
Dr. Prashant Jain, J17555, Dr. Mahesh G, Dr. Giridhar Anantharaman
Abstract:
Aim:To have an insight of the outcome of PDT with intravitreal anti VEGF for patients with PCV in a real world population
Methods:Retrospectivereview of 42 eyes of 40 patients(mean age 64.3 year) with BCVA 20/60 or better and mean follow up of 40 months(Range 12-71 months)treated with PDT and anti VEGF for ICG proven PCV
Results:Mean BCVA was significantly better(p <0.001) from 0.22 logMARat baseline to 0.15 at last visit.Polypoidal lesion regressed in 89.2% and BVN in 70.3% after combined therapy.Meangreatest linear diameter reduced significantly(p <0.001) from 7.22 to 4.11 mm.Central choroidal thickness was significantly reduced(p <0.001) from 275.12 to 239.24 µm at last visit.Mean number of PDT was 1.17 with mean injections 6.38.At final visit 66.7%(p <0.001) were having fluid free retina.No complication of subretinal hemorrhage was noted
Conclusion:Long term effect of PDT with anti VEGF appears to be safe and effective treatment for PCV with better outcomes in real world setting
Introduction
Polypoidal choroidal vasculopathy (PCV) was first described by Yannuzzi et al. in 1990 as having two distinct components of branching vascular network (BVN) and terminal aneurysmal dilatations or “polyps” associated with or without serous/hemorrhagic detachment of retinal pigment epithelium (RPE)[1].It’s a question that has beencontroversial in ophthalmology over many years: Is PCV a subtype of neovascular agerelatedmacular degeneration (AMD)or a separate clinical entity? Even moreimportant, does this distinction affecttreatment and outcomes?Genetic studies suggest that PCV isa type of choroidal neovascularization(CNV), and other research has demonstrated that the anti-vascular endothelial growth factor (VEGF) therapies used for AMD may improve vision inpatients with PCV. Yet, in contrast toAMD, some PCV patients fail to respond to anti-VEGF treatment and do better with verteporfin photodynamictherapy (PDT). Recent studies indicatethat the combination of PDT and ananti-VEGF agent provides added benefitin treating PCV.
Theprevalence of PCV varies among different ethnicgroups and has a higher prevalence in Asiansand Blacks as compared to Caucasians.[2] PCVaccounts for 25-50% of Asian patients presentingwith presumed neovascular AMD,[3-6] whereasit is seen in only 5-10% of Caucasian patients with neovascular AMD.[7-9] There is a marked male preponderance of 63%–78.5% and only5.9%–24.1% have bilateral disease.[2,10,11,12]
The Beijing Eye Study 2011, a population-based study in NorthernChina, attempted to estimate the prevalence of PCV using a combined clinical and optical coherencetomography (OCT) criteria to define the presence of PCV. In this study, PCV was defined as anelevated orange-red lesion on fundus photographs, characterized by a double layer sign and highdome-shaped pigment epithelial detachment on the OCT images. With this definition, they found aPCV prevalence of 0.3% ± 0.1%.[11]
The goldstandard for diagnosing PCV is by indocyanine green angiography (ICG) which shows the presence of a branchingchoroidal vascular network and/or clusters of dilated polypoidal lesions.[13,14]
The treatment options for PCV include anti VEGF and verteporfin photodynamictherapy (PDT). Anti-VEGF agents improve visual function by restoring normal retinal thickness, reducing the sub retinal fluid (SRF), taking care of BVN and reduce re-uptake of VEGF after PDTwhile PDT facilitates polyp regression. The efficacy of these treatments as monotherapy versus combination therapywas previously evaluated in a randomized controlled trial (EVEREST)[14] The results showed that PDT, usedin combination with ranibizumab or used alone, is superior to ranibizumab monotherapy in achieving polypregression.
However, there are very few study in literature on the efficacy of combined therapy with PDT and intravitreal anti VEGF from the Indian subcontinent.The aim of this study was to have an insight of the outcome of PDT with intravitreal anti VEGF for patients with PCV in patients having good visual acuity on initial presentation in a real world population.
Material and Methods
This is a single centre retrospective case study included 42symptomatic eyes of 40 patients having best-corrected visual acuity (BCVA) better than 20/60 at baseline with subfoveal PCVtreated with either full fluence or reduced fluence PDT therapy along with intravitreal anti VEGF at Department of Vitreo-retina, Giridhar Eye Institute, Kochi, India, between January 2011and December 2015. All patients received a comprehensive ocular examination including BCVA and dilated fundus examination. The diagnosis of PCV was confirmed by clinical examination, spectral domain optical coherence tomography (SD-OCT) (Spectralis; Heidelberg Engineering, Inc., Heidelberg, Germany), fundus fluorescein angiography (FFA), indocyanine green angiography (ICG), and fundus autofluorescence(FAF) imaging (Heidelberg Retina Angiograph 2; Heidelberg Engineering, Heidelberg, Germany).
Patients who were ICG proven cases of PCV and BCVA 20/60 or better at the time of combined therapy were included in the study. Patients who were followed for at least 12 months were only included in the study. Eyes with the presence of RPE tear or other maculopathies such as AMD, diabetic macular edema, or high myopia were excluded. Patient in whom ICG was not performed at three month visit after combined PDT were also excluded.
