
Dr. Manjunath Natarajan, N18243, Dr. Supriya Bhagat, Dr. Sri Ganesh, Dr. Sheetal Brar
ABSTRACT
Purpose: To investigate the safety, efficacy and biomechanical changes after ReLex SMILE Xtra for corneas which are borderline for refractive surgery.
Materials and Methods:
In this retrospective study two groups of 21 eyes of patients who underwent ReLex SMILE and 21 eyes of patients who underwent SMILE Xtra respectively were selected such that the two patient groups had comparable refractive error (spherical equivalent), central corneal thickness (CCT) and age(in years).
Amongst these two matched groups, the changes in the corneal deformation parameters, including deformation amplitude (DA), applanation time(AT1 and AT2), applanation length(AL1 and AL2), corneal velocity(CV1 and CV2), peak distance (P.D), radius (RAD) and central corneal thickness (CCT) were measured preoperatively, and 3months post-operatively with the Schiempflug camera based tonometer, CorvisScheimpflug Technology (Corvis ST, OCULUS, Wetzlar, Germany) in both groups of patients who underwent either SMILE or SMILE Xtra.
Results:
SAFETY – All surgical procedures in both groups were uneventful. None the patients had any post-operative complications.
EFFICACY – All patients in both groups had 6/6 or better vision post-operatively, with no complications in either group. There was a significant difference in the SMILE Xtra group between the pre and post-operative B-IOP’s(p = 0.05), there was no similar change in the ReLex SMILE group i.e the pre and postoperative B-IOP’s were the same (p=0.17).
BIOMECHANICAL CHANGES–A significant reduction was observed for corneal velocity-1 (pre=0.137m/s, post=0.125m/s), Applanation length-2(pre=1.48mm, post=1.23mm) and central corneal thickness (pre=508.7µ, post=388.19µ), pachymetry corrected IOP showed increase (pre=17.68mmHg, post=23.33mmHg).
Conclusions: There is a significant increase in the biomechanical strength of the cornea following SMILEXtra as evidence by the B-IOP measurements pre and post operatively. The increase is not related merely to changes in central corneal thickness.
This study suggests that SMILE Xtra indeed helps to increase the biomechanical stability of the cornea and is a boon in borderline cases who are at risk of post-surgery ectasia.
INTRODUCTION
This study is the first of its kind to investigate the safety, efficacy (in terms of unaided visual acuity)and corneal biomechanical effects of SMILE Xtra, ReLex SMILE combined with corneal cross-linking.This procedure’s biomechanical strengths are investigated using a novel index called B-IOP measured usingscheimpflug camera based tonometer, CORVIS ST.
With the booming popularity of refractive surgeries, nowadays, there are a multitude of patients whose topography would put a frown on a refractive surgeons face. These borderline cases, under the care of a cautious surgeon would have been easily written off as a case unsuitable for corneal refractive surgery.
Collagen cross-linking (CXL) has been proved as an effective modality to strengthen and stabilize the cornea in keratoconus and ectasia after corneal refractive surgery [1].The novel application of CXL technique with photo ablative procedures such as LASIK and PRK [2, 3], has improved safety and has better outcomes in subjects that were not suitable for corneal refractive correction due to their corneas being borderline.
A further refinement of this ideology is SMILEXtra which has been suggested as a safe and effective procedure for prophylaxis againstpostoperative ectasia in susceptible patients [4].
ReLEx SMILE is a flapless, all femtosecond laser technique which involves creation of a refractive lenticule with femtosecond laser and its removal from a small incision. This
procedure has significant advantages over LASIK as there are no flap related complications, faster visual recovery, better long-term biomechanical stability, less postoperative dry eye, and fewer induction of aberrations.
Since SMILE is flapless and a more tissue saving procedure as it takes similar or less tissue per diopter (~13 ? versus ~17 ? for LASIK) and the cap thickness contributes to the residual bed thickness, it allows higher corrections to be safely achieved. Hence, it may not be unreasonable to say that even patients, ineligible for LASIK Xtra, may safely qualify to undergo corneal refractive correction with SMILE Xtra without increasing the risk of corneal destabilization. Due to this advantage, corrections using this technique may be safely attempted in early keratoconus with judicious patient selection. We observed the refractive and topographic stability of the procedure to be excellent and well maintained at one year[4].
ReLEx SMILE, when combined with collagen cross-linking intraoperatively, may further prevent the risk of future ectasia in susceptible individuals[1].
The efficacy of the procedure, in particular regarding corneal biomechanics has not been studied till date. Hence this study has been taken up.
