
Dr. Meena Chembil Kakkitampara, M11279, Dr. Sanitha Sathyan, Dr. Elizabeth Joseph
Abstract
Aim
To assess the site of horizontal extraocular muscle insertion from the limbus and to tailor recession values accordingly
Compare surgical outcome with a deviation and age matched group where surgical correction is based only on pre-operative measurement
Methodology
Retrospective observational study. Only patients who underwent surgery for horizontal strabismus were included. Patients wereassigned to 2 groups – in group 1 recession was done based on the pre-operative deviation; and in group- 2 the site of insertion site from limbus measured and recession values were tailored. Lateral rectus insertion at 7-7.5 mm and medial rectus at 5-5.5mm from limbus taken as normal. Post-operative deviation of the 2 groups was compared.
Results
Twenty five age, sex and deviation matched patients were included in each group. In group 2 lateral rectus insertion site ranged from 5-8mm and medial rectus 4-6mm from the limbus. In 9 exotropia and 4 esotropia patients of group 2 surgical measurements need to be tailored based on the limbus to insertion site difference. Two patients in both groups had 2nd stage surgery. Though statistically significant outcome in postoperative status between groups was not obtained no case of overcorrection with consecutive deviation was noted in group2.
Conclusion
Horizontal Extraocular muscle insertion site from the limbus is variable and not age dependent. Tailoring recession values based on this variable do have an added advantage on postoperative outcome
Key words
Exotropia, Esotropia, Limbus, Extraocular muscles
Millimeters = mm, LR- Lateral Rectus, MR- Medial Rectus
Introduction
Strabismus surgery is a procedure in ophthalmic practice where results are much dependent on your personal experience and where procedure needs much planning before deciding on a value to correct your deviation. Though the procedures on extraocular muscles are easy compared with the dexterity involved in intraocular surgeries, difficulties are mainly in judgment making as to when to; which muscle to; and how much of each muscle to operate. ⁽¹⁾ A high percentage of your expectations come true, but the dilemma arises when you are faced with a post-operative situation you never expected. So many factors like visual acuity, age of patient, associated refractive errors,pre-operative deviation etc., come into play to decide on the outcome. ⁽2,3,4) There are studies where the limbus is taken as the landmark for surgical correction. (5,6,7)However the relevance of the site of original insertion in tailoring surgical measurements is not widely studied.
Gross difference has been found between various studies on the site of extraocular muscle insertion from limbus. 8,9)Studies have shown that by processes of differential degeneration between the sclera and the rectus tendon, posterior recession of the tendon from the limbus, and contemporaneous growth of the anterior segment of the eye, the tendons ofextraocular muscle reach their adult location only between the ages of 18 months and 2 years. 9Thus, it is a known factor that in the early years of a growing eye the muscle position could be variable, but can this occur in later ages too and do all the insertionsregress and reach the expected position in the specified time?
Aim
To assess the site of horizontal extraocular muscle insertion from the limbusand to tailor recession values accordingly
Compare surgical outcome with a deviation and age matched group where surgical correction is based only on pre-operative measurement
Methodology
Retrospective observational study. Only patients who underwent recession on horizontal extra ocular muscles were included. All patients underwent routine preoperative workup which included vision assessment with age appropriate chart,strabismus evaluation which included assessment of extraocularmovements,motorevaluation with loose prisms using accommodative targets for distance and near,sensory evaluation done with worth4 dot test, TNO charts in cooperative and comprehensive subjects. Cycloplegic refraction done in all and patients with high refractive errors were excluded. All refractive error issues were addressed with glasses. Patients were assigned into 2 groups. Group 1 –here surgery was done based on the pre-operative deviation alone. In group 2 muscle recession was tailored based on the insertion site distance; for example, if a 7mm recession was planned but lateral rectus insertion was seen at 5mm from limbus, then the recession measurement was reduced accordingly. All procedures done by a single surgeon (EJ). With previous experiences of measuring the distance of insertion of the horizontal rectus muscle from limbus in the present study, medial rectus insertion at 5-5.5mm and lateral rectus insertion at 7-7.5mm was taken as normal.Measurements were done using Castroviejo calipers intraoperative. In cases of anterior insertion, the planned measurements were corresponding to the amount of change. For example, if 7mm recession was planned in an exotropia and lateral rectus was seen at 5mm from limbus the recession was reduced to 5- 5.5 mm. Similarly, in posterior insertion it was increased. All patients had uneventful postoperative periods and were on topical steroids and antibiotics for 3 weeks. Review was at 1 month, 3 months and subsequently 6 monthly follow-ups.Minimum follow-up period was 3 months range 3 -12 months. Post operatively all patients underwent the same orthoptic evaluation as was done preoperatively.
