
Dr. Praveen Vashist, V11693, Dr. Vivek Gupta, Dr. Noopur Gupta Parakh, Dr. Suraj Singh Senjam
Abstract:
To understand attrition among known diabetics (KDs) referred for free diabetic retinopathy (DR) management to the base hospital in a DR screening program.
We referred 1136participantsincluding 918(80.8%) with mild/moderate Non-Proliferative DR (NPDR), 92(8.1%) severeNPDR, 77 (6.8%) Proliferative DR and 49(4.3%) having Diabetic Macular Edema (DME). Successful referral rate was 36.9% (95% CI 33.4-40.7). Females (adjusted odds ratio[OR]=0.6) and cases aged ≥60 years (aOR 0.7) had significantly higher attrition rate (p-value < 0.01). Presenting visual acuity, diabetes duration, systemic complications and glycemic control were not associated with attrition. A non-significant trend towards increasing referral success with worsening DR stage (mild NPDR 31.6%, moderate NPDR 38.3%, severe NPDR 42.4%, PDR 40.3%, DME 44.9%) was observed.
The rates of successful referrals in DR screening program are low and can potentially be improved by targeting elderly female patients.
INTRODUCTION
Blindness and visual impairment is a major public health issue that disproportionally affects larger populations in developing nations.[1] Over years, global blindness control efforts in developing nations have focused on causes of avoidable blindness particularly cataract and refractive error.With the stabilization of blindness control efforts and riding the wave of epidemiological transition, blindness due diabetic retinopathy (DR) is increasing. DR is responsible for 2.6% of global blindness.[2,3] If affects 34.6% of all patients with type 2 diabetes mellitus (T2DM) and 10.2% of all diabetics have vision-threatening DR.[4] A systematic review of studies from India concluded that 18.1% of known diabetics aged ≥50 years had DR.[5] DR is the fifthleading cause of blindness in India, and has been included as a priority disease in Vision 2020: The Right to Sight India.[6]Considerable efforts have been devoted worldwide and in India for developing DR screening programs.The potential role of DR screening program is well established in the management of DR.[7]The desired final outcome for participant in these screening programs is early and appropriate management of DR and prevention of vision loss based on the concept of lead-time. Infrastructure for detailed investigations and treatment of patients with DR is often not available in community based screening and the screened positive patients need to visit the base hospital. This step is a potential weak link in DR screening programs. We present our experience with post-referral attrition among known diabetics identified through community based DR screening program in urban slums of Delhi.
MATERIALS AND METHODS
This program was implemented from January 2013-June 2014in slums of the National Capital Territory Delhi. The slum population consisted mainly of migrant daily wage workers, rag pickers, and skilled and unskilled workers. There are 350 slums in Delhi of which 70 slums were selected for our screening program.
Participants were eligible for screening if they were 40 years or above of age and were known diabetics (KD) defined as: available records of fasting blood glucose ≥ 126mg/dl, or (ii) random blood glucose ≥ 200 mg/dl, or (iii) patient using oral hypo-glycemic or insulin. There were no exclusion criteria. KDs were identified in the community by active survey, through non-governmental organization (NGO) volunteers and self-referrals through publicity. (Figure1)Pre-scheduled DR screening camps were organized in the vision centres, local government dispensaries or local schools that were easily accessible by the slums. One field worker, one laboratory technician, one dietician, two volunteers and two trained optometrists were involved in each DR screening camp. Activities during the camp included assessment of risk factors, clinical evaluation and ocular evaluation for DR.Information about duration of diabetes and other complications related to diabetes (neuropathy and nephropathy, other associated systemic disorders) was also collected. Health awareness talks about prevention of DR were also done. A dietician gave health talks on diabetic diet and healthy life style. A laboratory technician measured blood pressure using a sphygmomanometer (Omron SEM-1 HEM-7051-C12). Height (in cm) and weight (in kg) of all KDs was measured and body mass index (BMI) calculated. Random capillary blood sugar was measured with a glucometer by finger prick method. It was noted if the patient was overnight fasting.