The corneal biomechanical stability has been investigated using a Schiempflug camera based tonometer, CORVIS ST. The novel parameter used here to study the biomechanics is the Biomechanically corrected intraocular pressure (B-IOP), along with other variable such as deformation amplitude (DA), applanation time(AT1 and AT2), applanation length(AL1 and AL2), corneal velocity(CV1 and CV2), peak distance (P.D), radius (RAD) and central corneal thickness (CCT).
Materials and Methods
The study was approved by Institutional Ethics Committee and adhered to the tenets of declaration of Helsinki. The nature of the procedure was explained and informed consent was obtained from all the patients participating in the study.
Inclusion criteria–
The decision to advise SMILE Xtra to patients was taken considering the assumed risk factors for ectasia based on published literature reports [5,6].According to the Randleman Scoring [6]for ectasia risk, eyes were classified into low (score < 2),moderate(score = 3), and high risk (score = 4). Eyes with moderate and high riskwere selected for treatment; however, eyes with low risk, but associated with other risk factors as per published literature reports, were also included in the study [5].
Subjects with corneal thickness <450 um, established keratoconus, hyperopic refractive error, mixed astigmatism, concurrent eye infection, history of riboflavin allergy, pasthistory of herpes infection or chemical injury, long-term topical or oral steroid use, and pregnant or nursing females were not advised SMILE Xtra procedure.
Patients with whose topography did not have any risk factors for ectasia and whose cornea was healthy and corneal thickness was suitable for refractive surgery were selected to undergo ReLeX SMILE.
Exclusion criteria – Patients who were non-consenting, unwilling to come for follow-up, who were non consenting/ unable to undergo evaluation on CORVIS ST.
Pre-surgery evaluation – All patients underwent a thorough preoperative clinical examination including slit lamp biomicroscopy, dilated fundus examination, manifest and cycloplegic refraction,uncorrected (UDVA) and best corrected (CDVA) distant visual acuity using Snellen charts at 6 m, noncontact tonometry, topography (OrbscanIIz, Baush& Lomb), aberrometry(I Trace, Hoya), specular microscopy for endothelial cell count (ECD; Tomey EM-3000, Japan), contrast sensitivity (FACT), and dry eye assessment (Schirmer 1) and in addition also underwent OCULUS PENTACAM (Pentacam HR, Typ70900, Oculus Optikgeräte GmbH,Wetzlar, Germany)and CORVIS ST (CST, Oculus Optikgeräte GmbH, Wetzlar, Germany)evaluation.
Patients were examined on post-operative day 1, 1 month, 3 months, 6 months, and 12 months postoperatively. Recordings of UDVA and slit lamp examination was done on all visits.
On subsequent visits after day one, CDVA, topography, aberrometry, AS-OCT (Optovue), specular counts, contrast sensitivity, and dry eye assessment were also performed.
Surgical Technique-
All patients underwent bilateral procedures by the same experienced surgeon (SG) on the same day. In the first stage, ReLEx SMILE was performed usingstandard surgical techniques. Visumax femtosecond laser (Carl Zeiss Meditec, Jena) was used to create a refractive lenticule with optical zone ranging from 6 to 6.5 mm, capdiameter 7–7.5 mm, and thickness of 100 ?m. The lenticule was then dissected and extracted through a 2 mm superior incision. Immediately after removal of the lenticule, 0.1 mL of VibexXtra, (Avedro, Waltham, MA) which is 0.25% riboflavin in saline was injected into the interface and allowed to diffuse for 60 seconds followed by washing of the interface with saline. Intraoperative slit lamp examination was done to ensure saturation of the cornea and the diffusion of dye into the anterior chamber. Using the Avedro KXL system (Waltham, MA), accelerated cross-linking with UV-A radiation was performed at 365?m wavelength, with energy of 45 mW/cm2 delivered in continuous mode to facilitate cross-linking through the cap for 75 seconds. Total energy deliveredwas 3.4 J/cm2.