Results
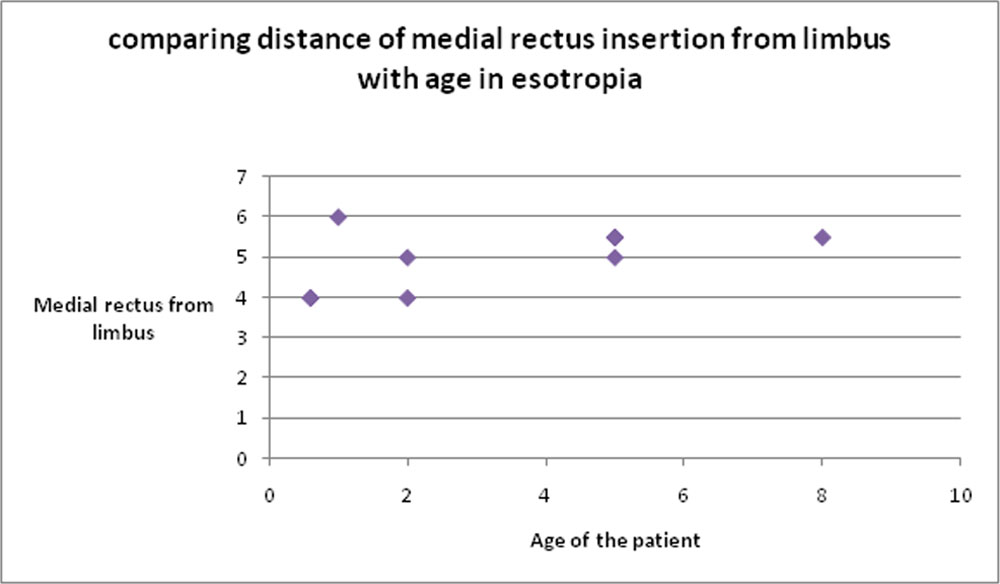
Twenty five 25 patients were included in each group. Mean age was 5.7 +/- SD years in group 1 with range of 2-30 years; and 5.2 +/- SD years with a range of 8months -32years in group2. 14exotropia and 11esotropia in group1; 16 exotropia and 9 esotropia in group2. Twelve males and13females were in group1;Tenmales and 15 females were in group 2. Preoperative deviation ranged from 60 to30 (it should be 30-60 prisms) prisms in group1 and 60 to 20 prisms (here it should be 20-60 (prisms) in group 2.The site of lateral rectus insertion ranged from 5 to 8 mm and medial rectus ranged from 4-6 mm from limbus in group 2.Figure 1 and 2 show muscle insertion sites in relation to age in exotropia and esotropia respectively.
