
Dr. Joyeeta Das, D11894, Dr. Nibedita Das
Abstract :
Aim:
To study the characteristics of Spectral domain AS-OCT imaging of lacrimal punctum and vertical canaliculus of normal subjects
Methods :
Prospective observational cross sectional study on 50 asymptomatic subjects underwent SD-ASOCT imaging of both lower lid punta(n=100). External and internal punctal diameter,vertical depth ,proximal vertical canaliculi depth measured and statistically analyzed
Results:
Mean external and internal Punctal diameter 432.02µm ±128.77 ,133.22 ± 33.132 µm respectively.Mean vertical punctal depth 332.77 ± 48.04 µm , proximal vertical canaliculi depth 919 ± 196.23µm. Significant gender difference found only in punctal depth (p=0.0021).Seven morphological variant with tear film and hyper reflective debris found in 77% and 21% puncta respectively.External punctal diameter strongly showed strong agreement between clinical grading of puncta by masked observer.
Conclusion :
SD-ASOCT provides high resolution in-vivo imaging of proximal lacrimal system which will help clinician to manage proximal lacrimal disorders like punctal stenosis and designing of punctal plug devices.
Full text :
Introduction:
Epiphora or excessive tearing is one of the most common complaint encountered by ophthalmologist in their practice. Though epiphora is a multifactorial entity prevalence of exclusive punctal stenosis ranges from 11 to 19% [1,2]. In clinical practice diagnosis of punctal stenosis often missed due to lack of availability of standard diagnostic test or imaging. In past Punctal grading was done by slit lamp examination with or without computer based cursor driven measurement which had wide subjective variability.[3]. Punctal grading system proposed by Kashkouli et al [4] which requires insertion of Bowman probe of various sizes to measure the diameter has fallacy of stretching of puncta by punctal dilator prior to probing leading to inaccurate measurement of punctal diameter.
Normal diameter of lacrimal punctum varies from 200 to 500 micron which are mainly derived from ex vivo studies of cadaver which are unlikely to capture the true morphology of punctum due to tissue shrinkage [Kakizaki et al. 2008, 2012] [7]. Actual measurements and morphology of functioning puncta in physiological condition are still lacking in ophthalmic literature .Due to wide variability of size and shapes of normal puncta [5] it is difficult to determine whether it is normal variant or pathological stenosis.
These necessities need of development of a imaging techniques that would measure lacrimal puncta in vivo. First demonstration of high resolution imaging of lacrimal punctum and proximal canaliculi by anterior segment Optical coherence tomography [AS-OCT ]done by Wawrzynski et al.[6] in small sample group [n=36] Later Kamal et al ,Timlin et al published separate results of lacrimal puncta AS-OCT in different subsets of population using different types of OCT like FD-OCT or SD -OCT.
However there is lack of uniformity on the criteria for defining punctal dimensions based on AS-OCT. The aim of this study is to know imaging characteristics of proximal lacrimal system using SD-ASOCT in normal asymptomatic eastern Indian population.
Methods and materials:
This is a prospective observational cross sectional study done on 50 normal control [aged 20 to 40 years] with no symptoms of epiphora [ MUNK score 0] done in Disha Eye Hospital Barrackpore,India . Written consent from each subject and Hospital Ethics Committee approval was taken . After taking detailed history of long term use of eye drops, previous lid surgery and trauma . All subjects underwent slit lamp examination by an oculoplasty consultant. Ocular surface examination ,tear film break-up time(TBUT),corneal ,staining, lid examination for lid laxity, margin dysfunction ,scarring ,lower lid punctal size shape and position in relation to globe noted.
Exclusion criteria for the study are previous lacrimal or lid surgery,long term antiglaucoma medication use ,lid laxity ,entopion or ectropion, lid mass near puncta ,positive regurgitation of fluid On Pressure over the lacrimal Sac (ROPLAS) and clinically evident stenosed puncta . Slit lamp photography of both lids lower punta with 10x magnification done and punctal grading done by masked evaluator [ ophthalmologist] using clinical grading system proposed by Kashkouli et al [4] .