Assessment of presenting visual acuity was done using Snellen’s chart. This was followed by fundus photography using non mydriatic fundus camera. A portable handheld camera with retinal module (Pictor, Volk Optical, Inc. Mentor, OH, USA) was used to take paired images of fundus. The trained optometrist viewed these images on laptop and graded the diabetic retinopathy according to International Clinical Diabetic Retinopathy Scale (Table 1).[8]Patients diagnosed with any DR were counselled, and referred to our tertiary care eye hospital. At the base hospital, provision of free investigations and treatment of all referred patients was made. A social workers and optometrist posted at the base hospital were responsible for coordinating the patients visit. They also maintained a record of each visit and the nature of investigations and treatment provided.
All the data was entered in Microsoft AccessTMdatabase.Duration of diabetes was categorized as under 5 years, 6-10 years and over 10 years. A participant who reported any cardiovascular, neurological or renal comorbidities was classified as suffering from co-morbidities. Presenting distance visual acuity was categorized as ≥ 6/12, < 6/12 – 6/18, < 6/18-6/60, < 6/60 -3/60 and < 3/60 based on better eye vision and worse eye vision. If measured fasting blood glucose was ≥ 126mg/dl, or random capillary blood glucose was ≥ 200 mg/dl, participant was classified as having uncontrolled diabetics. Successful referral was defined as a patient screened positive for DR and reaching the base hospital while patients who did not report to based hospital were considered as attrition. The data was exported to Stata version 14 (Stata Corp, College Station, TX) for statistical analysis. A p-value of less than 0.05 was considered statistically significant.
RESULTS
Identifying Known Diabetics
We organized 277 DR screening eye camps, and 9435 KDs attended these camps. Of these 9435 participants, 8566 (90.8%) underwent non-mydriatic fundus photography and in 8432 (98.4%) participants, DR grading could be done. (Figure 3) DR was identified in 1136 (13.5%, 95% CI=12.5-14.1) participants of whom 497 (43.8%) were males, 340 (15.2%) had family history of diabetes, 791 (16.9%) had uncontrolled diabetes, and 198 (20.6%) reported systemic complications related to diabetes. Among referred cases, 351(30.9%) had mild NPDR, 567(49.9%) had moderate NPDR, 92(8.1%) had severe NPDR, 76(6.7%) had PDR and 49(4.4%) had diabetic macular edema. (Figure 1)
Post-referral attrition and its risk factors
Successful referrals were achieved in 420 (36.9%, 95% CI 33.4-40.7) cases and a high post-referral attrition of 63.1% was observed. The rate of successful referrals was significantly higher amongst males (44.5%) and among participants aged<60 years (40.8%). Diabetes duration, systemic complications and glycemic control were not associated with attrition. A non-significant trend towards increasing referral success with worsening DR stage (mild NPDR 31.6%, moderate NPDR 38.3%, severe NPDR 42.4%, PDR 40.3%, and DME 44.9%) was observed.Referred cases having severe visual impairment or blindness (presenting visual acuity< 6/60) had an attrition rate of 60.3% and the association between visual acuity and attrition was not statistically significant.
Amongst these 420 participants visiting the tertiary care hospital 315 underwent fundus examination, 344 underwent optical coherence topography, 126 participants underwent fundus fluorescein angiography,34 underwent laser photocoagulation, 20 underwent intraocular injections in the form of posterior subtenons or intravitreal AvastinTM.