There were no intraoperative complications.Postoperative medications included topical 0.3%Ofloxacin (Exocin, Allergan) 4 times for 3 days, 0.1%prednisolone acetate eye drops (Predforte, Allergen) intapering dosages for 4 weeks, and lubricants 4–6 times for 4weeks or more
CORVIS ST
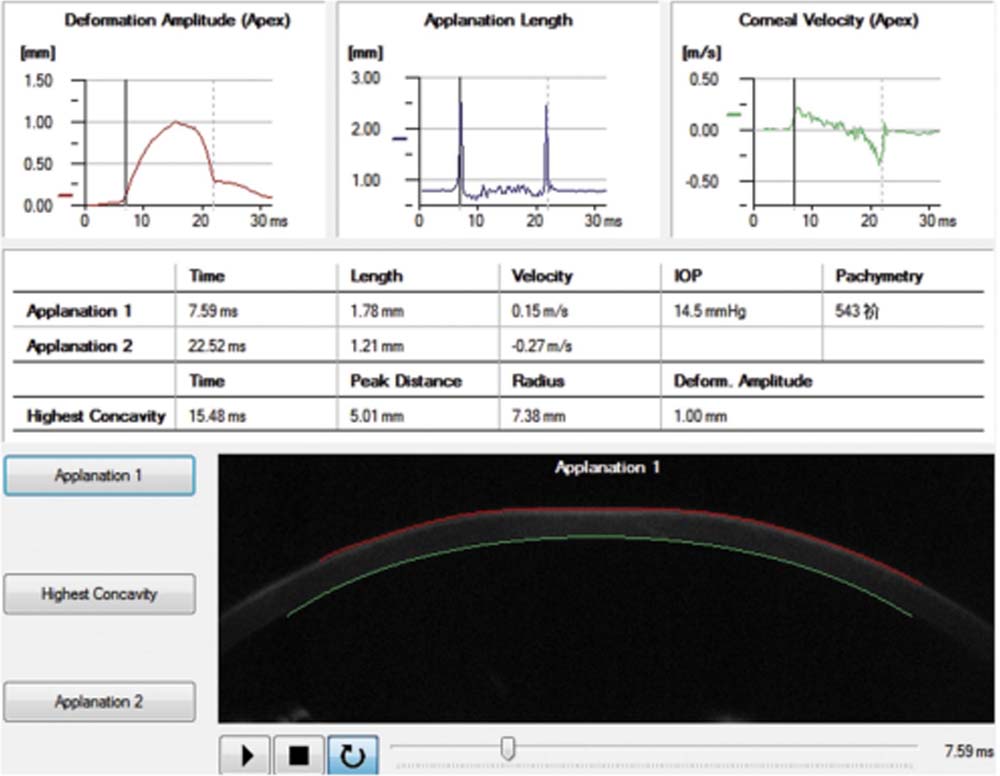
Figure 1. The real-time corneal deformation parameters of a participant recorded when the cornea was just flattened.
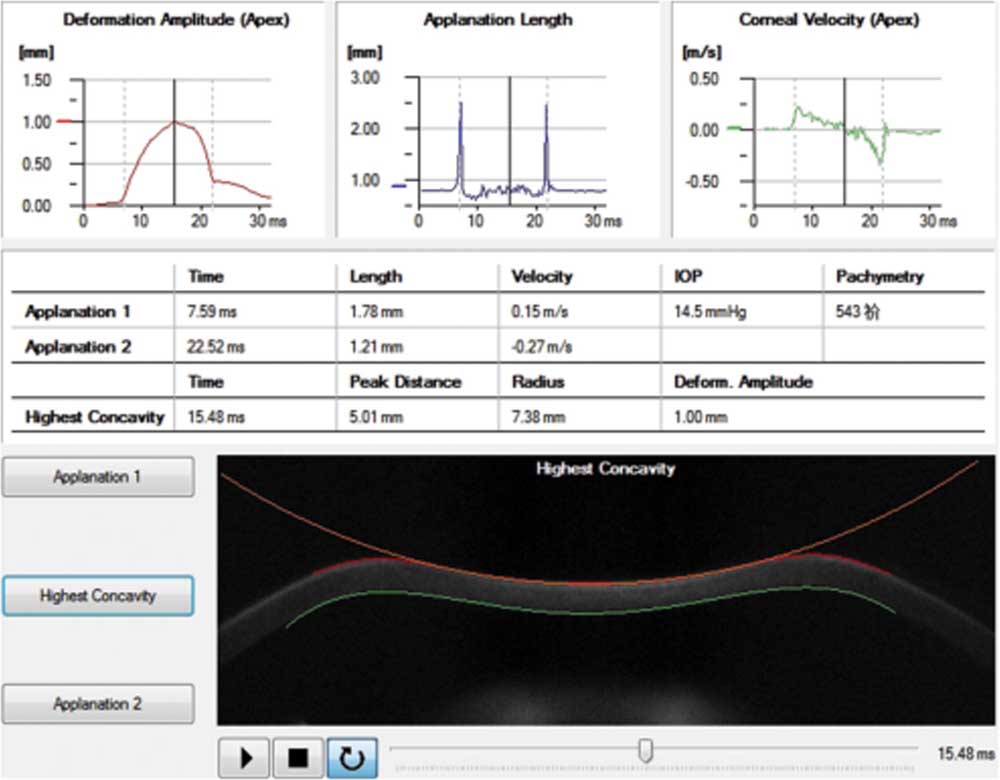
Figure 2. The real-time corneal deformation parameters of a participant recorded when the cornea was flattened to the highest
concavity.
