
Dr. Shruti Chandra, C17895, Dr. Mahesh G, Dr. Giridhar Anantharaman, Dr. Jay Sheth
Abstract
Purpose:Researchers have correlated peripheral retinal ischemia with severity of diabetic retinopathy, but its relationship with macular edema and choroidal thickness(CT) remains unexplored. Current study aimed to elucidate these lacunae by assessing the connexion between peripheral retinal ischemia in DR, assessed on widefield fluorescein angiography, with macular edema and choroidal thickness
Methods: Prospective study of diabetic patients undergoing enhanced-depth imaging(EDI)-OCT for measurement of sub-fovealchoroidal thickness(SFCT), at 1500 & 3000µm nasally and temporally(N1500, N3000, T1500, T3000). Additionally, digital widefield fluorescein angiography(102°;WF-DFA)was performed on Spectralis (Heidelberg,Germany). Areas of peripheral ischemia, defined as area of capillary non-perfusion on WF images, were delineated manually & area calculated in pixels by a single grader. A Peripheral Ischaemic Index(PII), defined as ratio of total CNP areas and total area of WF image, was calculated. Correlation coefficients for various parameters with PII was calculated using Spearmans correlation.
Results:Analysis included 161 eyes of 86 patients with DR. Eighty-five eyes had NPDR and 76 eyes had PDR. The mean age was 57.9 ±8.7 years, and gender ratio of 2:3 (Male:Female). Overall, Central Macular Thickness (CMT) was negatively correlated with PII in all eyes with DR. In subgroup analysis, it was negatively correlated in PDR subgroup while it was positively correlated in NPDR eyes. However, none of these associations was statistically significant. Choroidal thickness at each loci had a negative correlation with PII in all eyes with DR (SFCT: p<0.004) and in NPDR eyes (SFCT:p<0.005). This correlation between choroidal thickness at all points with PII was statistically significant. However, in PDR group, although this relationship was negatively correlated, it was not statistically significant.
Conclusion: Macular choroidal thickness can be considered as a putative measure of choroidal blood flow and consequently a marker of tissue oxygenation. Current study establishes an inverse relationship between amount of peripheral retinal ischemia and macular choroidal thickness in DR thereby suggestive of concomitant diabetic choroidopathy with progressive peripheral retinal ischaemia.
INTRODUCTION AND AIM OF STUDY
Diabetic retinopathy(DR) incorporates a group of predominantlyvascular anomalies. The spectrum of disease has been classified according to the behavior of the retinal vasculature: (1) hyperpermeability (leakage and edema), which results in the development of lesions such as macular edema, peripheral hard exudates, and microaneurysms; and (2) hypoperfusion (ischemia), which results in enlargement of the foveal avascular zone (FAZ) in the macula and capillary nonperfusion(CNP) and retinal neovascularization in the retinal periphery1. Multiple studies have postulated that diabetic retinopathy originates in peripheral retina2. Capillary non perfusion has been hypothesized to be responsible for primary involvement of peripheral retina and it is potentially associated with progression of DR. It is this mid and peripheral CNP that has a correlation with tissue hypoxia and drives the overall ischaemia in the eye, thereby contributing to disease progression4. Consequently, identification of areas of CNP in the initial stages of disease mandate a reliable and excellent visualization of the peripheral retina.
The advent of widefield imaging has made it possible to visualize the peripheral retina4. The 30-degress and 50-degrees field of view cameras emerged are being widely used in clinical practice and are referred to as “standard” field of view. Accordingly, imaging angles larger than 30- or 50-degrees have been referred to as “widefield” or “wide-angle.” Several imaging platforms have been developed that provide a wide field view of the retina. These include the Pomerantzeff camera5,the Retcam (Clarity Medical Systems, Inc, Pleasanton, CA, USA), the Panoret-1000TM camera (Medibell Medical Vision Technologies, Haifa, Israel), the Optos® camera (Optos PLC, Dunfermline, UK), the Staurenghi lens (Ocular Staurenghi 230 SLO Retina Lens; Ocular Instruments Inc, Bellevue, WA, USA)6,and other wide-angle contact lenses,among others. The single-shot, non-steered wide field imaging capabilities of these modalities range from 20 degrees up to 200 degrees, albeit with variable image quality. As a result of these advances in WF imaging, we can now evaluate accurately the association of WF retinal nonperfusion on fluorescein angiogram with diabetic retinopathy severity.
