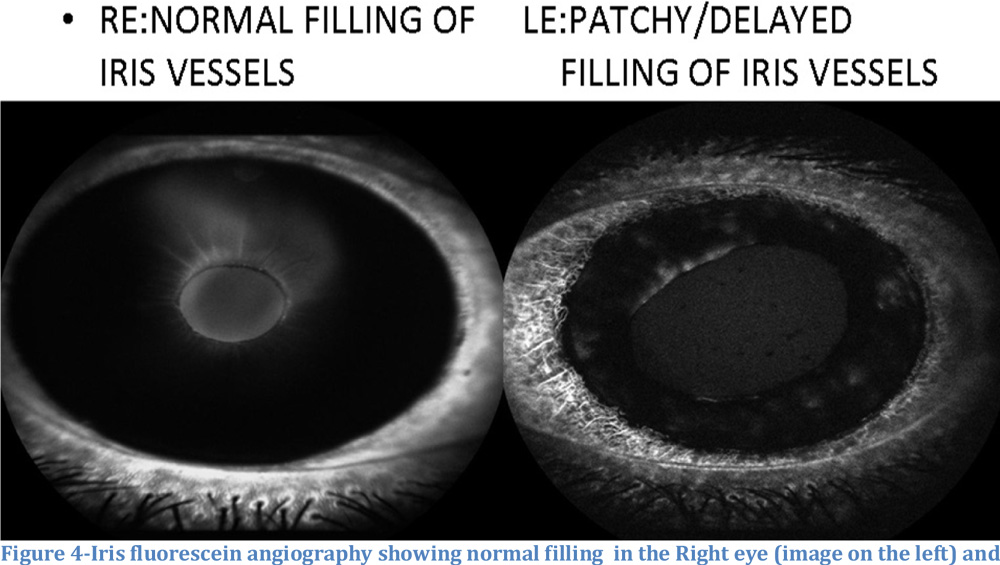

Figure 5 showing pigments on the ICL surface in the eye which developed Urrets Zavalia syndrome.
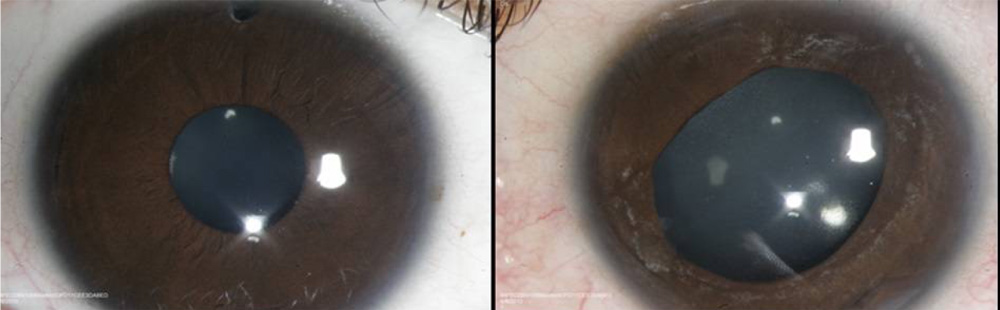
Figure 6 showing Right eye following ICL V4b implantation with surgical PI and Left eye with Urrets Zavalia syndrome following ICL implantation showing fixed dilated pupil with sphincter atrophyafter 3 months
References
- Fernandes P, Gonzalez-Meijome JM, Madrid-Costa D, Ferrer-Blasco T, Jorge J, Montes-Mico R. Implantable collamer posterior chamber intraocular lenses: a review of potential complications. Journal of refractive surgery. 2011;27(10):765–76. doi: 10.3928/1081597X-20110617-01. pmid:21710954
- Marcus MW, de Vries MM, Junoy Montolio FG, Jansonius NM. Myopia as a risk factor for open-angle glaucoma: a systematic review and meta-analysis. Ophthalmology 2011;118(10):1989–94 e2. doi: 10.1016/j.ophtha.2011.03.012. pmid:21684603
- Chang DF, Tan JJ, Tripodis Y. Risk factors for steroid response among cataract patients. Journal of Cataract & Refractive Surgery. 2011 Apr 30;37(4):675-81.
- Sanchez-Galeana CA, Zadok D, Montes M, Cortes MA, Chayet AS. Refractory intraocular pressure increase after phakic posterior chamber intraocular lens implantation. Am J Ophthalmol. 2002;134(1):121–3. pmid:12095821
- Smallman DS, Probst L, Rafuse PE. Pupillary block glaucoma secondary to posterior chamber phakic intraocular lens implantation for high myopia. Journal of cataract and refractive surgery. 2004;30(4):905–7. doi: 10.1016/j.jcrs.2003.09.019. pmid:15093659
- Almalki S, Abubaker A, Alsabaani NA, Edward DP. Causes of elevated intraocular pressure following implantation of phakic intraocular lenses for myopia. Int Ophthalmol 2016;36(2):259–65. doi: 10.1007/s10792-015-0112-4. pmid:26265323
- Al Habash A, Al Arfaj K, Al Abdulsalam O. Urrets-Zavalia syndrome after implantable collamer lens placement. Digital journal of ophthalmology :dJO. 2015;21(3):1-11. doi:10.5693/djo.02.2014.09.002
- Gonzalez-Lopez F, Bilbao-Calabuig R, Mompean B, et al. Intraocular pressure during the early postoperative period after 100 consecutive implantations of posterior chamber phakic intraocular lenses with a central hole. Journal of cataract and refractive surgery. 2013;39(12):1859-1863.
- Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clinical ophthalmology (Auckland, NZ). 2016;10:1059.
Leave a Comment