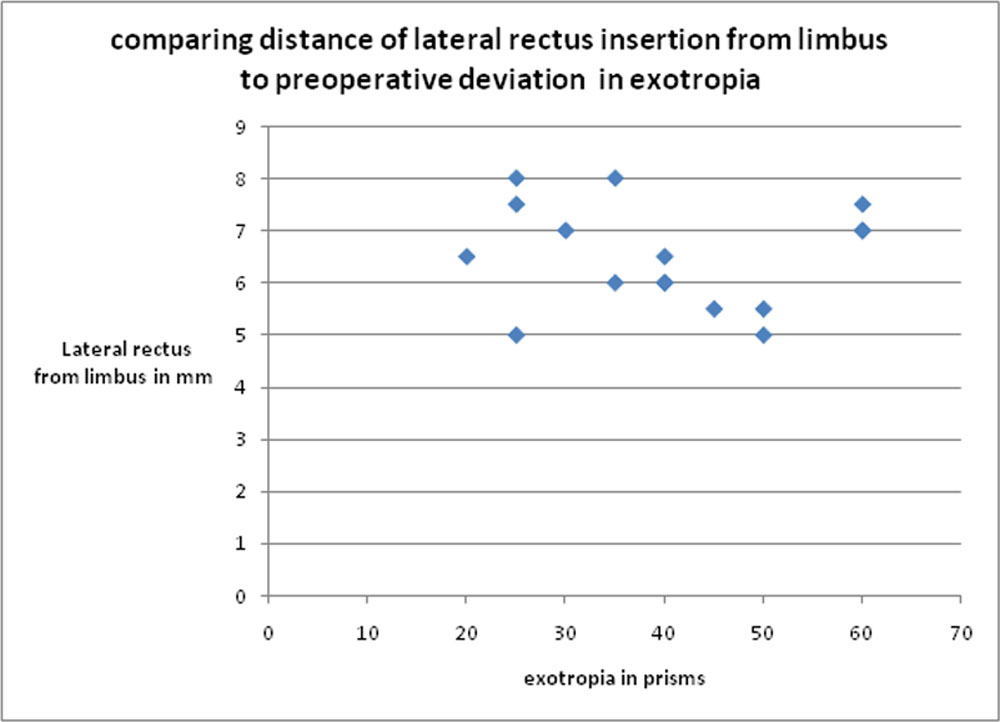
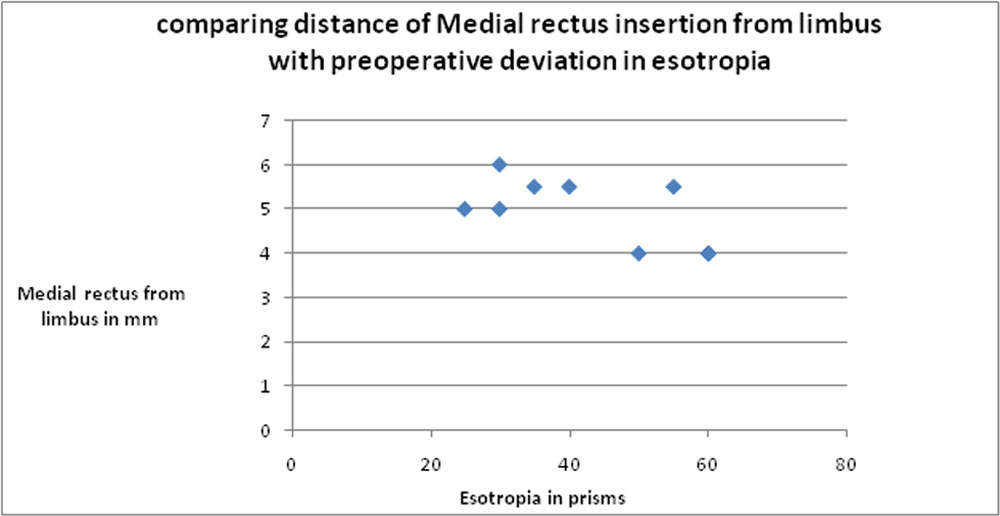
In 9 cases of exotropia and 4 cases of esotropia,the planned measurements were changed as the muscles were not in the expected position. Site of muscle insertion in comparison to deviation in exotropia and esotropia as are shown in figure 3 and 4 respectively were no association to the amount of deviation and insertion site could be made out.
Post-operative status of 7 patients in group 1 were not at expected level; that is, it was not within 10 prisms, of which 6 were exotropia and one was esotropia patient. Of these 6 exotropes,4 had overcorrection and 2 of these overcorrected cases underwent re-surgery. The other 2 cases had variable overcorrection prisms with long periods of orthotropia, and so, were observed. Two cases of under-correction were in the range of14-16 prisms and a single case of esotropia with under-correction was within 20 prisms.