Diagnosis was based on the presence of polypoidal lesions along with BVN seen on ICG in early frames. Leakage in the form of stippled hyperfluorescence on FFA was also noted. Patient having BVN without polyp on ICG were documented as cases of PCV only. The ICG based greatest linear diameter (GLD) of the lesion was determined to cover the polypoidal lesions and surrounding BVN. PDT was done using light energy of 50 J/cm2 for 83 s (600 mW/cm2) after 6 mg/m2verteporfin injection. For reduced fluence PDT light energy of 25 J/cm2 with power 300 mW/cm2was used. Choice between full fluenceor reduced fluence PDT was done at the discretion of treating surgeon. It was followed by 1.25 mg of bevacizumab (Avastin; Genentech Inc., South San Francisco, California, USA) or 0.5 mg of ranibizumab (Lucentis, Genentech Inc., South San Francisco, California, USA), given intravitreal 3.5 mm from limbus using a 30-gauge needle under topical anesthesia with strict aseptic precautions within 24 hour after PDT. Patients were given the choice to choose between bevacizumab and ranibizumab according to the financial status.
Outcome measures included resolution of SRF on SD-OCT at 3 month and last visit and regression of polypoidal lesions/BVN on ICG done at 3 month after combined PDT. Comparison of baseline BCVA and BCVA at 3 month, 6 month and at final visit was done. The number of PDT and anti-VEGF injections required was recorded. Any ocular or systemic adverse event was noted. The intravitreal anti-VEGF injection was repeated at 4–6 weeks intervals if persistent SRF was seen on OCT. If active polypoidal lesions associated with SRF or subretinal hemorrhage were seen on ICG at follow up visits, retreatment with PDT combined with intravitreal anti VEGF was performed at the discretion of treating surgeon.
Statistical Analysis used was SPSS software version 16.0 (SPSS Inc., Chicago, IL, USA) to compare the logarithm of the minimal angle of resolution visual acuity at presentation and final follow-up. p < 0.05 was considered statistically significant.The differences between quantitative variables were analyzed using Wilcoxon signed rank test.
Since our study was a retrospective analysis of patient data from the electronic medical records, consent was not obtained. The study was conducted in accordance to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board.
Results
The mean age of patient was 64.29 ± 8.72 years. Out of 42 patients only one was of age less than 50 years. On analysis, 21 were female and 219 were male.The mean follow up period was 40.02 ± 10.21 months (Range 12-71 months). Demographic profile of the patients is given in table 1.
Table 1: Demographic Characteristics of the Population
| Characteristics | Summary Details (n =42) |
| Age (Years),Mean (SD) | 64.29 (8.719) |
| Age Category (Years), n (%) | |
| <50 | 1 (2.5) |
| ≥50 and <65 | 39 (97.5) |
| Gender, n (%) | |
| Male | 19 (47.5) |
| Female | 21 (52.5) |
| Follow up (Months),Mean (SD) | 40.02 (10.21); Range (12-71 months) |
| Systemic illness, n (%) | |
| Diabetes | 6 (14.3) |
| Hypertension | 8 (19.0) |
| Both | 5 (11.9) |
| Nil | 23 (54.8) |
SD- Standard deviation
The mean BCVA at baseline was +0.23 ± 0.17 logMAR unit (Mean snellen’s 20/33). PCV was classified as serosanguineous (26 eyes;61.9%), haemorrhagic (7 eyes; 16.7%) and mixed (9 eyes; 21.4%) based on biomicroscopy. On ICG, polyp was seen in 37 eyes (88.1 %) and only in one case pulsatile polyp was seen on dynamic video ICG. Out of 42 eyes BVN was seen in 37 (88.1%). The ICG based mean greatest linear diameter (GLD) of the lesion (polyp and BVN) was 7.22 ± 4.98 mm. On FFA stippled leakage was found in 26 eyes (61.9%). On SD-OCT SRF was present in 100 percent of cases at baseline. The mean central choroidal thickness (CCT) measured on EDI mode of SD-OCT was 275.12 ± 84.9 µm. Double layer sign (DLS) was found in 38 eyes (90.5%) on OCT.The baseline characteristics of the study group is given in table 2.
