
Dr. Supriya Bhagat, B15084, Dr. Manjunath Natarajan, Dr. Sheetal Brar, Dr. Sri Ganesh
Abstract:
Context:
Aims: Purpose: To evaluate the clinical benefits of intense pulsed light (IPL) in chronic dry eye patients due to meibomian gland disease (MGD) , unresponsive to the conventional treatments.
Settings and Design: Prospective, clinical
Methods and Material:
Methods: This is a prospective, non-randomized, non-comparative clinical study whichincluded 18 patients with chronic dry eye disease due to MGD who were unresponsive to the conventional treatments. IPL treatment was administered to the skin area below and lateral to the lower eyelid on 4 consecutive sessions one month apart. The intensity of IPL ranged from 10 Joules/centimetre square (J/cm2) to 12 J/cm2 in accordance with the Fitzpatrick skin type grading and as per manufacturer recommendations. Tear break up time (TBUT), tear meniscus height, corneal staining, meibomian gland assessments and subjective symptom scores (SPEED 2 questionnaire) were recorded at each visit( A brief description of SPEED Questionnaire?). After the IPL treatment meibomian glands were expressed manually at the slit lamp.
Statistical analysis used:
Results: Significant improvements were observed in subjective symptom scores(SPEED 2),TBUT from baseline 4.64+/-2.13 sec to 7.80+/-1.98 sec in the last session(P value <0.05).Meibomian gland secretion quality and expressibility improved at every visit. No adverse effects were noted in any patient.
Conclusions: In our experience IPL therapy appears to be promising and effective treatment in relieving signs and symptoms of dry eye due to MGD.
Key-words: Intense pulsed light, Meibomian gland dysfunction, dry eyes, IPL
Key Messages:
Meibomian gland dysfunction (MGD) is the leading cause of evaporative dry eye disease (DED). It manifests with symptoms of ocular surface burning and irritation, fluctuating visual acuity and red and often watery eyes.1,2 In MGD the meibomian glands become narrowe, the acini atrophy and hyperkeratiniseand the meibum increases in viscosity This reduces meibum outflow, encouraging proliferation of commensal bacteria.
The goal of MGD therapy is to provide long term improvement of symptoms for patients by improving the quality of meibum, increasing meibum flow , improving tear film stability and decreasing inflammation.
Commonly used therapies include preservative free drops (which drops? Lubricants? Please mention) , omega 3 fatty acid5 supplementation, topical cyclosporine2, topical azithromycin, oral doxycycline, warm compresses and others.Despite the variety of treatment options available, patients often do not experience complete or long term relief of symptoms.
Intense-Pulsed-light therapy:-Intense pulsed light (IPL) therapy, which uses light energy to affect the skin surface, is widely used in dermatology to treat a variety of conditions including dermal vascular lesions, such as port wine stains and hemangiomas, facial rosacea, and acne6. In addition, this technology is used in hair removal and treatment of facial skin photodamage signs, such as fine wrinkles and skin laxity. In 2002, Rolando Toyos, MD, discovered the positive ophthalmic effects of IPL on his patients who underwent treatment for facial rosacea7. Along with decreased facial erythema, his patients developed improvement in signs and symptoms of meibomian gland dysfunction (MGD) and dry eyes.
IPL treatment:
IPL is a broad spectrum, non-coherent, and polychromatic light that uses Xenon flashlamp to emit wavelengths of light from 400 to 1200nm; it can be filtered to allow only arange of wavelengths to be emitted8. The pivotal mechanism of IPL involves the principle of selectivephotothermolysis, in which light energy that comes in contact with tissue is preferentially absorbed by achromophore and converted into heat. With respect to the skin, melanin and hemoglobin are the two primary chromophores present. Light energy absorption in melanin decreases as the wavelengthof light increases. Oxyhemoglobin, however, has an absorption peak at 578nm. Yellow light wavelengths are able to pass through the upper layers of the skin without excessive absorption of the light energy by melanin. The absorption of the yellow light by oxyhemoglobin then results in conversion of the light into heat energy, leading to coagulation and ablation of blood vessels9. Eyelid margin telangiectasias are often seen clinically in patients with MGD. IPL allows for selective ablation of these superficial vessels, which not only reduces telangiectasias and erythema but also presumably decreases inflammatory marker access to the meibomian glands. Other potential mechanisms of action of IPL for dry eye treatment include reduction of bacteria and/or parasitic growth on the eyelids. Demodexfolliculorum mites, which are ectoparasites living in hair follicles and sebaceous glands, retain a commensal relationship with the Bacillus oleronius bacterium9,10. Prieto et al. discovered coagulated Demodex organisms and reduced lymphocytic infiltration in patients who had undergone IPL treatment11. Another potential mechanism of IPL includes a temporary local thermal effect that warms the meibomian gland secretions. This warming effect can allow for improved manual expression of inspissated meibum within the meibomian glands after application of the light. With improved meibum secretion and viscosity, the tear film can become more stable and thus evaporative dry eye symptoms would improve.