Group 2 had 5 cases with residual deviation of which 3 were exotropes and 2 esotropes; there was not a single case of overcorrection. One case each of residual esotropia and exotropia underwent re-surgery. The esotropewas a large angle of 60 prisms in a 2 year old with no refractive error and the exotropia was in an adult of 32 years who had undergone bilateral recession of 8 mm for a 40 prism exotropia.Both were orthotropic after the second procedure. Of the 2 residualexotropia, 1 was a mentally challenged child and the other patient had extremely thin atrophic muscles, both had residual of 20 prisms of exotropia. The case of residualesotropiahad a preoperative deviation of 50 prisms and had +2 hyperopia associated and is kept under observation withglasses in view of the young age of 8 months and the associated hyperopia.
Statistical analysis
Mann Whitney U-test to compare the Post Operative deviation between
Group I and Group II
| Mann Whitney U | z value calculated from U value | p-value | |
| 254 | 1.324 | p > 0.05 |
Since the p-value greater than 0.05, we are not able to reject H0 at 5% level of significance. So there is no significant difference between Group I and Group II in comparison of post Operative deviation.
Statistical analysis comparing the postoperative outcome of the 2 groups could not achieve significance.However, no over corrections observed in group 2.
Discussion
Surgery on the extra ocular muscles involves meticulous preoperative workup and is a procedure where your judgmental skills cannot be at the spinal level as each case needs to be approached individually. Yet another challenge in strabismus surgery is the postoperative results which are so obvious to the patient and associates in the immediate postoperative period.
The site of insertion of the extra-ocular muscle has been studied by various authors and has come up with highly variable values and ranges. However in strabismus surgery where each mm of your surgical correction is accountable it is almost impossible to adhere to such wide ranges. It is a known fact that the learning curve in strabismus surgery is more for your caliper measurements than for the real surgical technique and each surgeon develops one’s own standard with experience. It is also a known fact that one cannot achieve orthotropia in all cases, and in spite of years of experience still can end up with over corrections and under-correction, of which, the former is a situation no surgeon would like to encounter.
D Sevels in his study on extra ocular muscles,(9) has mentioned that the adult location is reached only by the age of 18 months to 2 years and the insertion site of medial and lateral rectus varied from 3-5.5 and 3-6.5 with age respectively. However in our study we were unable to demonstrate such a situation and of the 7 children less than 2 years in group 2 only 3 had their insertion anterior, which included 2 cases of esotropia and a single case of exotropia. The oldest participant in group 2 had lateral rectus insertion at 6mm and the anterior most insertion of lateral rectus was 5 mm which was seen in a 1 year and 8 year old , and this lead us to the conclusion that the site of insertion is highly unpredictable and not age dependent.
Liu X et al in their study,(10) on comparing the site of insertion of medial rectus and lateral rectus fromlimbus with anterior segment OCT and intraoperative calipers got a range of 4.5-6.1mm and 5.5- 7.5mm respectively. This study was done on strabismus patients and the values mentioned were comparable to our measurements of 4-6mm for medial rectus and 5-8mm for lateral rectus from limbus.
Though the course and thickness of extraocular muscles in high myopia has been studied extensively,(11,12)literature on the site of insertion of these muscles in high refractive errors is sparse. Since in high axial myopia and hyperopia the globe size is involved we concluded that the insertion site of the muscle could be variable hence cases of high refractive errors were not included in the study.
There are surgeons who advise limbus to be taken as the landmark for recession values,(13) but on logical thinking one is dealing with a muscle which is functioning from a particular distance from the limbus and our aim should be to weaken it depending on the preoperative deviation and position, hence the original insertion does have great value.The main incentive to assess the insertion site was the unexpected overcorrection beyond acceptable levels in group 1. In patients who underwent a 2nd procedure in group 1 to correct their deviation,on assessing their insertion site during the second surgery, it was found to be quite anterior and the possibility of a slipped muscle was also ruled out.
