
Dr. Jayasri Kanthalu Narayanamoorthy, J20067, Dr. Mahesh Kumar, Dr. Kowsalya Akkayasamy
Aim: To assess the Demographics, various Etiologies of Isolated Sixth Nerve palsy and role of Neuroimaging in Diagnosis and Management in a Tertiary Eye Care Centre in South India. Design: Hospital based Retrospective case analysis of 185 Neurologically Isolated sixth nerve palsy from Jan 2016 to Dec 2016. Results: Total cases were 185.Mean age of presentation was 51 years with Male preponderance. Of the 185 cases, 135 were Ischemic (73%) group (with vasculopathic risk factors) and 50 were Non Ischemic (27%) group (without vasculopathic risk factors). Among Non-Ischemic, Trauma(7.02%), Inflammatory (6.48%), False localising sign(5.4%), Tumour (3.2%), Idiopathic(2.1%), Infective(1.08%), congenital(1.08%) and Restrictive(0.5%).Neuroimaging yielded significant diagnosis in 84% of Non Ischemic cases. Conclusion: In our study Micro vascular ischemia was the commonest cause. In the absence of risk factors, a suggestive history, or positive laboratory and clinical findings Neuroimaging can serve as a useful diagnostic tool in identifying the exact cause of sixth nerve palsy.
INTRODUCTION
The sixth cranial nerve also known as the Abducent nerve (CN VI) is a purely motor nerve, which moves the eye into abduction. Isolated sixth nerve palsy is a common neuro-ophthalmic problem often presenting to the general ophthalmologist [1, 2], with the annual incidence of approximately 11.3/1, 00,000 in a geographically defined population [2].Etiologies like Microvascular ischemia (diabetes, hypertension), trauma, tumour, Inflammatory &idiopathic are the causes of sixth nerve palsy. In majority of cases, Microvascular ischemia is the commonest cause of sixth nerve palsy, which spontaneously improves over time (usually within 3 to 6 months) [2,3,4] . Alternative etiologies of CN VI palsy with grave neurological implications often cannot be excluded without neuroimaging. However, the practice of obtaining neuroimaging for every patient presenting with an acute, isolated CN VI palsy is a costly diagnostic paradigm [1]. This study highlights the various etiologies of sixth nerve palsy and the role of neuroimaging in diagnosis and management. Furthermore we recommend an algorithm for clinical evaluation and need of neuroimaging in isolated sixth nerve palsy.
MATERIALS AND METHODS
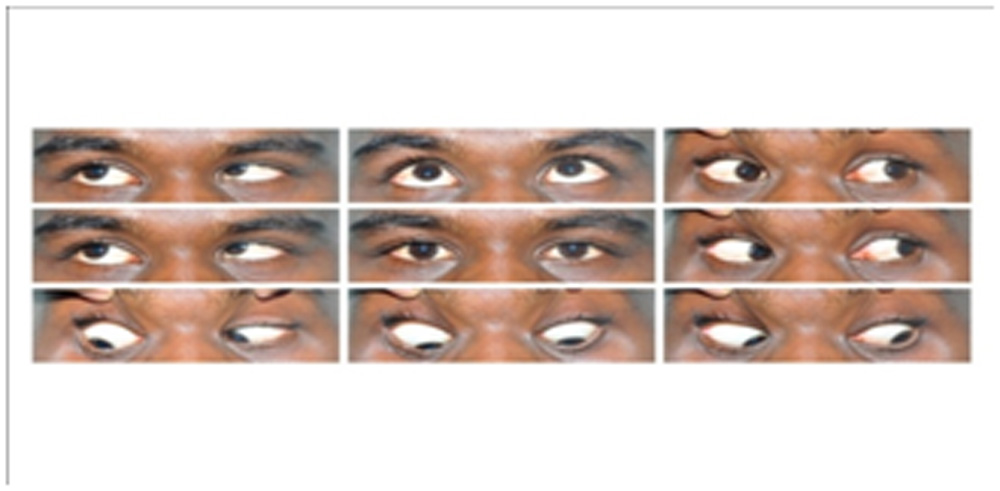
It is a Hospital based Retrospective case analysis of 185 Neurologically Isolated sixth nerve palsy presented to neuro ophthalmology department from Jan 2016 to Dec 2016.Documentation included age, gender, presenting complaints, history of diabetes, hypertension, trauma and mode of onset. All patients with congenital or acquired isolated sixth nerve palsy were included in our study and multiple cranial nerve palsy was excluded. For all patients, slit lamp examination, systemic and neurological examinations was done (Fig1). All patients with sixth nerve palsy were diagnosed clinically and documented with Hess and diplopia charting (Fig 2). Neuroimaging (MRI/MRA Brain) was ordered wherever indicated. The data collected was analysed and interpreted.