Subjects and Methods:
A total of 18 participants (10 females and 8 males) with moderate to severe MGD and a mean age of 54 ± 12 years were included in the prospective study.Subjects were recruited between December 2016 and June 2017.
The inclusion criteria for this study were:
(1) Adult patients with moderate to severe MGD who were unresponsive to conventional MGD therapy after one year of treatment (2) willingness to cooperate with the doctors in the follow-up visits.
Exclusion criteria included patients with
(1) history of ocular trauma or surgery; (2) punctal occlusion; (3) active allergy or infection or inflammatory disease of the ocular surface unrelated to dry eye or MGD; (4) pathology of the lacrimal drainage system, (5)use of systemic medications which alter the tear film; (6) contact lens wear; (7) systemic diseases affecting the ocular surface; (8) pigmented lesions in the treatment area; (9) skin treatments within 2 months; (10) pregnant/nursing mothers.
Treatment Procedure.
Patient selection and the IPL treatment protocol followed the established technique of Toyoset al15. In brief, potential IPL candidates underwent Fitzpatrick skin typing12 to classify their skin response to ultraviolet exposure by the degree of burning and tanning . With an Lumenis M22 IPL with OPT (Mention fullform of OPT), IPL treatment was administered to the skin area below and lateral to the lower eyelid . Before treatment, the eyes were protected with eye shields and ultrasound gel was applied on the patient’s face from tragus to tragus including the nose to conduct the light. This helps to spread the energy evenly, and provide a degree of protection . The intensity of the IPL treatment ranged from 10 J/cm2 to 12 J/cm2 in accordance with the Fitzpatrick Skin Type grading and as per manufacturer recommendations. In each IPL treatment, 6 overlapping flashes were applied to the skin area below and lateral to the lower eyelid for every eye withoutany pressure. All the treatment areas were identical within different subjects.Each treatment was followed by Meibomian gland expression with a cotton tip applicator and digital pressure to empty meibum from bilateral upper and lower eyelids. The subjects received four consecutive treatment sessions one month apart. All the treatments were performed by the same doctor.
Clinical Evaluation.
Subjects were evaluated at five visits: one day before the first IPL treatment and at 1st month, 2nd month , 3rd month and 4th month after the first IPL treatment. The clinical assessments of the subject and both eyes were carried out in the following order: best spectacle corrected visual acuity(log MAR), upper and lower tear meniscus height (TMH), tear break-up time (TBUT), fluorescein corneal staining (IT IS NOT CLEAR HOW CORNEAL STAINING WAS MESURED/ QUANTIFIED/ GRADED), and meibomian gland assessment. An interval of5 minutes was kept between different tests.Symptoms were also compared prior to each treatment usingthe Standard Patient Evaluation of Eye Dryness (SPEED 2)validated questionnaire, and each subject summarized their perceived severity of dry eye symptoms before and after treatment for each eye. All the test data were collected by two doctors ; the average would be defined as the final results. All the evaluations and assessments were carried out before the IPL treatment at each visit.
Statistical analysis
Post-IPL scores at 1 month, 2 month , 3 month and 4 month were compared with pre-
IPL scores at baseline (BL). Comparison betweendata points was performed with paired ?-test with the Bonferronicorrection, which compared the single and total symptoms,
TMH, TBUT, corneal staining,and the meibomian gland at the different follow-up times to those of the last visits. Outcomes were considered significant if P <0.05.
Results
The mean patient age was 54 ± 12 years.
TBUT (in seconds) and Corneal Staining.