Table 2: Baseline Characteristics of the study Population
| Characteristics | Summary Details (n =42) |
| BCVAlogMAR, Mean (SD) | 0.23 (0.165); Mean snellen’s 20/33 |
| Type of PCV | n (%) |
| Hemorrhagic | 7 (16.7) |
| Mixed | 9 (21.4) |
| Serosanguineous | 26 (61.9) |
| Presence of leakage on FFA | |
| No | 16 (38.1) |
| Yes | 26 (61.9) |
| Presence of POLYP on ICG | |
| No | 5 (11.9) |
| Yes | 37 (88.1) |
| Presence of pulsatile polyp on dynamic ICG | |
| No | 41 (97.6) |
| Yes | 1 (2.4) |
| Presence of BVN on ICG | |
| No | 5 (11.9) |
| Yes | 37 (88.1) |
| GLD of lesion (mm), Mean (SD) | 7.22 (4.98) |
| CCT (µm), Mean (SD) | 275.12 (84.975) |
| Presence of SRF | 42 (100) |
| Presence of DLS on OCT | |
| No | 4 (9.5) |
| Yes | 38 (90.5) |
PDT- Photodynamic therapy; BVN- Branch vascular network; ; SRF- Serous retinal fluid; FFA- Fundus fluorescence angiography; ICG- Indo cyanine green angiography; GLD- Greatest linear diameter; ; CCT- central choroidal thickness; DLS- Double layer sign
Out of 42 eyes, primary modality of treatment was combined therapy of PDT and anti VEGF in 19 eyes (45.2%). Intravitreal anti VEGF monotherapy was used as primary treatment in 23 (54.8%) eyes. In monotherapy group, patientswereshifted to combined therapy after non-responding to atleast three loading dose of anti VEGF injections. Full fluence PDT was done in 35and reduced fluence in 7 eyes. Intravitreal bevacizumab was given in 17 eyes (40.4%) and ranibizumab in 13 (31.0%). In 12 eyes triamcinolone was administeredalong with PDT.
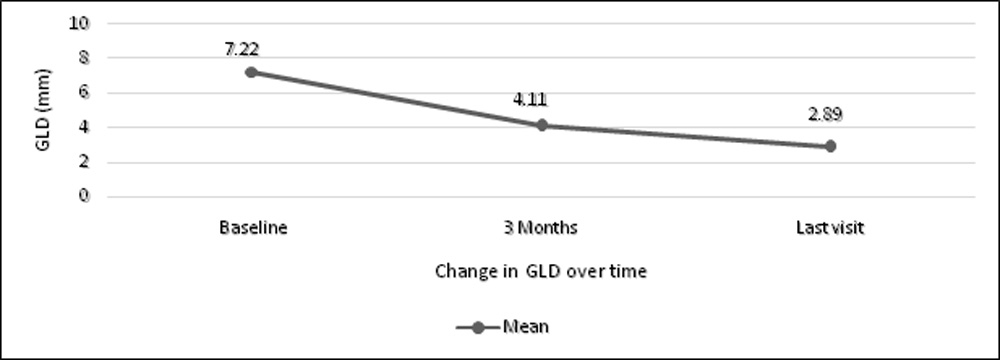
Assessing the PCV status 3 months after combined therapy, out of 37 eyeswith polyps at baseline 33 (89.2 %) shows regression of polyps. When we compared the polyp regression rate between two groups of full or reduced fluence PDT the p-value was not statistically significant (p=0.35) shown in table 3.1. BVN was regressed in 26 eyes of 37 (70.27%) having BVN at baseline. The p-value (0.30) was not statistically significant between two group of full fluence or reduced fluence PDT (Table 3.2). The size of GLD was reduced significantly (p<0.001)at 3 month and at last visit after combined therapy shown in table 4 and figure 1. On FFA none of the patients had leakage 3 month after combined PDT.
Table 3.1: POLYP Regression rate between two PDT Groups
| ICG POLYP | PDT | p value | ||
| FF PDT | RF PDT | Total | ||
| Yes | 27 | 6 | 33 | 0.351 |
| No | 4 | 0 | 4 | |
| Total | 31 | 6 | 37 | |
FF PDT- Full fluence photodynamic therapy; RF PDT- Reduced fluence photodynamic therapy
Table 3.2: BVN Regression rate between two PDT Groups
| BVN | PDT | p value | ||
| FF PDT | RF PDT | Total | ||
| Yes | 22 | 4 | 26 | 0.296 |
| No | 11 | 0 | 11 | |
| Total | 33 | 4 | 37 | |
Fisher’s exact test; BVN- Branch vascular network; FF PDT- Full fluence photodynamic therapy; RF PDT- Reduced fluence photodynamic therapy
Table 4: Change in GLD over 3 months after PDT
| Variable | Descriptive Statistics
(n =42) |
p value | |
| Initial GLD (mm), Mean (SD) | 7.22 (4.998) | <0.001** | |
| GLD (mm) at 3 Months, Mean (SD) | 4.11 (4.362) |
** indicates a significant association (p-value <0.05); Wilcoxon Signed Rank test; GLD- Greatest linear diameter; PDT- Photodynamic therapy
Figure1: Line Graph showing Change in greatest linear diameter(GLD) over 3 months
The central choroidal thickness was significantly reduced over a period of time after PDT and antiVEGF which is shown in figure 2. When we assessed the CCT between baseline and at 3 months and final visit the p-value was statistically significant(p<0.001) which is shown in table 5.1 and 5.2.