Corneal deformation parameters were acquired with the Corvis ST preoperatively and at post-operative visits. The patient was asked to fixate on target (a red light) in the CORVIS ST with his or her chin on a chin-rest and forehead against the forehead strap. A monitor on the tonometer would guide the operator aim the nozzle at the center of the patient’s cornea with a joystick attached to the tonometer and it puffed an air jet onto the center of the cornea automatically. Then the process of corneal deformation caused by the air puff was recorded. Meanwhile, the Corvis ST automatically calculated the applanation time, applanation length and corneal velocity while the cornea was flattened for the first time (applanation 1) (Figure 1), depressed to the highest concavity(Figure 2) and applanated for the second time during the recovery from the air puff (applanation 2) (Figure 3). The corneal deformation amplitude (DA), peak distance (P.Dist.), radius, central corneal thickness (CCT) and intraocular pressure (IOP) values were also calculated and recorded.
The B-IOP is recorded automatically by the CORVIS ST, this parameter is an index of the biomechanical strength of the cornea, it is the intraocular pressure of the eye after correcting for biomechanical changes.The Corvis ST allows a measurement in vivo of the cornealdeformation properties referred to as DA, AT1 and AT2 inaddition to IOP, which appear to be indicators of the overallbiomechanical properties of the cornea. Hon Y reported that DA,AT1, AT2 and IOP values were well repeatable while corneal velocities, applanation lengths and time at the highest concavitywere not. [7–8] So far, Corvis ST has not clinically used in the field of refractive surgeries.
Fig 3. Parameters measured in the CORVIS ST.
RESULTS
SAFETY – All surgical procedures in both groups were uneventful. None the patients had any post-operative complications.
EFFICACY – All patients in both groups had 6/6 or better vision post-operatively, with no complications in either group. Themean spherical equivalent reduced from -4.36 ± 1.79 to -0.166±0.58D.The mean uncorrected distant visual acuity post-op was -0.01 LogMAR was comparable with mean pre-op distance corrected visual acuity of 0.06 LogMAR (p=0.11).No eye developed haze or progressed to ectasia.
BIOMECHANICAL CHANGES–A significant reduction was observed for corneal velocity-1 (pre=0.137m/s, post=0.125m/s), Applanation length-2(pre=1.48mm, post=1.23mm) and central corneal thickness (pre=508.7µ, post=388.19µ), pachymetry corrected IOP showed increase (pre=17.68mmHg, post=23.33mmHg).
A significant difference was detected among both the groups (pre-operative vs post-operative) for applanation 2 velocity, PD, DA.
DISCUSSION
In our study the results show that SMILE Xtra procedure (ReLex SMILE with collagen cross linking) is a safe, efficacious procedure.
We also found that SMILE Xtra procedure does cause an increase in the biomechanical stability of the cornea, evidenced by the B-IOP found by CORVIS ST. This information is important as there are many who question the results of refractive procedures combined with collagen cross linking, including SMILE Xtra.
Photorefractive keratectomy (PRK) and laser in situ keratomileusis (LASIK) have been recognized as weakening the corneal structural integrity by 14% to 33% and may increase the risk of ectasia [7-9].
For prophylactic purposes virtually any corneal excimer laser patient can be treated with cross-linking, although certain susceptible patients may benefit more [3].
SMILE Xtra, which involves simultaneous high fluence cross-linking of cornea following ReLEx SMILE. For myopia, in individuals who may be at risk of future corneal ectasia. The concept is similar to the study by Kanellopoulos who did CXL in a femtosecond laser created corneal pocket in early keratoconus, suggesting a safe and effective alternative to conventional collagen cross-linking with advantages of no deepithelisation, faster healing, and reduced chances of infections and better patient comfort [10].
Although the efficacy of the classical Dresden protocol as well as accelerated cross-linking is established in longterm follow-up studies in keratoconus [4], the prophylactic dose required in non keratoconus individuals who may be at risk of ectasia is not yet established. Review of the literature reveals that there is no standard protocol addressing such patients at risk, and different authors have suggested different regimens. When combined with LASIK, researchers have used high fluence of 30mW/cm2for variable durations, delivering energy ranging from 1.8 to 5.4 J/cm, and found all regimens to be safe and effective [4]. In our study, all SMILE Xtra procedures were done using the Avedro KXL device, we took avdageofthehighestfluenceat45mW/cm2 and accelerated cross-linking for 75 seconds, thus delivering a surfacedose of 3.4 J/cm2at the corneal plane.