TBUT (in seconds) at 1 month (5.51 ± 1.8),2nd month (6.84 ± 1.9), 3rd month (7.62 ± 1.4) and 4th month (7.8 ± 1.2 ) were significantly increased compared to that at the baseline (4.64 ± 2.1) (?<0.05) (Figure 1). Between the visits of 1month and 3 month, TBUT increased continuouslyand this difference was statistically significant(?< 0.05).
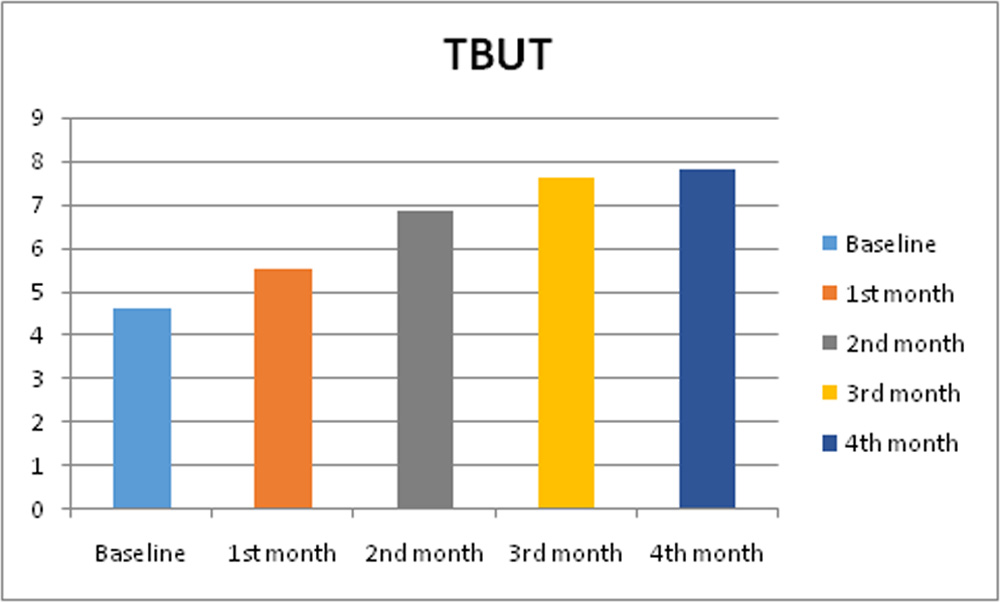
Figure 1: Tear Break Up Time (TBUT)
No significant differencewas found in the assessment of corneal staining among all visits.
| Baseline | 1 month | 2nd month | 3rd month | 4th month | |
| Corneal Staining(HOW IS THE VALUE OBTAINED) | 0.18 ± 0.35 | 0.11 ± 0.19 | 0.08 ± 0.17 | 0.09 ± 0.21 | 0.11 ± 0.25 |
| P value | 0.46 | 0.74 | 0.89 | 0.92 |
Table 1: Corneal Staining changes during IPL treatment
Tear Meniscus Height (TMH)in millimeters (mm)
No significant difference was found in the assessment of upper and lower TMH among all visits (Figure 2).