Figure 2: Assessment of central choroidal thickness over period of time in study group
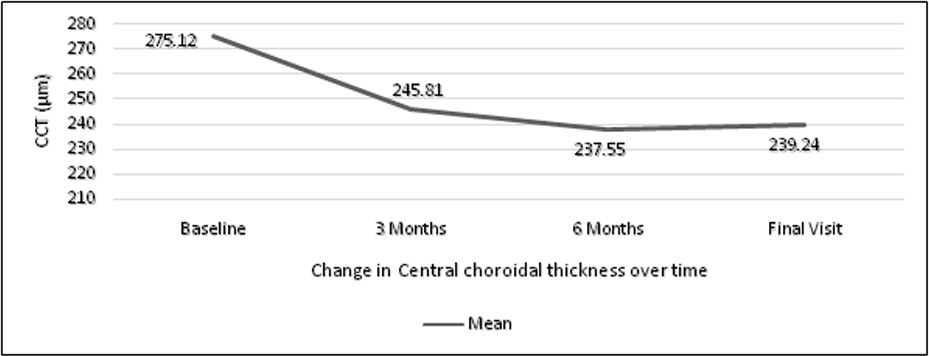
Table 5.1: Assessment of CCT – Baseline & post PDT at 3 Months
| Variable | Descriptive Statistics(n =42) | pvalue |
| Initial CCT (µm), Mean (SD) | 275.12 (84.975) | <0.001** |
| CCT 3 Months, Mean (SD) | 245.81 (73.257) |
** indicates a significant association (p-value <0.05); Paired t test; CCT- central choroidal thickness; PDT- Photodynamic therapy
Table 5.2: Assessment of CCT – Baseline and Final Visit
| Variable | Descriptive Statistics(n =42) | p value |
| Initial CCT (µm), Mean (SD) | 275.12 (84.975) | <0.001** |
| Final CCT, Mean (SD) | 239.24 (68.613) |
** indicates a significant association (p-value <0.05); Wilcoxon Signed Rank test; CCT- central choroidal thickness
Now if we analyze the fluid free retina i.e. presence of SRF on OCT at follow up visit, SRF was resolved in 40 eyes (95.2 %) at 3 months and at final visit 28 eyes (66.7 %) was having fluid free retina. The status of SRF is shown in figure 3 at every visit. On assessing the SRF status between baseline and at 3 months and final visit p value was statistically significant(p<0.001) which is shown in table 6.1 and 6.2.
Figure 3:Proportion of Patients with SRF over period of time in study group
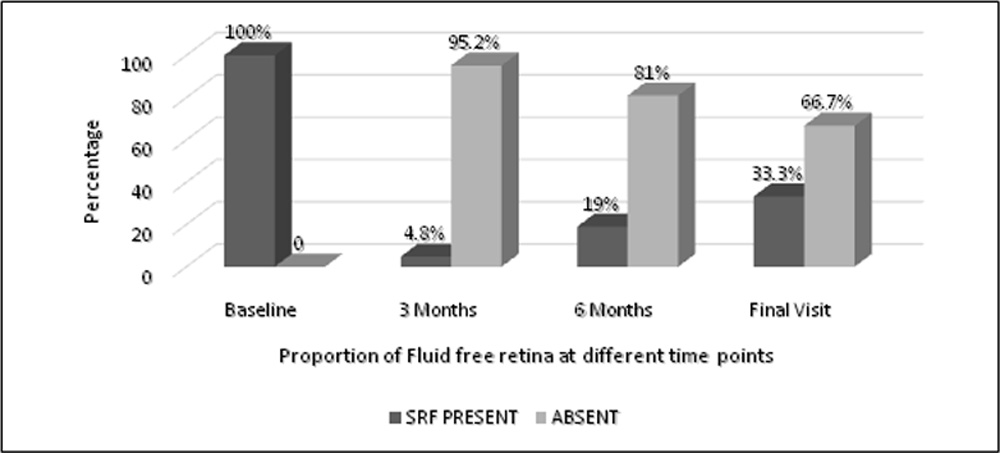
Table 6.1: Assessment of SRF – Baseline & post PDT at 3 Months
| SRF | Summary Details (n =42) | p value |
| Baseline, n (%) | <0.001** | |
| Present | 42 (100) | |
| Absent | 0 | |
| SRF 3 Months | ||
| Present | 2 (4.8) | |
| Absent | 40 (95.2) |
** indicates a significant association (p-value <0.05); McNemar’s test; SRF- Serous retinal fluid; PDT- Photodynamic therapy
Table 6.2: Assessment of SRF – Baseline and Final Visit
| SRF | Summary Details (n =42) | p value |
| Baseline | <0.001** | |
| Present | 42 (100) | |
| Absent | 0 | |
| Final SRF | ||
| Present | 14 (33.3) | |
| Absent | 28 (66.7) |
** indicates a significant association (p-value <0.05); McNemar’s test; ;SRF- Serous retinal fluid
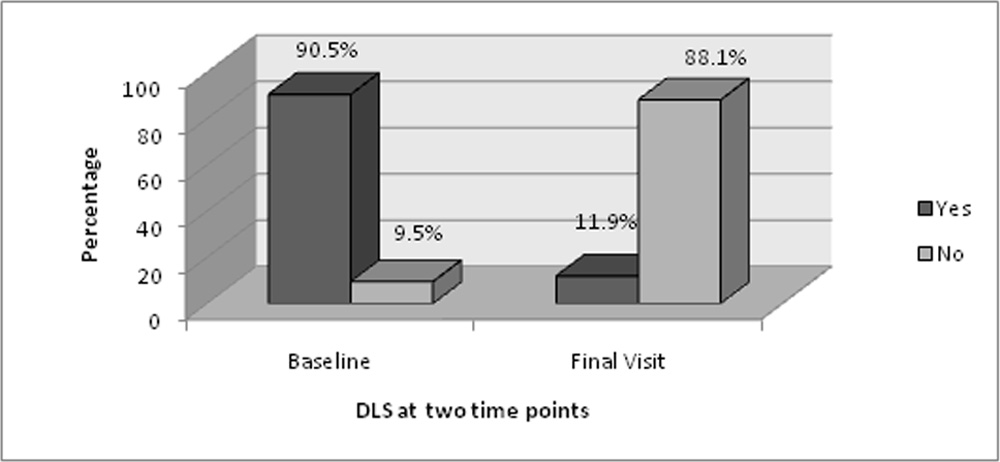
When we closely look into the SRF status throughout the study we found out that out of 42 eyes, 40 were not having any fluid at 3 month but on long term follow up there was reappearance of SRF in 25 eyes with mean follow up period of 9.64 ± 5.24 months for reappearance. In 25 eyes of recurrence, 22 has polyp, 21 has BVN and 18 has both on initial presentation. Out of 42 eyes, 17 remained dry throughout the study till last visit with mean follow up of 27 months. Out of 38 eyes having DLS on OCT at baseline, 37 eyes was having regression of DLS i.e. either reduced or resolved at final visit (Figure 4).