After the clinical examination single trained technician performed Spectral domain anterior segment OCT [SD-ASOCT] of lower punctum of all subjects [n=100] by using RTVue model-RT100 CAM system [Optovue Inc., Fremont CA, USA] with cornea-anterior module(CAMS) short lens. By gentle pressure by a ear bud the puncta are everted so that the vertical canaliculi placed into the axial plane.
A cross-scan done centred on the lower puntca after proper alignment. External gooseneck LED illumination used to improve the quality of scan. Three scan of each puncta done and the technician choose the clearest and widest diameter picture for measurement by using the adjustable distance measurement tool. For all the studied subjects, punctal shape ,diameter and contents were evaluated.
ASOCT images of punctum [axial scan] displayed a as a conical or funnel shaped gap of tissue from the surface of eyelid. (FIGURE 1) .The external punctal diameters [EPD] were measured as a distance between highest points on the medial and temporal punctal walls of the puncta determined by drawing a tangent line across lower puncta. Internal punctal diameter[IPD] is measured as horizontal line drawn just above junction between puncta and vertical canaliculi .Punctal depth [PD] is height from the EPD tangent line towards the bottom of punctum determined by the point of sudden narrowing of the lumen or the morphological thinning of the lining epithelium. Maximum vertical canaliculi height [MVCH] is the distance from EPD tangent to lowest point of visible canaliculi by ASOCT. Vertical canaliculi height [VCH] is obtained by subtracting the punctal depth [PD] from maximum vertical canaliculi height [MVCH]. Presence of hyper reflective debris and tear layer within puncta also noted.
All data collected and statistical analysis done using Minitab 15 software [Minitab Inc.USA] for windows. Descriptive statistics were calculated and numerical data analysis result expressed mean±SD . p value ≤0.05 considered as significant. Categorical data summarized as percentage. Paired-t test used to compare between gender and right-left eyes punctal measurements data. Agreement between clinical grading of puncta using slitlamp photography and AS-OCT measurements of external punctal diameter [EPD] done by Pearson correlation coefficient and Scatter-plot matrix. Correlation of other measurements like inner punctal diameter, punctal depth also done using same statistics.
RESULTS :
This is a study of both side puncta of 50 volunteers consists of 27 males and 23 females ( n=100) with mean age of 29.2years±SD 5.18. On AS-OCT the mean external punctal diameter(EPD) is 432.02µM± SD 128.77 and mean internal punctal diameter (IPD) is 133.22 µM± SD 33.13 . There was no significant gender and laterality difference (p>0.05) on EPD and IPD. The mean punctal depth [PD] is 333.72 µM± SD 48.04 . there are statistically significant difference in punctal depth(PD) between Male and female puncta [P value is 0.0021] .
There was no significant correlation between EPD and IPD [ r= 0.012 ] ,EPD and PD[r=0.214] and IPD and PD [r=0.034] .
Mean vertical canaliculi height [VCH] are 919.02 ± SD 196.23 [maximum 1467.0 µM, minimum 610.00 µM] which are far less than textbook reading of 2000 µM ( TABLE 1)
AS-OCT provides in vivo ‘optical biopsy’ of lacrimal punctal region revealing three tissue layers as described by various authors by histological studies [Kakizaki et al. 2012] . The first layer is the epithelium which extends from the eyelid surface downwards into the punctum . The epithelium lining the temporal wall thinned early at the entrance to the punctum, whereas the nasal epithelium maintained its thickness into whole wall down upto vertical canaliculus junction. The second thick layer is hyper-reflective compared to the epithelium and it becomes thinner more laterally near the punctal annulus. This layer corresponds to deep fibrous tissue .The deepest layer which depicts Orbicularis [Muscle of Riolan] is hyporeflective as compared to epithelium. (FIGURE 1)
Allam RS et al have described seven morphological variant according to angle of inclination of temporal and nasal wall, vertical punctal depth and proportion of EDP and IPD [8].. In our study sample most common type are funnel [35%] ,deep tubular [21%] and bicornuate [19%] (TABLE 2). Ampulla which are described as a significant dilation of the vertical canaliculus, was visible in only 12 puncta [12%] .