DISCUSSION AND CONCLUSION
We had a unique program offering end-to-end service ranging from free DR screening to free treatment in an urban slum population. Through our program, we could do staging of DR patients, provide them an immediate diagnosis and refer them to a tertiary care eye hospital. We observed 13.5% prevalence of DR among cases of T2DM, similar to the observation in urban slums of Mumbai where 14.5% of diabetics had DR.[9]In spite of offering free treatment in a well-respected public sector tertiary eye care hospital, we observed high attrition rates among referred cases. Over half of cases did not reach base hospital. While the results indicate that females and older individuals require special efforts/ intervention to ensure successful referrals, the low rates across the board indicate that much efforts are required in all ages and across both genders.Aleo et al. evaluated use of patient contracts to improve follow-up adherence among screened diabetic patients but concluded that contract were not helpful.[10]While previous studies have identified interventions that promote screening of diabetic retinopathy and adherence to annual eye examination among diabetics, we were unable to identify studiesreporting post-referral attrition in developing country context.[11–13]Studies on cost effectiveness of DR screening too have often focused on cost per case of DR detected and have ignored post-referral attrition.[14]
Our study does have its limitations.Being limited by programmatically collected data, we are unable to exactly specify the reasons for attrition directly elicited from the patients. This warrants further exploratory or qualitative studies. It is possible that DR is not considered a priority by the population, possible due to low awareness of DR which has been reported.[15]Another competing factor could be the fear of loss of wages in the target population of the program. Numerous DR screening programs are in place using various approaches like community based screening and tele-ophthalmology based.Addressing post-referral attrition in DR screening programs must be a priority if to improve the cost-effectiveness of such programs.
REFERENCES
- Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol 2012;96(5):614–8.
- Ting DSW, Cheung GCM, Wong TY. Diabetic retinopathy: global prevalence, major risk factors, screening practices and public health challenges: a review. Clin Experiment Ophthalmol 2016;44(4):260–77.
- Bourne RRA, Stevens GA, White RA, Smith JL, Flaxman SR, Price H, et al. Causes of vision loss worldwide, 1990–2010: a systematic analysis. Lancet Glob Health 2013;1(6):e339–49.
- Yau JWY, Rogers SL, Kawasaki R, Lamoureux EL, Kowalski JW, Bek T, et al. Global Prevalence and Major Risk Factors of Diabetic Retinopathy. Diabetes Care 2012;35(3):556–64.
- Jotheeswaran AT, Lovakanth N, Nadiga S, Anchala R, Murthy GVS, Gilbert CE. Estimating the proportion of persons with diabetes developing diabetic retinopathy in India: A systematic review and meta-analysis. Indian J Endocrinol Metab 2016;20(Suppl 1):S51–8.
- John N, Jose R, Vashist P, Murthy GVS, RAAB India Study Group. Rapid Assessment of Avoidable Blindness in India. PLoS ONE 2008;3(8):e2867.
- Vashist P, Singh S, Gupta N, Saxena R. Role of Early Screening for Diabetic Retinopathy in Patients with Diabetes Mellitus: An Overview. Indian J Community Med Off Publ Indian Assoc Prev Soc Med 2011;36(4):247–52.
- Wilkinson CP, Ferris III FL, Klein RE, Lee PP, Agardh CD, Davis M, et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 2003;110(9):1677–82.
- Sunita M, Desai S, Vinay P, Moolani S, Rai N, Deepen S, et al. Aditya Jyot-Diabetic Retinopathy in Urban Mumbai Slums Study (AJ-DRUMSS): study design and methodology – report 1. Ophthalmic Epidemiol 2014;21(1):51–60.
- Aleo CL, Murchison AP, Dai Y, Hark LA, Mayro EL, Collymore B, et al. Improving eye care follow-up adherence in diabetic patients with ocular abnormalities: the effectiveness of patient contracts in a free, pharmacy-based eye screening. Public Health 2015;129(7):996–9.
- Zhang X, Norris SL, Saadine J, Chowdhury FM, Horsley T, Kanjilal S, et al. Effectiveness of Interventions to Promote Screening for Diabetic Retinopathy. Am J Prev Med 2007;33(4):318–35.
- Sheppler CR, Lambert WE, Gardiner SK, Becker TM, Mansberger SL. Predicting Adherence to Diabetic Eye Examinations: Development of the Compliance with Annual Diabetic Eye Exams Survey. Ophthalmology 2014;121(6):1212–9.