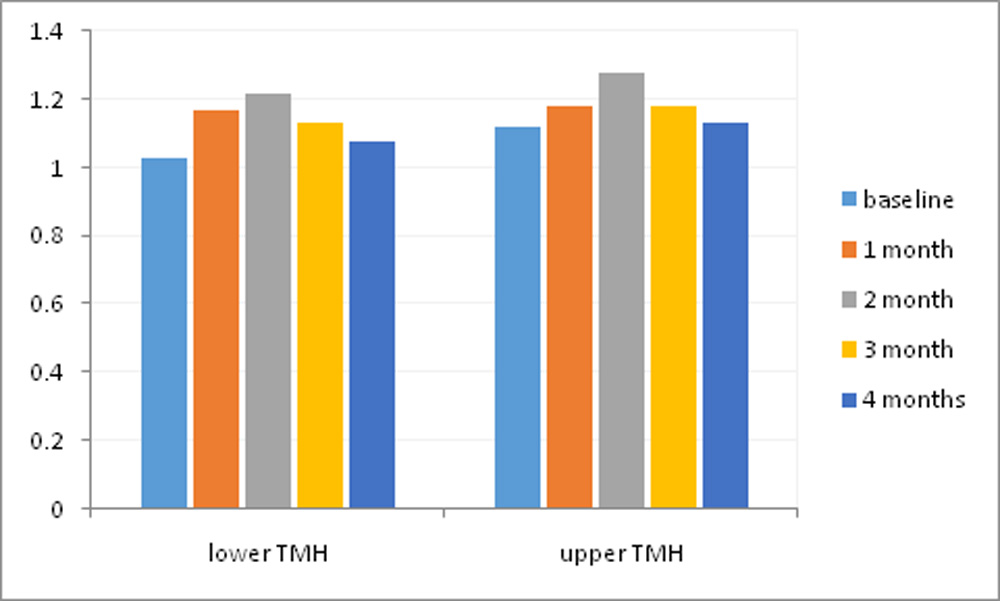
Figure 2: Tear Meniscus Height (TMH) changes in mm
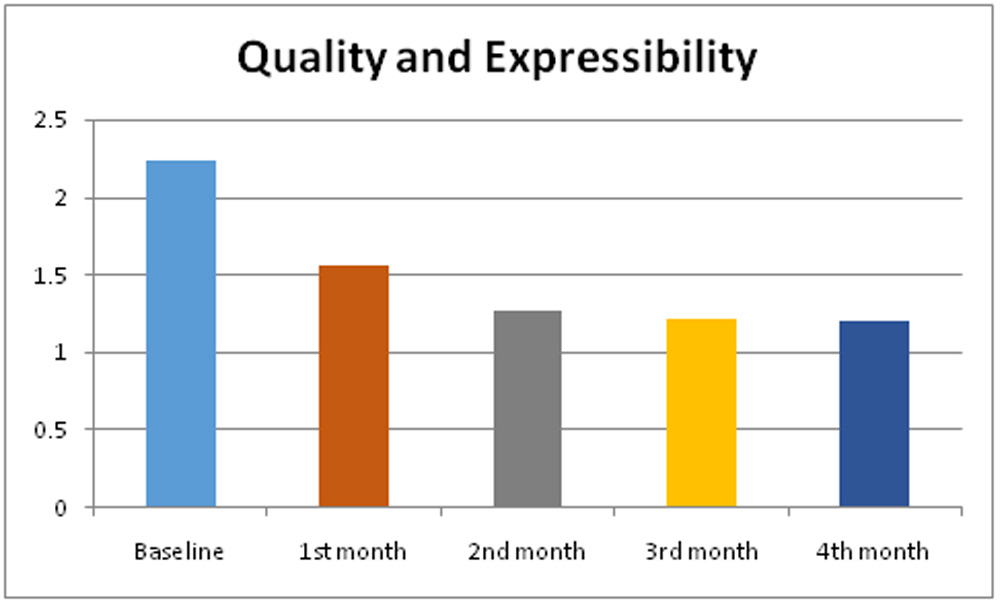
Meibomian gland secretion quality and expressibility
The degree of ease with which meibum could be expressed at the central area of both upper and lower eyelid was evaluated semi-quantitatively on a scale from 0 to 3: 0 = clear meibum readily expressed; 1 = cloudy meibum expressed with mild pressure; 2 = cloudy meibum expressed with more than moderate pressure; 3 = meibum could not be expressed even with strong pressure.Compared to the baseline, the meibomian gland secretion quality and expressibility significantly improved at the follow up visits(?< 0.05).