To determine clinical utility of the technique we have studied the agreement between clinical grading of puncta by masked observer and tested the agreement between clinical grade with EPD by Pearson correlation . we found strong agreement [ r=0.6892. 95% confidence level ] between clinical grading and EPD measurement by AS-OCT. [ FIGURE 2]
DISCUSSION :
Anterior segment OCT (AS-OCT) is a imaging modality that uses infrared light of 840nm wavelength to provide structural images of the anterior segment of eye. Wawrzynski et al. first published the result of AS-OCT scan of lacrimal puncta [6] which effectively produce axial image of lacrimal puncta and proximal vertical canalicuar system. In this study we revealed wide range of punctal morphology and measured different dimension of puncta and proximal vertical canaliculi of normal asymptomatic subjects.
In clinical practice punctal assessment is done by slit lamp examination which are prone to wide subjective variability and lacks accuracy. In our study one masked evaluator[ ophthalmologist] assessed Slitlamp photography of all punta [n=100] by using the grading system proposed by Kashkouli et al [4]. Agreement between this clinical grading and ASOCT derived punctal dimension assessed to study the clinical application of punctal ASOCT in actual practice .Pearson correlation of clinical grade of puncta and external punctal diameter[EPD] showed strong correlation between those two[ r=0.6892. 95% confidence ] i.e the ASOct can be a useful tool for ready diagnosis of various pathology like punctal stenosis . But internal punctam diameter[r=0.198],vertical punctal depth [r=0.02] and vertical canaliculi height [VCH] (r=0.120) showed weak correlation with clinical punctal grading. [FIGURE 2] So only examining external puncta by slit lamp one can not be sure about internal punctal or proximal canaliculi stenosis .In this regard punctal ASOCT is a useful tool to assess puncta and proximal lacrimal system.
In our study the mean external punctal diameter[EPD] of the in vivo punctal opening is 432.02 ±SD 128.77µ ASOCT which are larger than the values derived by cadaveric studies [200 to 300 µM ] (Milder & Weil 1983; Cohen et al. 2006)[9,10] . these difference probably attributed by tissue shrinkage in cadaver. Our mean EPD [432.02 ±SD 128.77µ] matches with ASOCT study done by Allam et al [8] but more than the first study done by Wawrzynski et al [6] (247±SD 48µM and Kamal et al (215 µM) [11]and less than Timlin et al. 646 µM[12]. The difference can be justified by difference in measuring points , technique and different ethnic study population.
Mean vertical canlaliculi height [VCH] in our study subjects is are 919.02 ± SD 196.23 [maximum 1467.0 µM, minimum 610.00 µM] which are much lesser than the height [2000µM] mentioned in textbook . The same finding also documented by prior AS-OCT scanning of lacrimal punctal by various groups.[6,8,11,12]. Kamal et al justified these finding may be due Orbicularis muscle tone in vivo study or dynamicity of lid may alter the value.
The limitation of the technique of AS-OCT puncta are steep learning curve because the technique to evert the lid shoud be in a plane so that the vertical canaliculi will be at same axis with the OCT beam. This technique can not scan closed lid and upper lid puncta . It is also not able to scan in blinking or moving lid .
AS-OCT is a useful tool for imaging the lacrimal puncta and proximal vertical canaliculi . AS-OCT puncta may also help to provide new insights into lacrimal pump mechanism [12] .This is also helpful to diagnose and proper treatment planning in punctal stenosis with or without proximal canaliculi stenosis. It can provide image of abnormal puncta like punvctal agenesis or supernumerary puncta. Anterior segment OCT can measure punctal dimensions accurately and it will be helpful to monitor effect of proximal lacrimal system by long term topical medication ,punctal surgery or intubation and to design punctal plug device .
CONCLUSION:
ASOCT of puncta opens a new avenue for understanding of anatomy and physiology of proximal lacrimal system. It can diagnose and monitor puntal pathology of epiphora with ease and good documentation . Different morphological shapes of puncta will be of value to design puntal plug device.