Figure 4: Status of Double layer sign (DLS) on SD-OCT over period of time
The mean number of PDT received in the study group was 1.17 ± 0.54 with median 1 (Table 7.1). 37 patient (88.1%) received only one PDT. In 5 eyes more than one PDT was given. Total number of injections given throughout the study was 268 with mean of 6.38 ± 6.15 and median of 4.50 (Table 7.2). Before PDT i.e. in the group who received anti VEGF monotherapy and was non responder, total injections given was 100 with mean of 4.35 ± 2.93 and median of 4 injections. In 21 eyes (50%) less than or equal to 4 intravitreal injections were give and in 8 eyes (19.04%) more than or equal to 10 injections were given in the study group.
Table 7.1: Numberof PDT received in the study group
| Characteristics | Summary Details (n =42) |
| PDT needed | |
| 1 | 37 (88.1) |
| ≥2 | 5 (11.9) |
| Mean (SD) | 1.17 (0.54) |
| Median | 1 |
PDT- Photodynamic therapy
Table 7.2: Number of IV Injections received in the study group
| IV Injections | Summary Details (n =42) |
| Total no. of Injections | 268 |
| Mean (SD) | 6.38 (6.152) |
| Median | 4.50 |
The BCVA logMAR value at baseline and at subsequent visit at 3 month, 6 month and at last visit is shows in table 8 and figure 5. On assessing the BCVA between baseline and at 3 month, the p-value was significant (p=0.001) with improvement in BCVA. Vision was stable without any deterioration between baseline and final visit (p=0.64) (Table 9.1 and 9.2). Out of 42 eyes one eye has BCVA worse than 20/60 on final visit and has BVN only without any polyp on initial ICG and underwent full fluence PDT.
Table 8: Assessment of BCVA over period of time in study group
| Variable | Descriptive Statistics(n =42) |
| Initial BCVA, Mean (SD) | 0.22 (0.165); Snellen’s 20/33 |
| BCVA 3 Months, Mean (SD) | 0.15 (0.130); Snellen’s 20/28 |
| BCVA 6 Months, Mean (SD) | 0.18 (0.155); Snellen’s 20/30 |
| Final BCVA, Mean (SD) | 0.21 (0.194); Snellen’s 20/32 |
BCVA- Best corrected visual acuity
Figure 5: Line Graph showing Change in mean logMAR BCVA over time
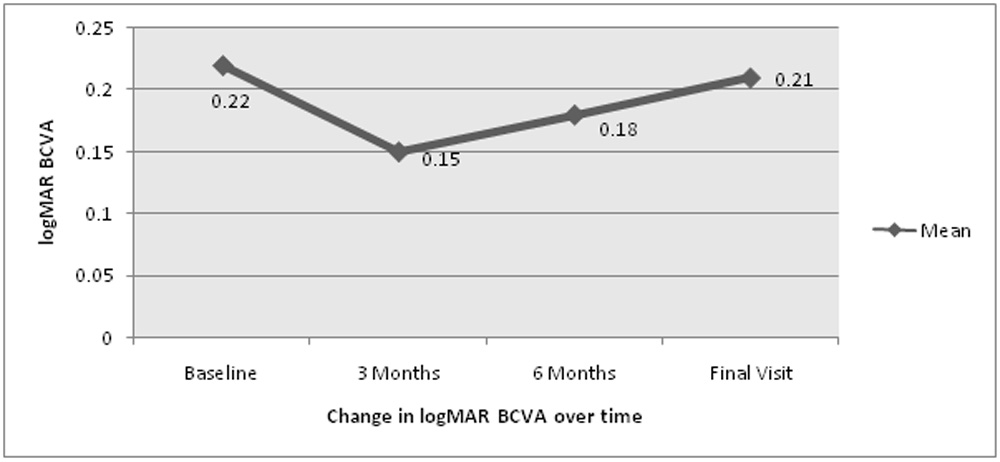
Table 9.1: Assessment of BCVA – Baseline & Post PDT at 3 Months
| Variable | Descriptive Statistics(n =42) | p value |
| Initial BCVA, Mean (SD) | 0.22 (0.165) | 0.001** |
| BCVA 3 Months, Mean (SD) | 0.15 (0.130) |
** indicates a significant association (p-value <0.05); Wilcoxon Signed Rank test; PDT- Photodynamic therapy; BCVA- Best corrected visual acuity
Table 9.2: Assessment of BCVA – Baseline and Final Visit
| Variable | Descriptive Statistics(n =42) | p value |
| Initial BCVA, Mean (SD) | 0.22 (0.165) | 0.638 |
| Final BCVA, Mean (SD) | 0.21 (0.194) |
Wilcoxon Signed Rank test; BCVA- Best corrected visual acuity
In one of the patient, 4 sitting of PDT was done and on last visit no activity was present and patient maintaining BCVA 20/20 (logMAR 0.0).In other patient after PDT there was residual BVN with extra large pigment epithelial detachment(PED) which was not settling after repeated intravitreal anti VEGF, then focal laser was given to feeder vessel shown on ICG and BVN completely resolved with flattening of PED and no disease activity after 41 month of follow up with BCVA of 20/30.