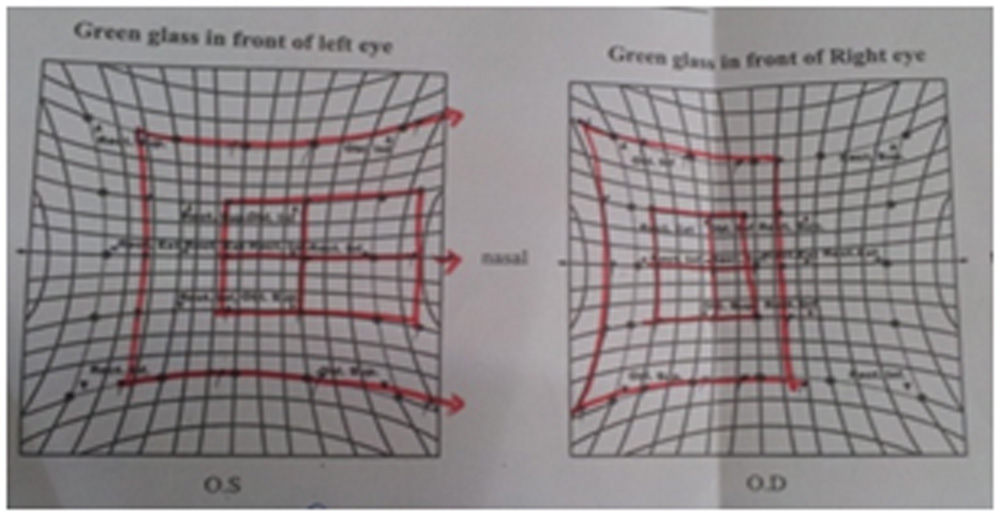
Fig.1 limitation abduction in RE sixth nerve palsy
RESULTS
A total of 185 patients was enrolled in this study. Of these 132 were males and 53 were females. Mean age of presentation was 51 years with Male preponderance. Of the 185 cases, 135 were Ischemic (73%) and 50 were Non Ischemic group (27%) [Fig 3].In our study, Microvascular ischemia was the commonest cause of sixth nerve palsy. Among 135 ischemic cases, Diabetes alone accounted for 63(34.05%), coexistent diabetes& hypertension 40(21.6%), hypertension alone 21(11.35%), hyperlipidaemia 6(3.2%), coronary artery disease 5(2.7%) [Fig 4]. Neuroimaging was done in 25 cases out of 135 cases, which showed positive findings only in 2 cases (8%). One patient aged 45 years who was a known case of chronic myeloid leukaemia on treatment with vasculopathic risk factors presented to us with isolated sixth nerve palsy .He underwent neuroimaging which showed Leukemic deposits/soft tissue lesion in anterior cavernous sinus and was referred to the Oncologist. . Another patient aged 43 years with coronary artery disease underwent neuroimaging which showed pre pontine haemorrhage and the patient was referred to the Neurologist.
Fig 3-Etiology of isolated sixth nerve palsy in our study
Fig 4-Distribution of risk factors in ischemic nerve palsy
In Non ischemic group, trauma accounted for 13(7.02%) ,Inflammatory 12(6.48%) ,false localising sign 10(5.4%),tumour 6 cases(3.2%) without vasculopathic risk factors, idiopathic(unknown etiology) 4 cases(2.16%),infective 2(1.08%),congenital 2(1.08%)and restrictive 1(0.5%) [Fig 5].Neuroimaging was done for all non-ischemic cases.42 cases (84%) out of 50 cases showed positive MRI findings which was diagnostically significant.