In 9 cases of exotropia and 4 cases of esotropia in group 2, the planned recession values were changed as the muscles were not in the expected position. The 2 cases of under-correction of esotropia were children of 8 months and 2 years with large angle esotropia and also there was hyperopia of +2 in the former. For these cases, in view of the young age, our assessment was by modified Krimsky method and the preoperative deviation was also borderline for a 3-muscle surgery. Only one of these under-correctedesotropiapatient, needed a second procedure and was orthotropic postoperatively.Of the 3 under-correctedexotropes, only 1 case needed a second surgery for a residual deviation of 25 exotropia.Thus,inalmost all the unfavorable outcomes in group 2 we could explain the situation and could reason out unlike in group 1 patients.
In our study, we also observed that the insertion of the lateral rectus had more variability in relation to the limbus than the medial rectus, also since most of the exotropia’s are intermittent unlike esotropia’s, extra care need to be exercised in such procedures not to convert an intermittent deviation to a constant one.
There are reports on considering anatomical landmarks to decide on strabismus surgery values andseveral authors have tried to develop guidelines to dose the amount of correction achieved per mm of surgery on the extra-ocular muscles.(14,15)Few publications talk about placing the muscle insertion with relation to certain points on the circumference like the equator, while others give limited importance to axial length and equator calculations.(16)
Kushnar B J et al in their study on the maximum recession value that can be safely done on medial rectus has mentioned that muscle can be recessed beyond equator to a certain extent. 17
Though we could find in literature various factors which could bepredictive forsurgical outcome the importance of the original insertion and variability has not been talked about. Though we could give importance to this variable only secondary to all other predictive factors like age, visual acuity, refractive error, preoperative deviation etc., the site of original insertion does hold a position in the list and should be considered when deciding on your recession values. The main limitation of the study is the small sample size and the bias in selecting cases in group 1, this could also probably explain the statistical insignificance of the study.
Conclusion
Horizontal extraocular muscle insertion distance from limbus is variable with anterior and posterior insertions possible even at young ages. The insertion distance should definitely be considered when deciding on your recession values along with other factors like age, refractive errors, preoperative deviation etc.Tailoring recession values based on this variable do have an added advantage on postoperative outcome.
References
1. Hermann M.BurianM.D.The Principles of Surgery on the Extra ocular Muscles*: Part 1 Fundamental Principles: Choice of Operation in Concomitant Strabismus: Horizontal Muscles. American Journal of OphthalmologyVolume 33, Issue 3, Part 1, March 1950, Pages 380-387
2.Kampanartsanyakorn S, Surachatkumtonekul T, Dulayajinda D, Jumroendararasmee M, Tongsae S The outcomes of horizontal strabismus surgery and influencing factors of the surgical success.J Med Assoc Thai. 2005 Nov;88Suppl 9:S94-9.
3.Gezer A, Sezen F, Nasri N, Gözüm N.Factors influencing the outcome of strabismus surgery in patients with exotropia.JAAPOS. 2004 Feb;8(1):56-60.
4.NamitaKumari, Abadan Khan Amitava, Mohammad Ashraf, Shivani Grover, Ashiya Khan, and PrabhaSonwaniPrognostic preoperative factors for successful outcome of surgery in horizontal strabismus..Oman J Ophthalmol. 2017 May-Aug; 10(2): 76–80
5.Kushner BJ, Lucchese NJ, Morton GV.Variation in axial length and anatomical landmarks in strabismic patients. Ophthalmology. 1991; 98:400–6.
6.Xiaoqiang Liu; Fang Wang; Ying Xiao; Xinhai Ye; LijieHou.Measurement of the Limbus-Insertion Distance in Adult Strabismus Patients with Anterior Segment Optical Coherence Tomography. Eye Movements, Strabismus, Amblyopia and Neuro-ophthalmology | October 2011
7.Scott R. Lambert, Christopher J. Lyons – 2016Taylor and Hoyt’s Pediatric Ophthalmology and Strabismus E-Book
8.SunitaAthavale, SheetalKotgirwar, RekhaLalwani.Rectus and oblique muscles of eyeball: a morphometric study of Indian population ttp://dx.doi.org/10.5115/acb.2015.48.3.201pISSN 2093-3665 eISSN 2093-3673
9.D Sevel. The origins and insertions of the extraocular muscles: development, histologic features, and clinical significance.Trans Am Ophthalmol Soc. 1986; 84: 488–526
10.Liu X1, Wang F, Xiao Y, Ye X, Measurement of the limbus-insertion distance in adult strabismus patients with anterior segment optical coherence tomography.HouLInvestOphthalmol Vis Sci. 2011 Oct 28;52(11):8370-3.doi: 10.1167/iovs.11-7752.