As mentioned earlier, the pathogenesis and clinical signs of diabetic retinopathy are linked to retinal vascular damage, but evidence in literature insinuates parallel existence of choroidalvasculopathy. Choroidal vessels are responsible for the nutrient and oxygen supply of outer third of retina, and thereby are chiefly engaged in maintaining the vascularity of the fovea region consisting of predominantly the outer retinal layers7. Various angiographic, laser doppler flowmetry and histologic studies in eyes with diabetic retinopathy have shown proven occurrence of choroidalvasculopathy in form of delayed choroidal filling, reduced choroidal blood flow and choriocapillaris “dropout” (a nonperfusion and/or a complete attenuation of the choriocapillaris) respectively8-10. But these are invasive techniques of assessment. The advancement in Spectral domain optical coherence tomography in the form of Enhanced Depth Imaging(EDI) permits a non-invasive, 3-dimensional, higher definition view of the choroid till the choroidoscleral interface11. Many researchers have evaluated changes in CT in various stages of DR with variable results ranging from thickening, thinning, to even no changes as DR progresses from nonproliferative diabetic retinopathy (NPDR) to proliferative diabetic retinopathy (PDR)12-15. The literature remains abstruse with regards to the alterations in the choroid.
In this study, we intend to analyze the association between the aforementioned main pathologies in diabetic retinopathy, the peripheral capillary non perfusion on widefieldfluorescein angiography and choroidal thickness using EDI in the foveal region. Also, we aim to scrutinize the variations in these parameters through the continuum of diabetic retinopathy stages.
MATERIAL AND METHODS
INCLUSION CRITERIA AND DATA COLLECTION METHOD:Treatment-naive patients with diabetes presenting to the Vitreo-Retinal Clinic of Giridhar Eye Institute,Kerala, India, between July 2015 and September 2015 were included in the study.This study was conducted in accordance to the tenets of Declaration of Helsinki and was approved by the Institutional Review Board. Written informed consent was obtained from each patient. Patients with myopia more than 3 diopters (D), concurrent macular pathologies such as age-related macular degeneration (AMD) or choroidalneovascular membranes (CNV) or retinal vein occlusion (RVO) were excluded.The participants were divided into three groups: those with non proliferative diabetic retinopathy (NPDR), those with proliferative diabetic retinopathy (PDR). All patients underwent DFA (Spectralis HRA + OCT, Heidelberg Engineering, Heidelberg, Germany).
ACQUISITION AND ANALYSIS OF FLUORESCEIN ANGIOGRAMS: Widefield fluorescein angiography image acquisition – All digital widefield FA images were acquired with the widefield angiography module of the Spectralis and Heidelberg Retinal Angiograph HRA-2 (Heidelberg, Germany). The images were captured using the Staurenghi lens (Ocular Staurenghi 230 SLO Retina Lens; Ocular Instruments Inc, Bellevue, WA, USA) All patients received a standard infusion of 3 mL of 25% sodium fluorescein through the vein on the dorsum of hand. One early to mid-phase image (at 60 seconds to 90 seconds) centered on the optic disc, was chosen for analysis. The early to mid-phase image was graded for peripheral and macular ischemia. All widefield FA images were exported as .tiff files and analyzed. No image manipulation was performed prior to grading.
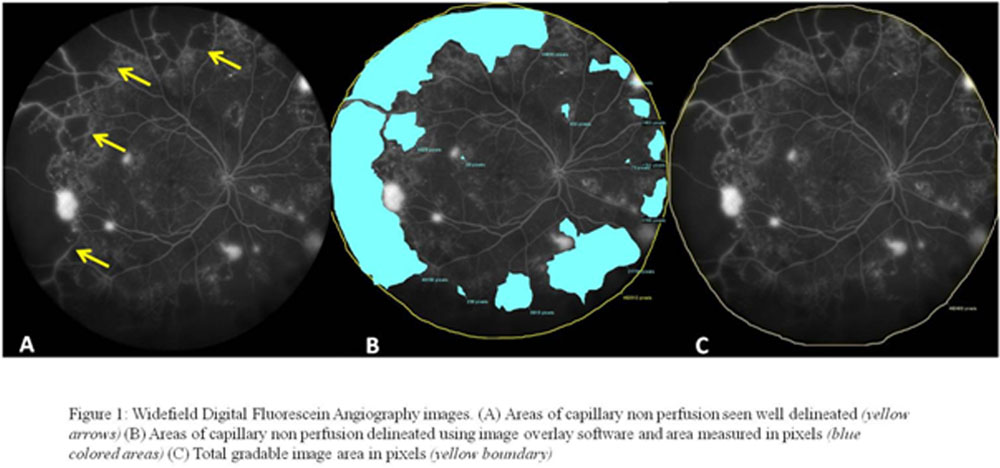
Quantification of peripheral ischemia – An ischemic index was calculated from the early to mid- phase FA. Briefly, areas of capillary non-perfusion outside the temporal vascular arcades were delineated manually using the image overlay software of the Heidelberg(Figure 1). The sum of all the areas of non-perfusion was calculated along with the total area of widefield image in pixels. Their ratio was designated as the Peripheral Ischaemic Index(PII)1. This was done by a single grader for all images.