Discussion
The aim of this study was to investigate the efficacy and long term effect of combining PDT as treatment for PCV in eyes having good visual acuity at baseline in an Indian population.There arevarious treatment options for PCV available which includes thermal laser, full fluence photodynamic therapy (FF PDT), reducedfluence PDT (RF PDT), and anti-vascular endothelial growth factor (anti-VEGF).
In recent years, thermal laser photocoagulation had been superceded by the superior efficacy of photodynamic therapy and subsequently anti-VEGF agents and it is mainly restricted to patients having extra foveal polyp.
Most studies on PDT monotherapy for PCV have reported favorable short to midterm results, with stable or improved vision and regression of polyps achieved in 80%-95% of eyes.[15-19] Although the short-term visual outcome of PDT monotherapy for PCV appeared promising, a 5-year multi-centered prospective study of 65 PCV patients showed that patients had a mean decline of 0.21 logMAR units in best corrected visual acuity from baseline to 5 years after the initiation of PDT monotherapy.[20]
The standard dose of PDT might beassociated with possible adverse effects on thechoriocapillaries surrounding the treatment zonedue to up-regulation of VEGF.[21,22] As a result, variations of PDT techniques including reduced-fluence PDT(300 mW/cm2, light dose 25 J/cm2) or evenquarter-fluence PDT have been developed.[23]
Yamashita et al, showed that the use of reducedfluence PDT (light dose 25 J/cm2) in 38 PCVpatients resulted in significant improvement inmean logMAR BCVA from baseline of 0.43 to0.28 at 12 months and that mean visual acuityremained at 0.29 logMAR after 24 months.[24]Improved or stable vision was achieved in 95%of treated patients at 24 months. In our study we used both modality of PDT treatment and there was no significant difference on the outcome of PCV. None of our patient in whom we gave full fluence PDT developed any complication of haemorrhage or chorio retinal atrophy. In one of our patient we gave 4 times PDT and after follow up of 68 months patient is maintaining BCVA 20/20.
Hikichi et al, reported the results of their two year prospective study on the use of intravitrealranibizumab monotherapy in 75 PCV patients.[25]All patients received three monthly loadingdoses of intravitreal ranibizumab injectionsfollowed by as-needed re-injections. MeanlogMAR BCVA improved from 0.59 at baselineto 0.37 and 0.41 logMAR at 12 months and 24months respectively. Complete regression ofpolyps was achieved in 40% and 25% of patientsat 12 and 24 months, respectively. Despite thepromising visual outcome, BVN persisted in allpatients and tended to increase in size during thesecond year.[25] In current study also intravitreal anti VEGF monotherapy was used as primary treatment in 23 (54.8 %) eyes and all of them shifted to combined PDT treatment after non responding to the anti VEGF monotherapy .
Although PDT seems to be effective inimproving vision and inducing regression ofpolyps among PCV patients, it is not ideal inview of the high recurrence rate and the riskof complications such as post-PDT subretinalhemorrhage. The up-regulation of VEGF levelsin PCV eyes following PDT may account for thedevelopment of secondary CNV and recurrence of PCV. Therefore, adjunctive treatment withintravitreal anti-VEGF therapy at the time ofPDT may suppress the pro-angiogenic activityof VEGF. PDT in the form of combined therapyfor PCV is targeted to cause thrombosis of thepolypoidal lesions and anti-VEGF therapy maytackle the CNV-like BVN to reduce the amountof exudation caused by PCV lesions. Recentstudies have also suggested that combined PDTand intravitreal anti-VEGF therapy might resultin less post-PDT subretinal hemorrhage than PDT alone.[26,27]The beneficial effectsof combined PDT and anti-VEGF therapy havebeen confirmed by the EVEREST study, a phase3, double-blind, multi-center, randomizedcontrolled trial, which evaluated the efficacyof intravitreal ranibizumab monotherapyversus verteporfin PDT monotherapy versuscombined therapy with PDT and intravitrealranibizumab for treatment of PCV.[14] The studyshowed that both combination therapy andPDT monotherapy resulted in a significantlyhigher proportion of PCV eyes having completeregression of polyps on ICGA than ranibizumabalone at 6 months (77.8% vs. 71.4% vs. 28.6% respectively).[14] A retrospectivestudy by Saito et al compared PDT monotherapyin 32 PCV patients with 25 PCV patients treatedwith PDT plus intravitreal ranibizumab and allpatients were followed for at least 24 months.[28]Patients who received combined PDT andintravitreal ranibizumab were found to havebetter vision gain as compared to the controlgroup using PDT alone.