- Lin S, Ramulu P, Lamoureux EL, Sabanayagam C. Addressing risk factors, screening, and preventative treatment for diabetic retinopathy in developing countries: a review. Clin Experiment Ophthalmol 2016;44(4):300–20.
- Pasquel FJ, Hendrick AM, Ryan M, Cason E, Ali MK, Narayan KMV. Cost-effectiveness of Different Diabetic Retinopathy Screening Modalities. J Diabetes Sci Technol 2016;10(2):301–7.
- Hussain R, Rajesh B, Giridhar A, Gopalakrishnan M, Sadasivan S, James J, et al. Knowledge and awareness about diabetes mellitus and diabetic retinopathy in suburban population of a South Indian state and its practice among the patients with diabetes mellitus: A population-based study. Indian J Ophthalmol 2016;64(4):272–6.
Table 1: Factors associated with successful referrals to base hospital among patients identified with diabetic retinopathy in a community based screening program
| Patients Referred | Adjusted Odds Ratio | ||||
| Reported | Not Reported | Total | Odds Ratio | P Value | |
| Total | 420 (37.0) | 716 (63.0) | 1,136 | – | – |
| Gender | |||||
| Male | 221 (44.5) | 276 (55.5) | 497 | 1 | |
| Female | 199 (31.1) | 440 (68.9) | 639 | 0.6 (0.4-0.7) | <0.001 |
| Age | |||||
| <60 years | 239 (40.8) | 347 (59.2) | 586 | 1 | |
| ≥60 years | 181 (32.9) | 369 (67.1) | 550 | 0.7 (0.5-0.9) | 0.004 |
| Family History | |||||
| Yes | 137 (40.1) | 203 (59.7) | 340 | 1 | |
| No | 280 (35.5) | 508 (65.5) | 788 | 0.9 (0.6-1.1) | 0.311 |