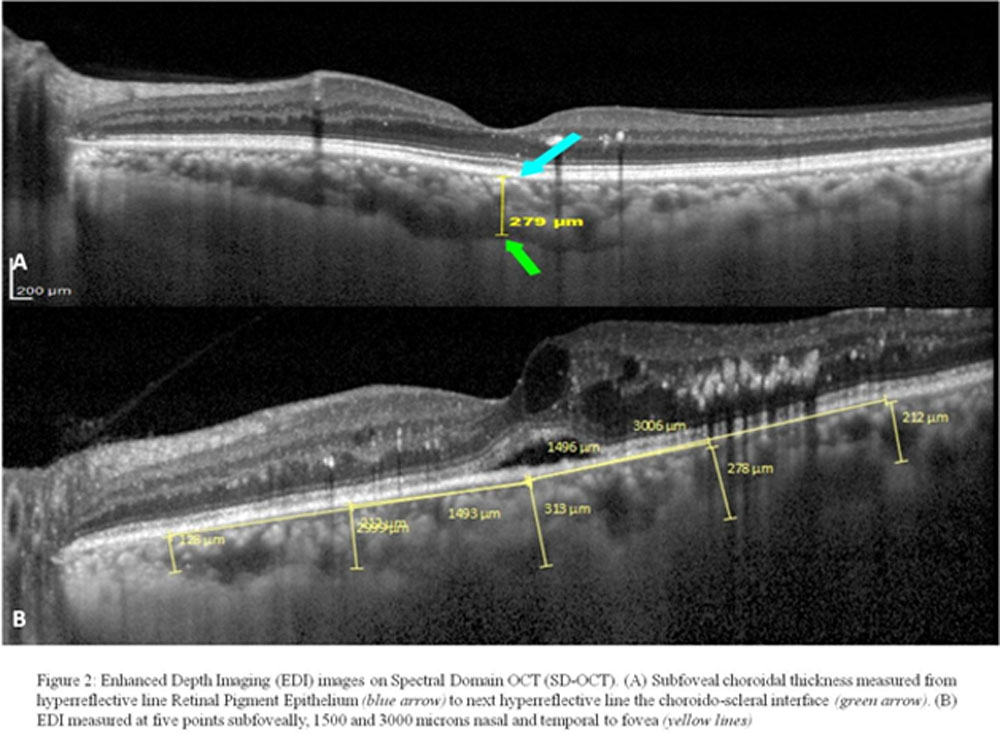
OPTICAL COHERENCE TOMOGRAPHY–DERIVED MEASUREMENTS OF CHOROIDAL THICKNESS: Enhanced depth imaging optical coherence tomography (EDI-OCT (Spectralis HRA + OCT, Heidelberg Engineering) was performed for all patients. CT was measured manually with the help of built-in callipers in OCT software. Measurements weremadefrom the outer portion of hyperreflective line corresponding to the retinal pigment epithelium to the inner portion of hyperreflective zone corresponding to choroido-scleral junction by a single masked observer. They were obtained in the subfoveal region (Subfovealchoroidal thickness; SFCT) and also at a distance of 1500µm and 3000µm from the locus of measurement of SFCT in nasal and temporal quadrants (N1500, N3000, T1500, T3000)(Figure 2). Automated central macular thickness (CMT) was also calculated using the 25-line raster scan protocol. CT and CMT were compared between the two groups.