We used Vibe XXtra (0.25% in saline) which is recommended for intrastromal application as it rapidly achieves high concentrations in the stroma. Since it is devoid of dextran, the diffusion into deeper layers is achieved as early as 60 seconds after application. This helps in selective placement of riboflavin in the stroma so that it absorbs and activates UVA light and achieves cross-linking without posing a threat to the underlying vital structures due to any stray radiation.
It is interesting that DA, AT1, AT2 and IOP did not change significantly after lenticule creation during SMILE procedure, butthe value of Peak 1 do change after cutting a flap during FSLASIK in earlier studies[12]. This indicated that SMILE mayoutplay FS-LASIK at operative safety and maintaining cornealbiomechanical stability. A possible explanation is that flap iscreated by cutting through the corneal epithelium and Bowman’slayer. This process breaks all the corneal collagen fibers between the flap and the stromal bed. However, SMILE procedure does not create a complete LASIK flap, and the process of lenticule creation does not cut Bowman’s layer, and thus maintains the structural integrity of the cornea.
The present study had some limitations. The relativelysmall sample size made it difficult to completely avoid a possible selection bias. The data was analysed at 3months post operative only not throughout the follow up period (to avoid confounding factors).
In conclusion, there is a significant change in corneal deformation parameters following SMILEXTra procedure which indicates that it indeed strengthens the cornea and it can be done in people whose corneas are borderline for refractive surgery.
REFERENCES.
- Wollensak, E. Spoerl, and T. Seiler, “Riboflavin/ultraviolet-Ainduced collagen crosslinking for the treatment of keratoconus,” American Journal of Ophthalmology,vol.135,no.5,pp.620–627, 2003.
- J. Kanellopoulos and P. S. Binder, “Collagen cross-linking (CCL) with sequential topography-guided PRK: a temporizing alternative for keratoconus to penetrating keratoplasty,” Cornea,vol.26,no.7,pp.891–895,2007.
- J. Kanellopoulos and G. J. Pamel, “Review of currentindications for combined very high fluence collagen crosslinkingand laser in situ keratomileusis surgery,” Indian Journalof Ophthalmology,vol.61,no.8,pp.430–432,2013.
- Sri Ganesh and SheetalBrar, Clinical Outcomes of Small Incision Lenticule Extraction withAccelerated Cross-Linking (ReLEx SMILE Xtra) in Patients withThin Corneas and Borderline Topography, Hindawi Publishing Corporation Journal of Ophthalmology Volume 2015, Article ID 263412, 2015
- P. S. Binder and W. B. Trattler, “Evaluation of a risk factor scoring system for corneal ectasia after LASIK in eyes with normal topography,” Journal of Refractive Surgery,vol.26, no.4, pp. 241–250, 2010.
- B. Randleman, M. Woodward, M. J. Lynn, and R. D. Stulting,“Risk assessment for ectasia after corneal refractive surgery,”Ophthalmology, vol. 115, no. 1, pp. 37.e4–50.e4, 2008.
- E.K.Cartwright,J.R.Tyrer,P.Jaycock,andJ.Marshall,“The effects of variation in depth and side cut angulation in subBowman’skeratomileusis and LASIK using a femtosecondlaser: a biomechanical study,” Journal of Refractive Surgery,vol.28,no. 6, pp. 419–425, 2012.
- C.Chen,N.Lee,N.Bourla,andD.R.Hamilton,“Corneal biomechanical measurements before and after laser in situ keratomileusis,” Journal of Cataract and Refractive Surgery ,vol. 34,no.11,pp.1886 1891,2008.
- Shah and M. Laiquzzaman, “Comparison of corneal biomechanics in pre and post-refractive surgery and keratoconic eyes by Ocular Response Analyser,” Contact Lens &Anterior Eye,vol. 32,no.3,pp.129–132,2009
- J. Kanellopoulos, “Collagen cross-linking in early keratoconus with riboflavin in a femtosecond laser-created pocket:initial clinical results,” Journal of Refractive Surgery,vol.25,no.11,pp.1034–1037,2009.
- Charters, “Combined SMILE, CXL safe for keratoconus,” https://ophthalmologytimes.modernmedicine.com.
- Uzbek AK, Kamburog˘lu G, Mahmoud AM, Roberts CJ (2011) Change in biomechanical parameters after flap creation using the Intralase femtosecond laser andsubsequent excimer laser ablation. Curr Eye Res 36: 614–619
Leave a Comment