Etiology of isolated sixth nerve palsy in our study
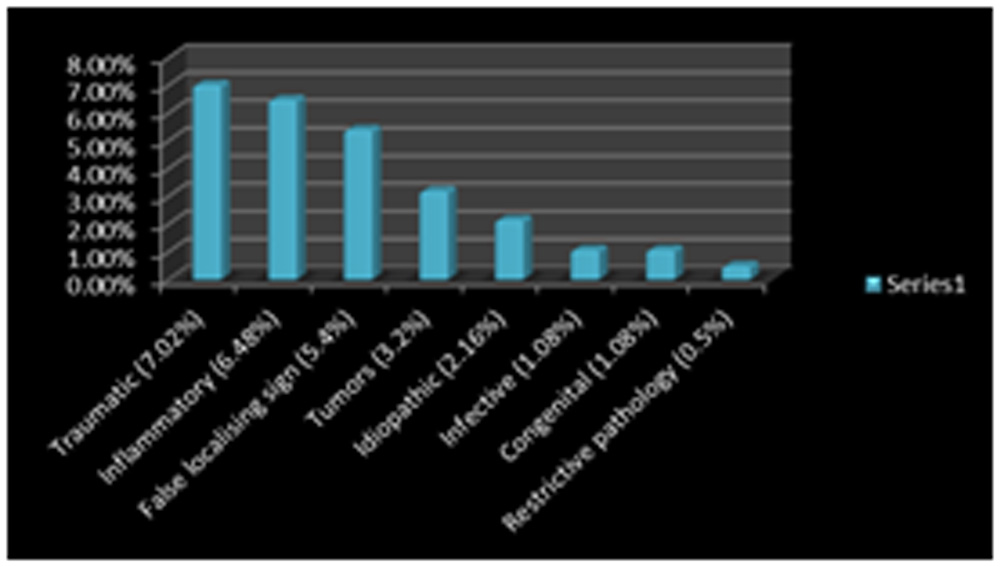
Fig 5-Etiology of non ischemic sixth nerve palsy in our study
DISCUSSION
Microvascular ischemic CN VI palsy is a presumptive diagnosis based on [5]
(1) Presence of vasculopathic risk factors
(2) Clinical presentation
(3) Clinical course.
Microvascular ischemic ophthalmoplegia classically presents with an abrupt onset, transitory pain, absence of other neurological findings, and spontaneous resolution over several months [6]. Diabetes mellitus and arterial hypertension are widely held to be the most common risk factors for microvascular ischemic CN VI palsy [3, 5, 6]. Studies have also suggested other risk factors including hyperlipidaemia, coronary artery disease, or alternative signs of hypertensive end-organ damage such as left ventricular hypertrophy (LVH) [2,7,8]. Patel et al. [2] reviewed 137 cases of CN VI palsy in patients of all ages, and found the most frequent associations to be unknown (26%), hypertension alone (19%), diabetes mellitus and hypertension (12%), and diabetes mellitus alone (4%).In contrast, our study revealed a different picture, Diabetes alone accounted for (34.05%), ,coexistent diabetes and hypertension-(21.6%), hypertension alone (11.35%), , hyperlipidaemia-(3.2%), coronary artery disease- (2.7%), traumatic (7.02%),inflammatory(6.48%)[Fig-6] ,false localising sign(5.4%),tumour(3.2%)[Fig-7],idiopathic(unknown etiology)-(2.16%),infective-(1.08%), congenital-(1.08%)and restrictive-(0.5%).