STATISTICAL ANALYSIS: Clinical and imaging data were analyzed with frequency and descriptive statistics. The Spearman rank correlation was used to test for associations between variables. Snellen visual acuities were converted to logMAR (logarithm of the minimal angle of resolution) visual acuity for the purposes of statistical analysis. A P value of <0.05 was considered statistically significant. Statistical analyses were performed using SPSS software version 16 (SPSS, Inc, Chicago, Illinois, USA).
RESULTS
The study included 161 eyes of 86 patients diagnosed with diabetic retinopathy of which 85 had NPDR and 76 had PDR. The demographics and clinical characteristics of the study population are mentioned in table 1.
| TABLE 1: Baseline demographic and clinical characteristics of patients with Diabetic Retinopathy who underwent Widefield Fluorescein Angiography | |
| All patients (n=161) | |
| Age in years, Mean (SD) | 57.91 ( 8.75) |
| Female sex, n (%) | 64 (39.8) |
| Affected eye- Right, n (%) | 80 (49.7) |
| Diabetes duration in years, Mean (SD) | 15.60 (7.14) |
| Type of Diabetic retinopathy
NPDR, n (%) PDR, n (%) |
85 (52.8) 76 (47.2) |
| CSME
Present, n (%) Absent, n (%) |
82 (50.9) 79 (49.1) |
| NPDR – Non proliferative diabetic retinopathy, PDR – Proliferative diabetic retinopathy, CSME – Clinically Significant Macular Edema, CMT – Central macular Thickness, SFCT- SubfovealChoroidal Thickness | |
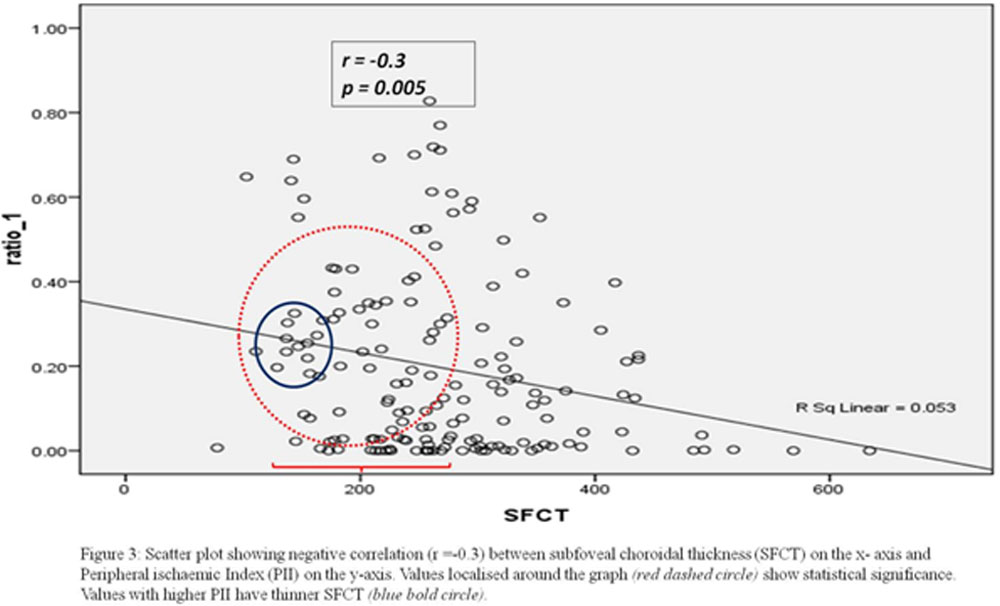
There was no significant correlation between PII and CMT in both groups. In the NPDR group, the PII was negatively correlated with CT which was statistically significant at all foci of measurements. On the other hand, although the PII had a similar negative correlation with CT in PDR group, it was not statistically significant (Table 2). The scatter plot of the relationship between PII and SFCT showed a downsloping graph. The values with higher PII have a thinner SFCT (Figure 3).