Wang et al., conducted a systematic review and meta-analysis thatanalyzed two randomized controlled trials and nine high quality retrospective studies, including a total of 543 PCV cases.[29] No significant difference in visual acuity was found between PDT monotherapy and combination therapy at three and six months, but the combination group performed better in terms of mean visual acuity change at 12 months (weighted mean differences (WMD) 0.11,95% CI 0.012, 0.21) and 24 months (WMD: 0.21; 95% CI: 0.054, 0.36; p = 0.008). Importantly, thestudy found that polyp regression, recurrence, central retinal thickness decrease and resolution of pigment epithelial detachment were not significantly different between the two groups. After 24 months, however, visual prognosis appeared to be more guarded.[30-37]
Through this study we try to analyze the real world experience of combined therapy of PDT and anti VEGF in eyes having good visual acuity at baseline in an Indian population. Demographically the mean age of presentation was 64.30 years with equal preponderance in male and female. If we look at the type of PCV then mainly it was serosanguineous with unilateral presentation in our study. In 54.8 percent of our patient first we tried anti VEGF as primary treatment and after no response we switch to combined therapy. We tried both form of PDT i.e. full and reduced fluence and the result was comparative in both group. After 3 month of therapy none of the patient was having leakage on FFA and SRF was resolved in 95.2 percent of patient. There was significant improvement in logMAR BCVA at 3 months (p-value 0.001) and at final visit BCVA was comparable with baseline vision. Mean follow up in our study was 40.02 months with range of 12 to 71 months. In real world setting we found out that after mean follow up of 40.02 months with minimum follow up of 12 months patient were maintaining good visual acuity (Mean snellen’s 20/32 at last visit) on long term after combined PDT and anti VEGF. In none of our patient there was sub retinal haemorrhage or any other complication till last follow up visit. Except one, all our patient was maintaining BCVA better or equal to 20/60. There was marked reduction in CCT and DLS on OCT and polyp and BVN regression with reduction in GLD diameter on ICG. 66.7 percent of the patient was having fluid free retina on last visit on SD-OCT with DLS regression in 88.1 percent. Mean number of injections given was 6.38 and mean number of PDT was 1.17. In one of our patient full fluence PDT was given four times with no chorio retinal atrophy at last visit with follow up of 68 months.
This real world experience in our study suggest that long term effect of PDT with anti VEGF appears to be safe and effective treatment for PCV with better outcomes and comparable with the studies conducted in western world (comparison chart shown in table 10) and further strengthen the superiority of combined treatment modality for treatment of sub foveal PCV with no or minimal risk of complication on long term follow up in an Indian population.
Table 10: Comparison with previous study of PDT with anti VEGF for PCV
| S. No | Study | Treatment | No of eyes | Interval between PDT and anti-VEGF | Visual Acuity (logMAR) | Mean No. of PDT | Mean No. of Injections | Polyp regression at 3 months | ||
| Initial | 3 M | 12 M | ||||||||
| 1 | SATO [38]
(2013) |
PDT+R | 40 | 2 days before PDT | 0.46 | 0.32 | 0.27 | 1.10 | 1.23 | 85.0% |
| 2 | GOMI[26]
(2010) |
PDT+B | 61 | 1 day before PDT | 0.48 | 0.36 | 0.36 | 1.43 | NA | 78.7% |
| 3 | RICCI[39]
(2012) |
RF PDT+R | 17 | 2 days after PDT | 0.45 | NA | 0.29 | 1.2 | 2.9 | 94.1% (at 12 months) |
| 4 | GOMI [40]
(2015) |
PDT+R | 37 | 7 days before PDT | 0.51 | 0.38 | 0.29 | NA | 6.8 | 69.7% |
| 5 | HATA M[41]
(2014) |
PDT+R | 95 | 3 days after PDT | 0.62 | 0.56 | 0.53 | 1.34 | NA | 63.2% (at 12 months) |
| 6 | SAITO [36]
(2014) |
PDT+R | 25 | 1-2 days before PDT | 0.30 | 0.52 | 0.59 | 1.4 | 4.5 | 100% |
| 7 | SAKURAI [42]
(2014) |
PDT+R | 17 | 1 day before PDT | 0.35 | NA |
0.38 |
1 | NA | 82.3% |
| 8 | LEE[43]
(2012) |
PDT+B | 36 | 7 days after PDT | 0.75 | 0.53 | 0.54 | 2.25 | 3.4 | NA |
| 9 | EVEREST [14]
(2012) |
PDT+R | 18 | <24 hour after PDT | 56.6 Letters ETDRS | Gain 7.4 Letters | Gain 10.9 Letters(6 month) | 1.4 | 3.9 | 72.2% |
| 10 | OUR STUDY
(2017) |
PDT+R/B | 42 | < 24 hour after PDT | 0.22 | 0.15 | 0.21 | 1.2 | 6.4 | 89.2% |
References
- Yannuzzi LA, Sorenson J, Spaide RF, Lipson B. Idiopathic polypoidal choroidal vasculopathy (IPCV) 1990;10:1–8.