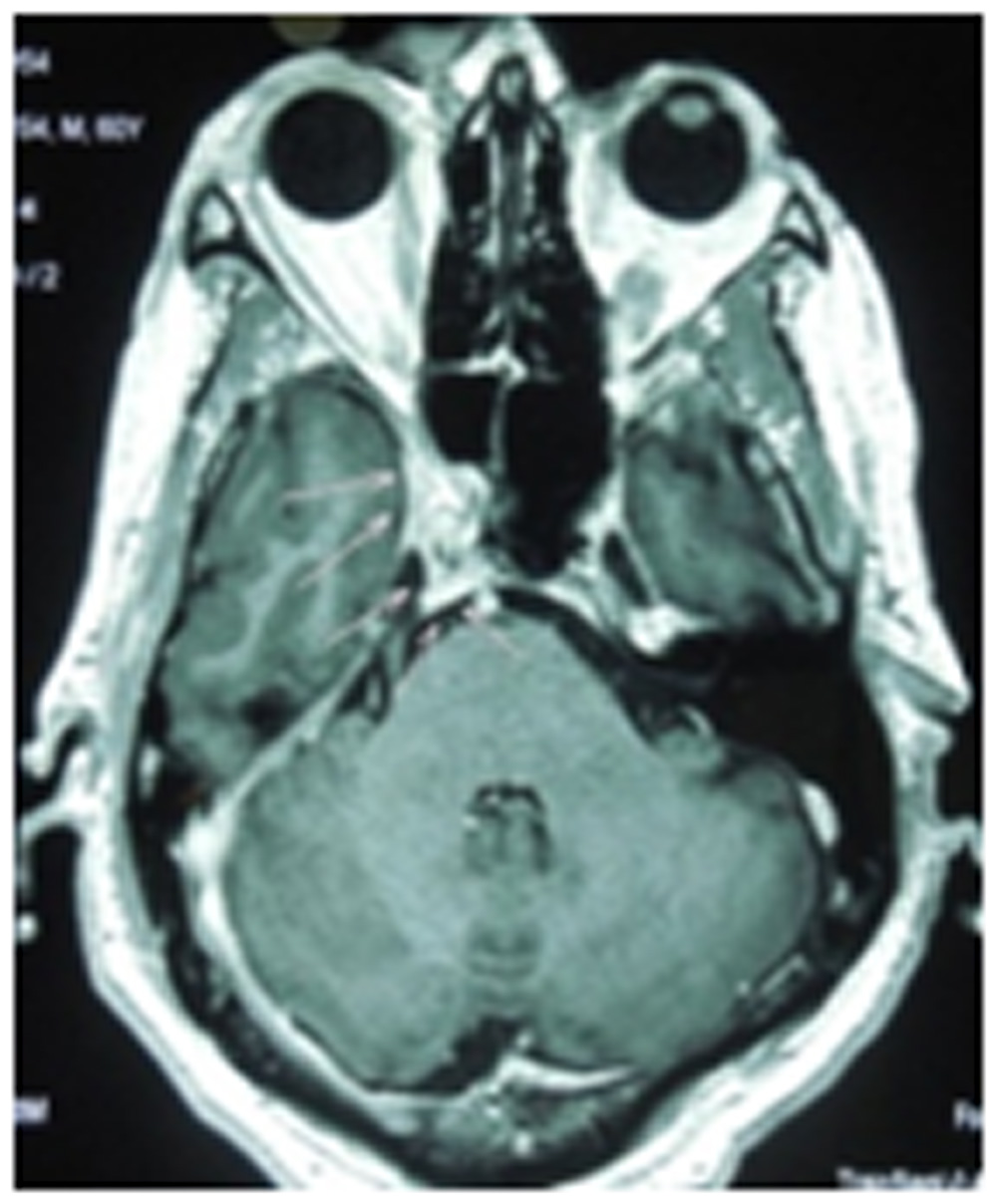
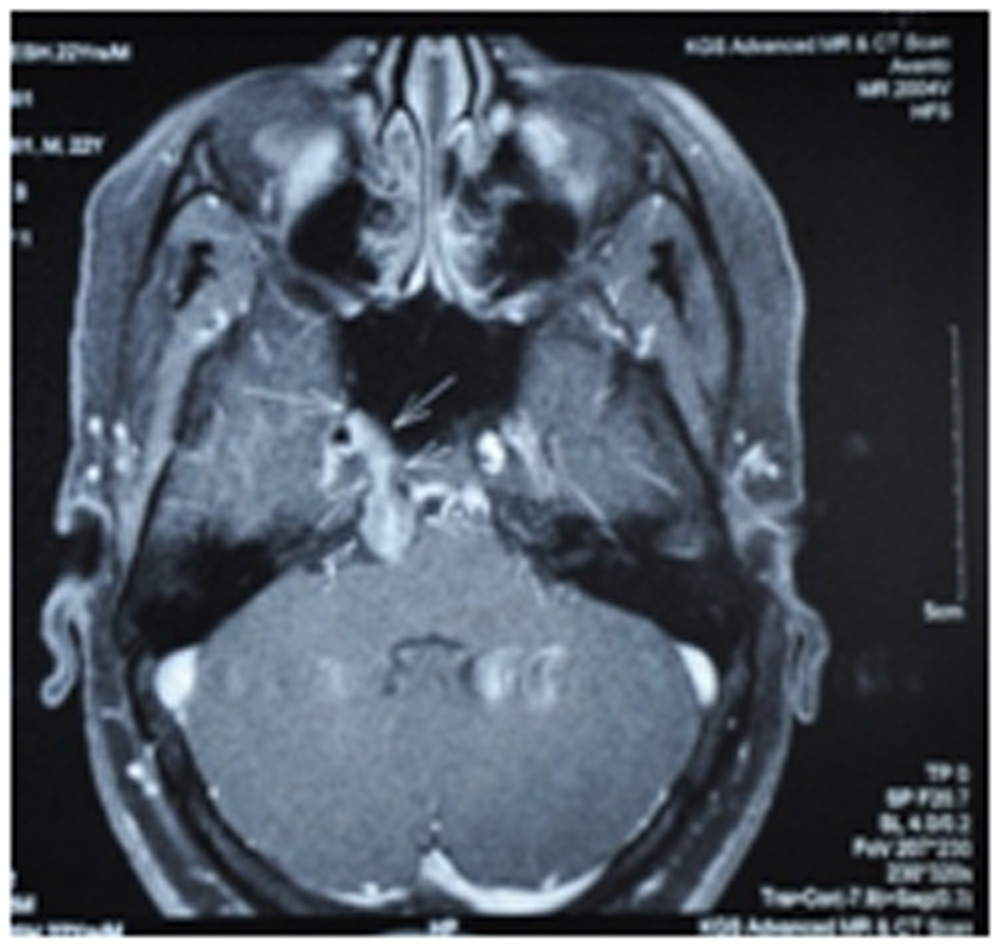
Fig 7-Sixth nerve Schwannoma
One plausible reason for diabetes being associated with a larger percentage of isolated sixth nerve palsy could be due to the higher incidence of type II diabetes in India (our study population) when compared to the United States (the population studied by Patel et al.): 14.3% versus 8.2%[2]. Patel SV et al, population based case– control method [7] to determine the risk of isolated sixth nerve palsy developing in the presence of diabetes mellitus or systemic hypertension. There was a 6-fold increase in odds of having diabetes in cases of sixth nerve palsy than in controls, whereas hypertension did not seem to be a significant association. Jacobson et al [8] conducted a case– control study at a referral centre assessing risk factors for third, fourth, and sixth nerve palsies. They also found diabetes to be an independent risk factor.
Majority of Microvascular ischaemic sixth nerve palsy resolved spontaneously. So observation, control of systemic condition and close follow up is necessary [2, 3, 4] till 3-6months.If not resolved, full neurological evaluation including neuroimaging should be done [2]. Traumatic sixth nerve palsy was treated conservatively with prisms for at least 6 months [2].Sixth nerve palsy due to tumour was referred to Neurosurgeon. Inflammatory nerve palsy was treated with steroids.