| TABLE 2: Correlation among variables measured with Peripheral Ischaemic Index (PII) in both Non Proliferative and Proliferative Diabetic Retinopathy groups | ||||
| Variables | NPDR
CC (r) P value |
PDR
CC (r) P value |
||
| CMT | 0.16 | 0.12 | -0.14 | 0.20 |
| SFCT | -0.30 | 0.005 | -0.19 | 0.08 |
| CT 1500 m N | -0.41 | <0.001 | -0.16 | 0.16 |
| CT 1500 m T | -0.28 | 0.009 | -0.09 | 0.39 |
| CT 3000 m N | -0.45 | <0.001 | -0.10 | 0.37 |
| CT 3000 m T | -0.28 | 0.007 | -0.01 | 0.91 |
| CC(r) – correlation coefficient, CMT- Central Macular Thickness, SFCT – SubfovealChoroidal Thickness, CT 1500 m N & T- Choroidal thickness at 1500 m Nasal and Temporal to fovea, CT 3000 m – Choroidal thickness at 3000 m Nasal and Temporal to fovea | ||||
DISCUSSION
It is well known that diabetic retinopathy is primarily a vascular disease affecting predominantly the retinal capillaries. Capillary non perfusion is conjectured to be responsible for DR progression. Additionally, extent of CNP tends to escalate with severity of DR2. Subsequent to its introduction in clinical ophthalmology WF fluorescein angiography(FA) has been observed to be valuable in assessment of various retinal pathologies like diabetes, vein occlusions, choroidal masses, retinal vasculitis, uveitis and retinopathy of prematurity to name a few. Quite a substantial amount of work has been done with regards to relevance of WF FA in vein occlusions. The total area of capillary non perfusion has been employed as a tool to classify central vein occlusions as non ischemic, minimally, moderately or markedly iscemic16. This has helped in treatment and prognostication of disease. After a thorough pubmed literature review, we came across very few studies have utilized WF FA in DR eyes and considered the relationship between CNP and its correlation with the severity of DR. Furthermore, rather fewer studies have researched the relationship between CNP and central macular thickness(CMT). To be noted among them is the work done by Dawn A et al1, who investigated the patterns of peripheral and central ischaemia in diabetic retinopathy using ultra WF FA. Along with identifying macular ischemia, they also measured the CMT. They put forth the following outcomes of their study: firstly, no relationship between peripheral ischemia or leakage was observed with macular edema; secondly, the retina is thinner in presence of macular but not peripheral ischaemia and lastly, poor visual acuity was associated with macular but not peripheral ischemia. Similar to results quoted by Dawn et al, our study also did not find any correlation between presence of increased CMT and peripheral CNP expressed as the peripheral ischemic index(PII). But, it was the absence of macular edema that negatively correlated with PII and this was statistically significant (r= -0.24, p=0.02). That is with increasing peripheral ischaemia there is associated decrease in CMT. We postulate that this could be attributed to coexistent central/macular ischemia, leading to macular thinning.
The choroid is primarily composed of blood vessels with nominal connective tissue. It provides vascular, nutritional, and metabolic support to the outer retinal layers including the RPE and photoreceptors14. Hence, CT as measured on EDI-OCT is highly indicative of vascular status of the outer retinal layers. Numerous published studies have attempted to decipher the complex relationship between subfovealchoroidal thickness and severity of diabetic retinopathy. Querques et al,13 have shown a reduction in CT in patients with diabetes with retinopathy changes as compared to those without retinopathy changes. Vujosevic et al12 have similarly shown a reduction in macular and peripapillaryCT with increasing levels of retinopathy changes (No DR to NPDR to PDR).This thinning of choroid is hypothesized to be a resultant of reduced choroidal blood flow as confirmed by histological and Doppler flow studies7.In contrast, Kim et al have shown significant increase in CT as DR progressed from NPDR to PDR stage.15 Also, they found that SFCT was mildly reduced in eyes with NDR and mild NPDR as compared to healthy subjects. In a large population-based study, Xu et al14 have shown choroidal thickening in patients with diabetes as compared to those without diabetes. However, they did not find any significant difference in CT associated with the presence of retinopathy changes or even the stage of retinopathy. Our study revealed a negative correlation between PII in NPDR eyes and SFCT (r= -0.30, p= 0.005), CT at 1500 m N (r = -0.41, p= <0.001) & T (r= -0.28, p= 0.009) and CT at 3000m N (r= -0.45, p= <0.001) &T (r= -0.28, p= 0.007). In addition, in eyes with PDR there was no correlation between CT and PII. In explanation of the aforementioned results we postulate, presence of concomitant choroidalvasculopathy in the early stages of retinopathy, as indicated by decreasing CT with increasing peripheral ischaemia in NPDR eyes. However, in PDR eyes the lack of correlation between CT and PII is suggestive of extensive preexisting diabetic retinopathy and choroidopathy, which is unlikely to worsen.