| Duration of Diabetes | |||||
| <5 Years | 108 (32.6) | 223 (67.4) | 331 | 1 | |
| 05-10 Years | 165 (38.9) | 259 (61.1) | 424 | 1.3 (1.0-1.8) | 0.062 |
| >10 Years | 147 (38.6) | 234 (61.4) | 381 | 1.3 (0.9-1.8) | 0.107 |
| DR Stage | |||||
| Mild NPDR | 111 (31.6) | 240 (68.4) | 351 | 1 | |
| Moderate NPDR | 217 (38.3) | 350 (61.7) | 567 | 1.3 (1.0-1.8) | 0.057 |
| Severe NPDR | 39 (42.4) | 53 (57.6) | 92 | 1.6 (1.0-2.6) | 0.072 |
| PDR | 31 (40.3) | 46 (59.7) | 77 | 1.2 (0.7-2.0) | 0.559 |
| DME | 22 (44.9) | 27 (55.1) | 49 | 1.8 (0.9-3.3) | 0.071 |
| Presenting Visual Acuity in Better Eye | |||||
| 6/6-6/18 | 311(36.9) | 532(63.1) | 843 | 1 | |
| 6/24-6/60 | 78(36.4) | 136(63.6) | 214 | 1.0 (0.7-1.5) | 0.914 |
| <6/60 | 31(39.7) | 47(60.3) | 78 | 1.2 (0.6-2.1) | 0.591 |
| Complications | |||||
| No Complication | 341 (36.4) | 597 (63.6) | 938 | 1 | |
| Complications | 79 (39.9) | 119 (60.1) | 198 | 1.1 (0.8-1.6) | 0.44 |
| Blood Sugar Control | |||||
| Controlled | 131 (38.9) | 206 (61.1) | 337 | 1 | |
| Uncontrolled* | 288 (36.4) | 503 (63.6) | 791 | 0.9 (0.6-1.1) | 0.284 |
*Uncontrolled if Fasting capillary sugar >126 mg/dl or random sugar >200 mg/dl
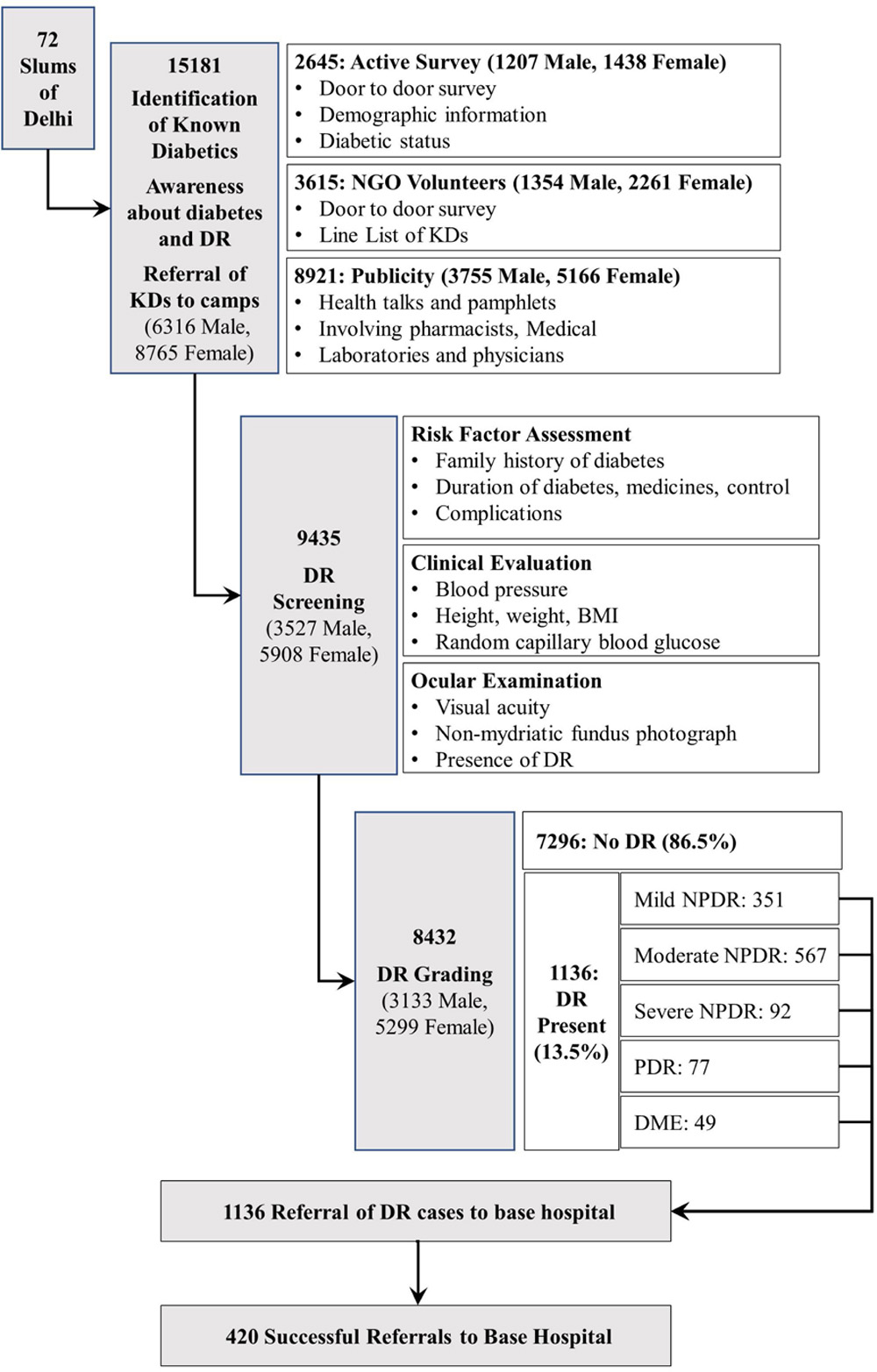
Figure 1: Participant flow-chart representing case identification, screening and referral successes in a community based diabetic retinopathy screening program for residents of urban slums of Delhi
Leave a Comment