CONCLUSION
In the absence of risk factors, a suggestive history, or positive laboratory and clinical findings, neuroimaging can serve as a useful diagnostic tool in identifying the exact cause of sixth nerve palsy. We believe that by delaying an MRI in isolated non traumatic sixth nerve palsy, the risk of not diagnosing an intracranial tumor certainly exists. Neuroimaging for all patients presenting with a sixth nerve palsy is a costly management practice, as pointed out by Chi and Bhatti [1] and Murchison et al., [9] also routinely performed MRI in every patient with sixth nerve palsy in a developing country may not always be feasible and financially viable [1]. We largely favour the algorithms recommended by Miller et al. and Murchison et al. [4, 9]
Patients above the age of 50, with the presence of vasculopathic risk factors may be treated conservatively with management focusing on the underlying systemic condition; however, these patients in our opinion need to be monitored closely and depending on the recovery, the next step may be taken. Worsening, non improvement for a period of 3 months or greater and progressive involvement of other cranial nerves needs urgent neuroimaging. Furthermore, in patients >50 years of age, isolated sixth nerve palsy in the absence of vasculopathic risk factors requires neuroimaging. In patients below 50 presenting with isolated nontraumatic acute sixth nerve palsy we believe neuroimaging on presentation is warranted. Any history of a malignancy in the past or at presentation is a case of immediate neuroimaging.
The decision of whether to image or not in a case of nontraumatic, isolated acute sixth nerve palsy lies largely with the examining clinician and must be taken on a case to case basis depending on the index of suspicion. On the basis of our study, we propose the following algorithm for clinical evaluation and need of neuroimaging in isolated sixth nerve palsy [Fig 8]. However, given the varying incidence of vasculopathic and tumor related causes of sixth nerve palsy in India and in the above quoted studies, larger, prospective, crosssectional studies, to study the role of neuroimaging in acute sixth nerve palsy are warranted.
Isolated sixth nerve palsy
Ischaemic
Non ischaemic
Prior history of cancer
Age > 50 yrs
No
Yes
Yes
No
Diabetes
Hypertension
Hyperlipidaemia
Coronary Artery disease
Yes
No
Observation
Control of Systemic condition
Close follow up
Resolution at 3 months
Regular Follow up
Neuro Imaging
Yes
No
No improvement
Worsening
Involvement of other
cranial nerves
Fig-8
A proposed Algorithm for clinical evaluation and need of Neuro imaging in isolated sixth nerve palsy
REFERENCES
- Chi SL, Bhatti MT. The diagnostic dilemma of neuroimaging in acute isolated sixth nerve palsy. Curr Opin Ophthalmol 2009;20:423-9
- Patel SV, Mutyala S, Leske DA, Hodge DO, Holmes JM. Incidence, associations, and evaluation of sixth nerve palsy using a populationbased method. Ophthalmology 2004; 111:3693
- Tiffin PA, MacEwen CJ, Craig EA, Clayton G. Acquired palsy of the Oculomotor, trochlear and abducens nerves. Eye 1996; 10 (Pt. 3):377– 384.
- Miller RW, Lee AG, Schiff man JS, Prager TC, Garza R, Jenkins PF,et al. A practice pathway for the initial diagnostic evaluation of isolated sixth cranial nerve palsies. Med Decis Making1999; 19:424
- Rush JA, Younge BR. Paralysis of cranial nerves III, IV, and VI. Cause and prognosis in 1,000 cases. Arch Ophthalmol 1981; 99:76–79.
- Rush JA. Causes and prognosis in 4,278 cases of paralysis of the Oculomotor, trochlear, and abducens cranial nerves. Am J Ophthalmol 1992; 114:777–778.
- Patel SV, Holmes JM, Hodge DO, Burke JP. Diabetes and hypertension in isolated sixth nerve palsy: a population-based study. Ophthalmology 2005; 112:760–763.
- Jacobson DM, McCanna TD, Layde PM. Risk factors for ischemic ocular motor nerve palsies. Arch Ophthalmol 1994; 112:961–966.
- Murchison AP, Gilbert ME, Savino PJ. Neuroimaging and acute ocular motor mononeuropathies: A prospective study. Arch Ophthalmol 2011; 129:3015.
Leave a Comment