Reference:
- Nemet AY. The etiology of epiphora: a multifactorial issue. Semin Ophthalmol. 2016;31(3):275–279
- Viso E, Rodríguez-Ares MT, Gude F. Prevalence and associations of external punctal stenosis in a general population in Spain. Cornea 2012; 31:1240–1245
- Carter KD, Nelson CC, Martonyi CL. Size variation of the lacrimal punctum in adults. Ophthal Plast Reconstr Surg 1988; 4(4):231–233
- Kashkouli MB, Nilforushan N, Nojomi N & Rezaee R (2008): External lacrimal punctum grading:reliability and interobserver variation. Eur J Ophthalmol,18: 507–511
- Carter KD, Nelson CC, Martonyi CL. Size variation of the lacrimal punctum in adults. Ophthal Plast Reconstr Surg 1988; 4:231–233
- Wawrzynski JR, Smith J, Sharma A, et al. Optical coherence tomography imaging of the proximal lacrimal system. Orbit 2014;33:428–32
- Kakizaki H, Takahashi Y, Iwaki M et al. (2012): Punctal and canalicular anatomy: implications for canalicular occlusion in severe dry eye. Am J Ophthalmol, 153: 229–237 e1.
- Allam RS & Ahmed RA (2015): Evaluation of the Lower Punctum Parameters and Morphology Using Spectral Domain Anterior Segment Optical Coherence Tomography. J Ophthalmol 2015: 591845.