The strengths of our study include the prospective study design and adequate sample size. Secondly, assessment of peripheral ischaemia was done on WF FA which improves identification of CNP areas thereby minimizing chances of missing out CNP areas which could be missed on standard FA. Also to the best of our knowledge this study is unique as it looks at relationship between CT and peripheral ischaemia in diabetic retinopathy eyes which has not been studied formerly. It also looks at quantitative alterations in the choroid with increasing severity of DR.
Our study has its limitations in the fact that indocyanine green angiography was not performed which could have provided additional information regarding existence of choroidalvasculopathy. Also, qualitative assessment of choroidal vasculature on spectral domain OCT would also ass to our understanding of the disease pathology.
CONCLUSION
Macular choroidal thickness can be considered as a putative measure of choroidal blood flow and consequently a marker of tissue oxygenation. Current study establishes an inverse relationship between amount of peripheral retinal ischemia and macular choroidal thickness in DR thereby suggestive of concomitant diabetic choroidopathy with progressive peripheral retinal ischaemia
REFERENCES
- Dawn A. Sim, Pearse A. Keane, RanjanRajendram, Michael Karampelas, SenthilSelvam, Michael B. Powner, Marcus Fruttiger, Adnan Tufail, And Catherine A. Egan. Patterns of Peripheral Retinal and Central Macula Ischemia in Diabetic Retinopathy as Evaluated by Ultra-widefield Fluorescein Angiography. Am J Ophthalmol 2014;158: 144–153
- Niki T, Muraoka K, Shimizu K. Distribution of capillary nonperfusion in early-stage diabetic retinopathy. Ophthalmology 1984;91:1431–9
- Shimizu K, Kobayashi Y, Muraoka K. Midperipheral fundus involvement in diabetic retinopathy. Ophthalmology 1981;88: 601–12.
- Wessel MM, Aaker GD, Parlitsis G, et al. Ultra-wide-field angiography improves the detection and classification of diabetic retinopathy. Retina 2012;32:785–91
- Equator-pluscamera.InvestOphthalmol.1975;14(5): 401–406
- Staurenghi G, Viola F, Mainster MA, Graham RD, Harrington PG. Scanning laser ophthalmoscopy and angiography with a widefield contact lens system. Arch Ophthalmol. 2005;123(2):244–252
- Kur J, Newman EA, Chan-Ling T. Cellular and physiological mechanisms underlying blood flow regulation in the retina and choroid in health and disease. ProgRetin Eye Res. 2012; 31(5):377– 406
- Shiragami C, Shiraga F, Matsuo T, Tsuchida Y, Ohtsuki H. Risk factors for diabetic choroidopathy in patients with diabetic retinopathy. Graefes Arch ClinExpOphthalmol. 2002; 240(6):436–442
- Fukushima I, McLeod DS, Lutty GA. Intrachoroidal microvascular abnormality: a previously unrecognized form of choroidal neovascularization. Am J Ophthalmol. 1997; 124(4):473–487
- Hidayat AA, Fine BS. Diabetic choroidopathy: light and electronmicroscopic observations of seven cases. Ophthalmology
- Yeoh J, Rahman W, Chen F, et al. Choroidal imaging in inherited retinal disease using the technique of enhanced depth imaging optical coherence tomography. Graefes Arch ClinExpOphthalmol. 2010; 248(12):1719–1728
- Vujosevic S, Martini F, Cavarzeran F, Pilotto E, MidenaE.Macular and peripapillarychoroidal thickness in diabetic patients. Retina 2012;32(9):1781-90.
- Querques G, Lattanzio R, Querques L, Del Turco C, Forte R, Pierro L, et al. Enhanced depthimaging optical coherence tomography in type 2 diabetes.InvestOphthalmol Vis Sci 2012;53:6017–24.
- Xu J, Xu L, Du KF, Shao L, Chen CX, Zhou JQ, et al. Subfovealchoroidal thickness in diabetes and diabetic retinopathy. Ophthalmology 2013;120(10):2023-8.
- Kim JT, Lee DH, Joe SG, Kim JG, Yoon YH.Changes in choroidal thickness in relation to the severity of retinopathy and macular edema in type 2 diabetic patients. Invest Ophthalmol Vis Sci 2013;54(5):3378-84
- Welch JC, Augsburger JJ. Assessment of angiographic retinal capillary nonperfusion in central vein occlusion. Am J Ophthalmol 1987 Jun 15;103(6):761-6
Leave a Comment