Higher grade meaning worse quality and expressibility (Figure 3)
SPEED II SCORE:
After a series of IPL/Meibomian Gland Expression(MGX) treatments noted a statistically significant decrease in SPEED 2 scores(paired t test). Patients showed various levels of improvement of their symptoms and rarely worsening of symptoms. After second IPL/MGX treatment, 61% of patients noted improvement in dry eye symptoms.After fourth IPL/MGX treatment, an additional 28 % of patients noted decrease in dry eye symptoms
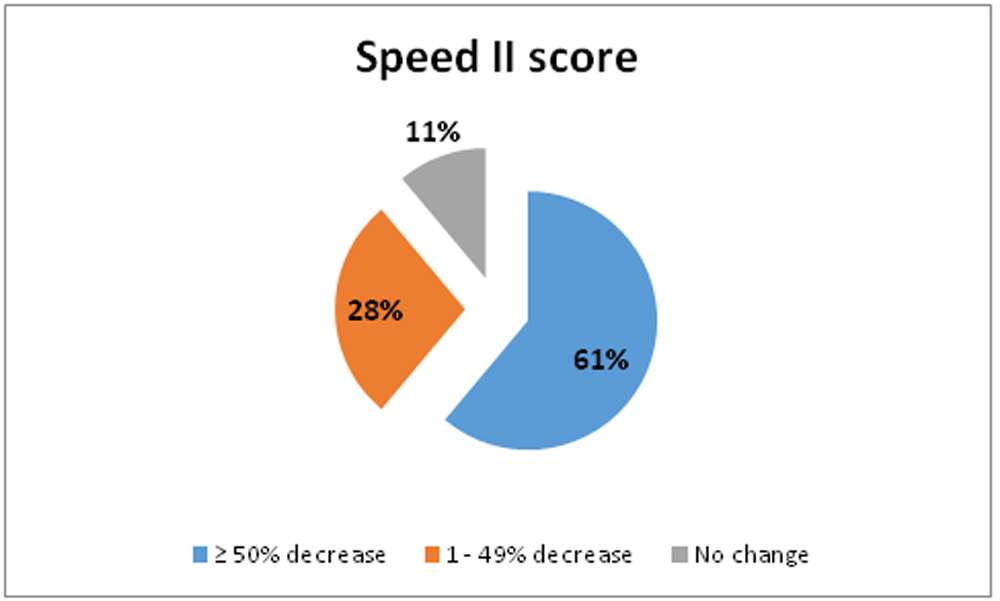
Figure 4: Number of patients in percentages versus change in Speed II score
Safety Data.
At all visits, best spectacle correctedvisual acuity was unchanged.There was no depigmentation,blistering, swelling, redness, and hair loss at the skin area around the eye. There was no significant eyelashloss during the evaluation. No systemic adverse event was observed during the study.
Discussion:
Meibomian gland dysfunction (MGD) is the leading cause of evaporative dry eye disease (DED).The management of MGD in clinical practice remainschallenging. The efficacy of conventional treatment for MGD continues to be transient and unsatisfactory,suggesting the need for the exploration of new therapeuticapproaches. Our study applied IPL treatment combined with meibomian gland expression in 18 MGD patients (36 eyes) and provided a strong evidence for the effectiveness and safety of IPL treatment in relieving ocular surface symptoms and signs.This article is the first report of a prospective study of IPL for MGD in Indian eyes.
The alteration of meibomian gland secretion quality andexpressibility are the key characteristics in MGD eyes. Our research revealed significant improvements of meibomiangland secretion quality and expressibility after IPL treatments.Similar results were observed in Jiang et al14in a prospective study.Studies showed that melting pointof meibomian gland secretions in subjects withMGDwas 3 degree celsiushigher than that in normal eyes and thermal therapies suchas warm compression were able to melt the pathologicallydysfunctional lipids and relieve the ocular surface symptomsassociated with MGD. Theoretically, the light coming fromIPL device is directly exposed to the skin and could resultin a production of heat higher than body temperature,which is enough to melt the thick meibomian secretion. Duringthe IPL treatment, enough ultrasound gel should be used onthe patient’s face from tragus to tragus including the noseto conduct the light, help to spread the energy evenly, andprovide a degree of protection.
Our study also found that TBUT was significantly lengthenedafter IPL treatment. Tear film is a highly organizedstructure on the ocular surface; its stability and functionare highly relied on its biochemical composition. Theimprovement of the meibomian gland secretion quality andexpressibility by IPL treatment may have a direct effect onthe stability of tear film. Craig and colleagues13 found outthat IPL therapy was able to improve the lipid layer gradein tear film.Similar improvement in TBUT was found by Jiang et al14 and Craig et al13.
In our study we also noted decrease in the SPEED 2 scores (indicating improvement in symptoms) possibly due to the effect on the stability of the tear film which might have improved due to the improved meibomian gland secretion quality and expressibility. Similar results were observed by Craig et al13.