11.Yoshiko Aoki, MDYasuhiroNishidaMD,Osamu Hayashi, MD,Jiro Nakamura, MD,SanaeOda, MD,ShinichiYamade, MD,KazutakaKani, MD. Magnetic resonance imaging measurements of extraocular muscle path shift and posterior eyeball prolapse from the muscle cone in acquired esotropia with high myopia. American journal of ophthalmology September 2003Volume 136, Issue 3, Pages 482–489
12.Pierro L. · Zaganelli E. · Tavola A. · MuragliaM.Extraocular Muscle Size Comparison between Normal and Myopic Eyes Using Standardized A Scan Echography..Ophthalmologica 1998;212(suppl 1):22–24
13.Taylor and Hoyt’s Pediatric Ophthalmology and Strabismus E-Bookhttps://books.google.co.in/books?isbn=0702066176
14.von Noorden GK, Campos EC. 6th ed. St. Louis, MO: CV Mosby; 2001.Principles of surgical treatment. In: Binocular Vision and Ocular Motility: Theory and Management of Strabismus; pp.571–3.
15.Rosenbaum AL, Santiago AP. Philadelphia, PA: WB Saunders Company; 2001. Surgical Dose Tables. In: Clinical Strabismus Management Principles and Surgical Techniques; p. 553.
16.Kuscher BJ, Fisher MR, Lucchese NJ, Morton GV. Factors influencing response to strabismus surgery. Arch Ophthalmol. 1993;111:75.
17.Kushner BJ, Fisher MR, Lucchese NJ, Morton GV. How far can a medial rectus safely be recessed? J PediatrOphthalmol Strabismus. 1994; 31:138–46. discussion 151-2
FIGURES
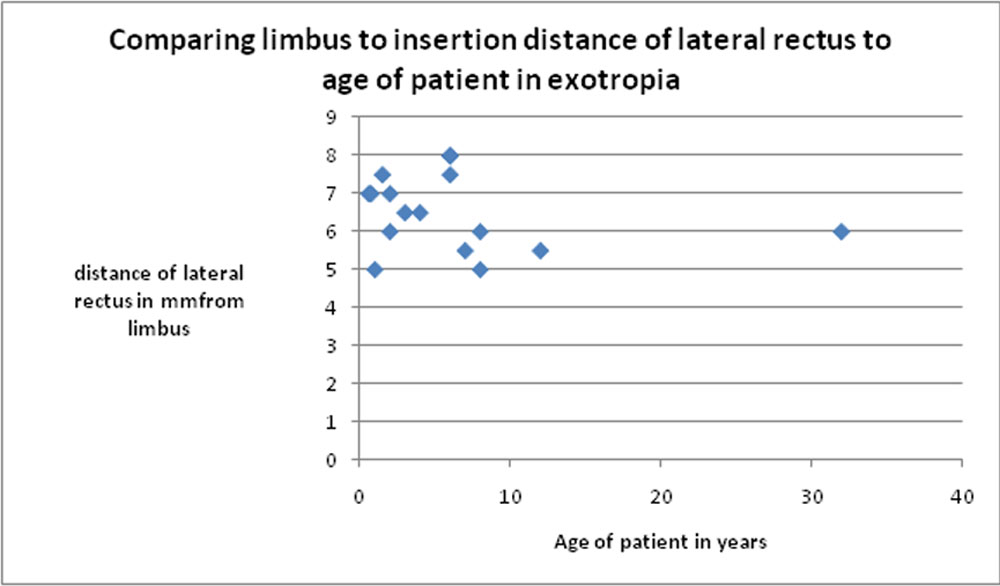
FIGURE 2
(FIGURE 3)
 (FIGURE 4)
(FIGURE 4)
Leave a Comment