- Milder B & Weil BA (1983): The Lacrimal system, Norwalk, CT: Appleton-Century-Crofts
- Cohen AJ, Brazzo BG & Mercandetti M (2006): The lacrimal system: diagnosis, management, and surgery. New York: Springer.
- Kamal S, Ali MJ, Ali MH & Naik M (2015): Fourier domain optical coherence tomography with 3D and en face imaging of the Punctum and Vertical Canaliculus: a step toward establishing a normative database. Ophthal Plast Reconstr Surg 32, No. 3, 2016
- Timlin HM, Keane PA, Day AC, et al. Characterizing the lacrimal punctal region using anterior segment optical coherence tomography. Acta Ophthalmol. 2016;94(2):154-159.
TABLE 1: Summary Of Punctal AS-OCT Measurements :
| Parameters | Value |
| Total number of subject/Eyes | 50[n=100] Male: Female :: 27:23 |
| Age [years ] | Mean : 29.20 ± SD 5.181
Min : 22.0 Max:42
|
| External Punctal Diameter [EPD] µM | Mean : 432.2 ± SD 128.8
Min : 164.0 Max: 756.0
|
| Internal Punctal Diameter [IPD] µM | Mean : 133.16 ± SD 32.63
Min : 67.00 Max: 247.00
|
| Punctal Depth [PD] µM | Mean 332.90 ± SD 47.91
Min : 192.00 Max: 434.00