Overall, there are some possible mechanisms by whichIPL treatment could relieve ocular surface symptoms andsigns of MGD eyes. First, IPL is able to produce a heat effectwhich melts the pathologically dysfunctional secretions. Second,the IPL device we applied emits energy in a band froma base of the visible spectrum (580nm) to near infrared(1200 nm), which can be absorbed by hemoglobin, causingthe thrombosis of the abnormal telangiectaticvasculature in eyelid marginand related conjunctiva. In addition, the bacterial load on the lid margin and ocular adnexa could be directlyaffected by the IPL. There is a further possibility that IPL hasthe potential to modify the mitochondrial output of reactiveoxidative species (ROS), which have been implicated in dry eyedisease.
CONCLUSIONS
In our experience, IPL therapy appears to be promising and effective treatment in relieving signs and symptoms of evaporative dry eye due to MGD. IPL treatment is a newly advanced choice for MGD patients in Indian eyes.
LIMITATIONS
There are some limitations in our study including thefollowing.
(1) The first is lack of control group. Lack of a non-treatmentcontrol group, the placebo effect and the risk of investigatorbias could have influenced the results. Further studies shouldbe carried out with placebo controls or positive controls torule out the above influences.
2) The short time of observation was limited to1 month after the final fourth treatment. The full effect of the final treatment might not have been realised. A long term follow-up is also needed after treatmenttermination to assess the long-term effectiveness and safety of such treatment.
3) Mechanisms of IPL treatment in MGD eyeswere not proven in our study. Further research should becarried out to explore the exact mechanisms or molecularchanges during IPL therapy in MGD eyes.
References:
- Shimazaki J, Sakala M, Tsubota K. Ocular surface changes and discomfort in patients with meibomian gland dysfunction. Arch Ophthalmol. 1995; 113:1266–1270.
- Geerling G, Tauber J, Baudouin C, et al. The International Workshop on Meibomian Gland Dysfunction: report of thesubcommittee on management and treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2011; 2:2050–2064.
- Obata H. Anatomy and histopathology of human meibomian gland. Cornea. 2002; 21:S70–S74.
- Borchman D, Foulks GN, Yappert MC, Milliner SE. Differences in human meibum lipid composition with meibomian gland
- dysfunction using NMR and principal component analysis. Invest Ophthalmol Vis Sci. 2012; 53:337–347.
- Ole˜nik A, Mahillo-Fern´andez I, Alejandre-Alba N, et al. Benefits of omega-3 fatty acid dietary supplementation on health-relatedquality of life in patients with meibomian gland dysfunction. ClinOphthalmol. 2014;8:831–836.
- Piccolo D, Di Marcantonio D, Crisman G, et al. Unconventional use of intense pulsed light. Biomed Res Int 2014; 2014:618206.
- Kent C. Intense pulsed light: for treating dry eye. Rev Ophthalmol 2010; https://www.reviewofophthalmology.com/content/d/technology_update/i/1353/c/25857/.
- Campolmi P, Bonan P, Cannarozzo G, et al. Intense pulsed light in the treatment of non-aesthetic facial and neck vascular lesions: report of 85 cases. J EurAcadDermatolVenereol 2011; 25:68–73.
- Papageorgiou P, Clayton W, Norwood S, et al. Treatment of rosacea with intense pulsed light: significant improvement and long-lasting results. Br J Dermatol 2008; 159:628–632.
- Li J, O’Reilly N, Sheha H, et al. Correlation between ocular Demodex infestation and serum immunoreactivity to Bacillus proteins in patients with facial rosacea. Ophthalmology 2010; 117:870–877; e1.
- Prieto VG, Sadick N, Lloreta J, et al. Effects of intense pulsed light on sun-damaged human skin, routine, and ultrastructural analysis. Lasers Surg Med 2002; 30:82–85.
- Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol 1988; 124:869–871.
- Craig JP, Chen YH, Turnbull PR. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci 2015; 56:1965–1970.
- Jiang X, Lv H, Song H, et al. Evaluation of the safety and effectiveness of intense pulsed light in the treatment of meibomian gland dysfunction. J Ophthalmol. 2016;2016:1910694.
- Toyos R, McGill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; a 3-year retrospective study. Photomed Laser Surg 2015; 33:41–46
- Gupta PK, Vora GK, Stinett S. Outcomes of intense pulsed light therapy for treatment of evaporative dry eye disease. Boston, MA: American Society of Cataract and Refractive Surgery; 2014.
Leave a Comment