|
| Vertical canaliculi height [VCH] | Mean 332.90 ± SD 47.91
Min : 192.00 Max: 434.00
|
| Ampulla present | 12 out of 100 puncta [12%] |
| Tear found within punctum | 78 out of 100 puncta [78%] |
| Hyper reflective debris | 20 out 0f 100 [20%] |
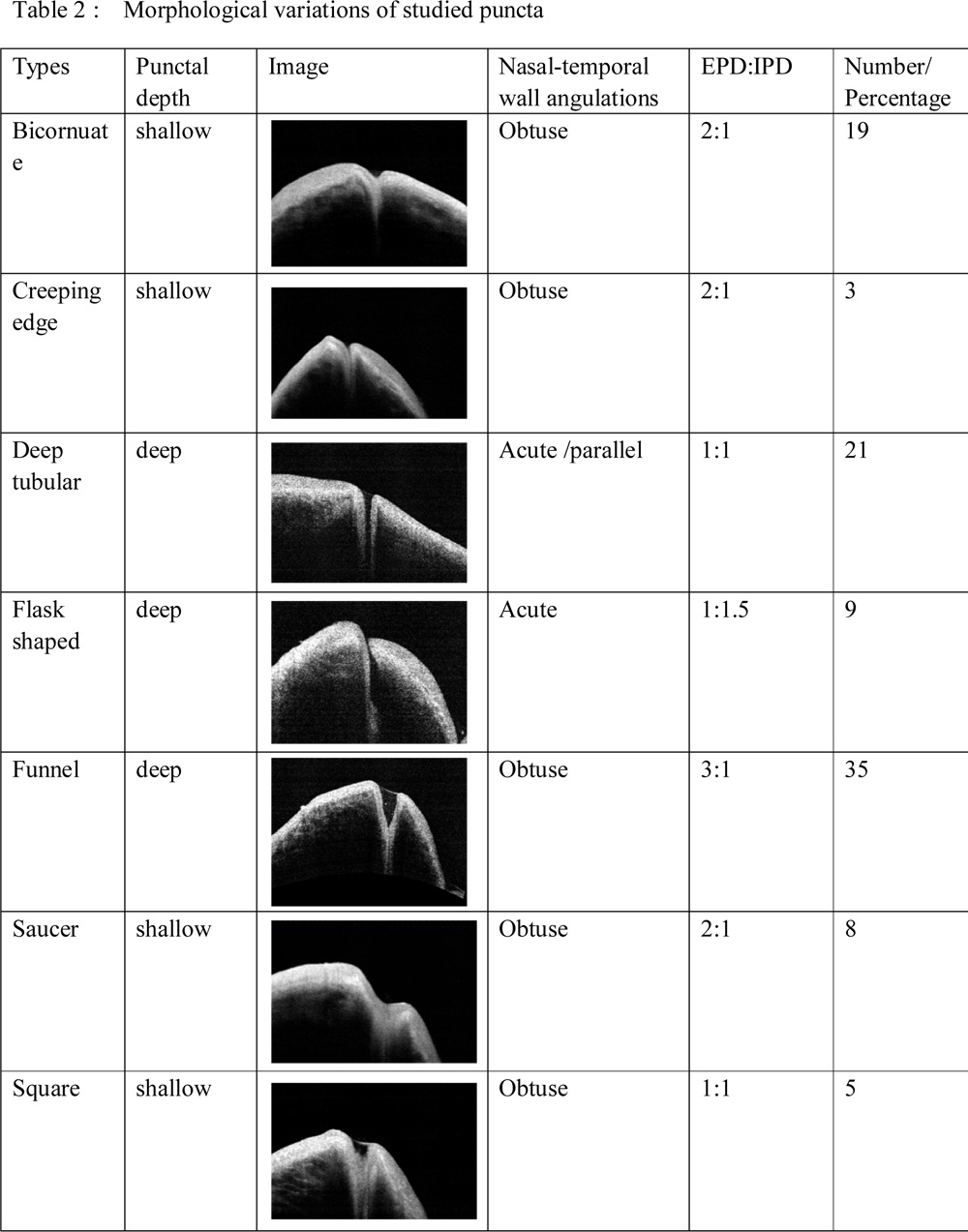
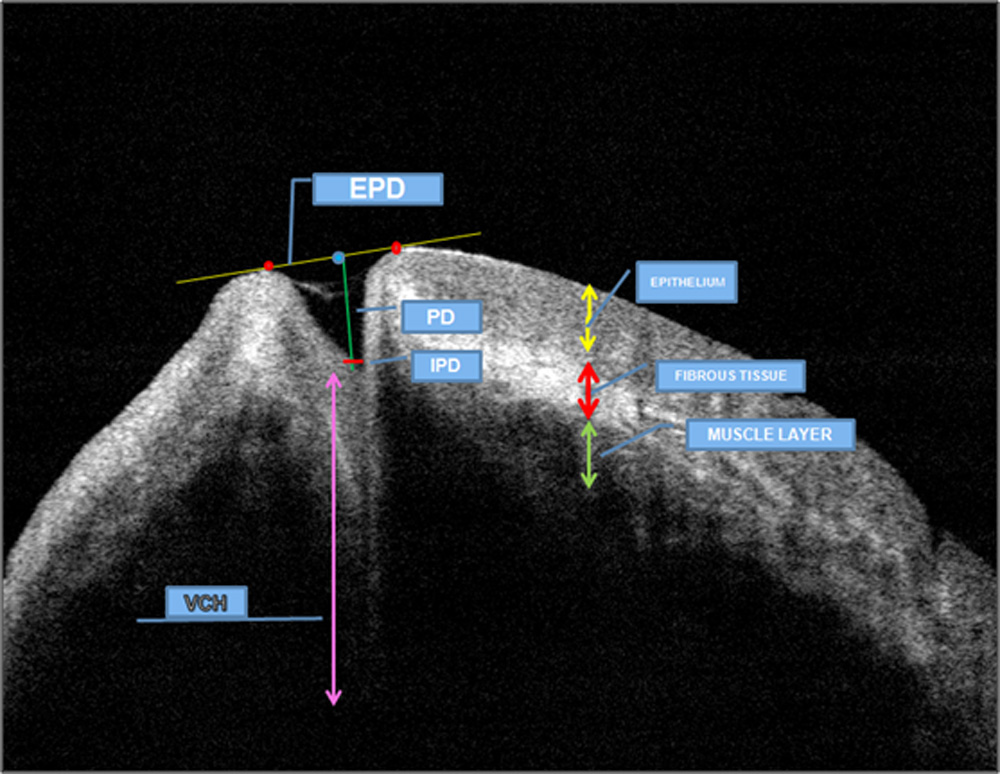
FIGURE 1: Cross-sectional view and measurements of normal punctum and vertical canaliculus , EPD -external punctal diameter distance between highest points on the medial and temporal punctal walls crossing by tangent line across puncta , IPD horizontal line drawn just above junction between puncta and vertical canaliculi, Punctal depth [PD] is height from the EPD tangent line towards the bottom of punctum.,VCH is the vertical canalicular height
FIGURE 2:
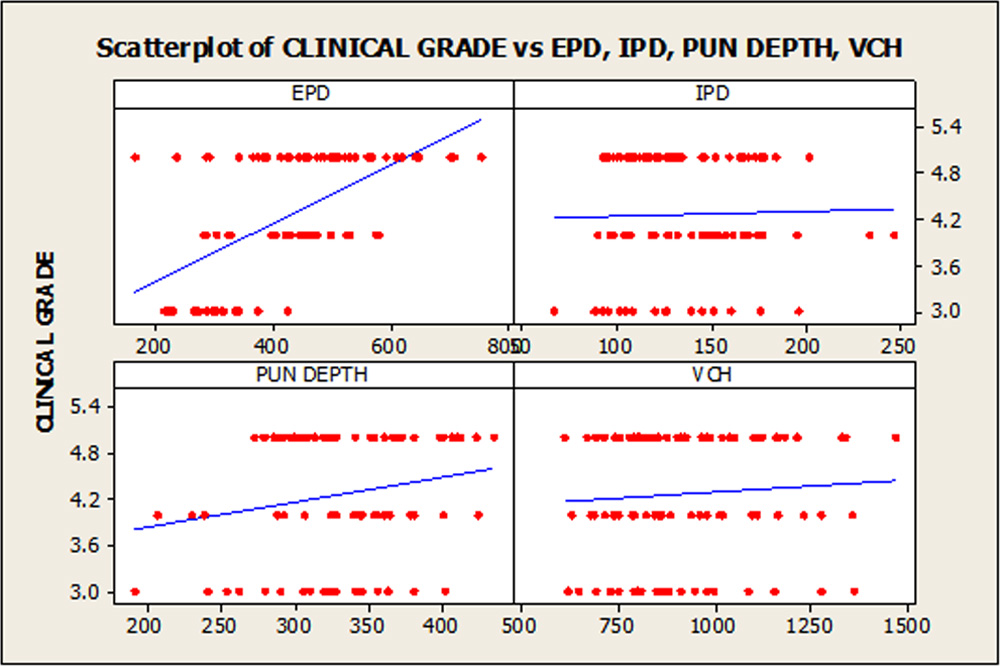
Figure 2 : Scatter Plot matrices of External punctal diameter(EPD) with clinical grading showing strong agreement between two. Agreement between internal punctal diameter(IPD) Punctal depth (PD) and Vertical canalicular height (VCH ) with clinical grading show weak correlation
Leave a Comment