- Byeon SH, Lee SC, Oh HS, Kim SS, Koh HJ, Kwon OW. Incidence and clinical patterns of polypoidal choroidal vasculopathy in Korean patients. Jpn J Ophthalmol2008;52:57-62.
- Liu Y, Wen F, Huang S, Luo G, Yan H, Sun Z, et al. Subtype lesions of neovascular age-related macular degeneration in Chinese patients. Graefes Arch ClinExpOphthalmol2007; 245:1441-45.
- Sho K, Takahashi K, Yamada H, Wada M, Nagai Y, Otsuji T, et al. Polypoidal choroidal vasculopathy: incidence, demographic features, and clinical characteristics. Arch Ophthalmol2003; 121:1392-96.
- Maruko I, Iida T, Saito M, Nagayama D, Saito K. Clinical characteristics of exudative age-related macular degeneration in Japanese patients. Am J Ophthalmol2007;144:15-22.
- Lafaut BA, Leys AM, Snyers B, Rasquin F, De Laey JJ. Polypoidal choroidal vasculopathy in Caucasians. Graefes Arch ClinExpOphthalmol2000; 238:752-59.
- Yannuzzi LA, Wong DW, Sforzolini BS, Goldbaum M, Tang KC, Spaide RF, et al. Polypoidal choroidal vasculopathy and neovascularized agerelated macular degeneration. Arch Ophthalmol1999; 117:1503-10.
- Scassellati-Sforzolini B, Mariotti C, Bryan R, Yannuzzi LA, Giuliani M, Giovannini A. Polypoidal choroidal vasculopathy in Italy. Retina 2001; 21:121-25.
- Sho K, Takahashi K, Yamada H, Wada, Nagai Y, Otsuji T, et al. Polypoidal choroidal vasculopathy: Incidence, demographic features, and clinical characteristics. Ophthalmol. 2003;121:1392–96.
- Cheung C M, Li X, Mathur R, Lee S Y, Chan C M, Yeo I,et al. A prospective study of treatment patterns and 1-year outcome of asian age-related macular degeneration and polypoidal choroidal vasculopathy. PLoSONE2014, 9, e101057.
- Li Y, You Q S, Wei W B, Xu J, Chen C X, Wang Y X,et al. Polypoidal choroidal vasculopathy in adult Chinese: The Beijing Eye Study. Ophthalmology 2014;121:2290–91.
- Uyama M, Matsubara T, Fukushima I, Matsunaga H, Iwashita K, Nagai Y, et al. Idiopathic polypoidal choroidal vasculopathy in Japanese patients. Archives of ophthalmology 1999; 117, 1035–42.
- Spaide, R F, Yannuzzi L A, Slakter J S, Sorenson J &Orlach D A. Indocyanine green videoangiography of idiopathic polypoidal choroidal vasculopathy. Retina1995; 15:100–10.
- KohA, Lee WK, Chen LJ, Chen SJ, Hashad Y, Kim H,et al. EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina 2012; 32:1453-64.
- Chan WM, Lam DS, Lai TY, Liu DT, Li KK, Yao Y, et al. Photodynamic therapy with verteporfin for symptomatic polypoidal choroidal vasculopathy: one-year results of a prospective case series. Ophthalmology2004; 111:1576-84.
- Mauget-Faysse M, Quaranta-El Maftouhi M, De La Marnierre E, Leys A. Photodynamic therapy with verteporfin in the treatment of exudative idiopathic polypoidal choroidal vasculopathy. Eur J Ophthalmol2006;16:695-704.
- Spaide RF, Donsoff I, Lam DL, Yannuzzi LA, Jampol LM, Slakter J, et al. Treatment of polypoidal choroidal vasculopathy with photodynamic therapy. Retina2002; 22:529-35.
- Akaza E, Yuzawa M, Matsumoto Y, Kashiwakura S, Fujita K, Mori R. Role of photodynamic therapy in polypoidal choroidal vasculopathy. Jpn J Ophthalmol2007; 51:270-77.
- Silva RM, Figueira J, Cachulo ML, Duarte L, Faria de Abreu JR, Cunha-Vaz JG. Polypoidal choroidal vasculopathy and photodynamic therapy with verteporfin. Graefes Arch ClinExpOphthalmol2005; 243:973-79.
- Miki A, Honda S, Kojima H, Nishizaki M, Nagai T, Fujihara M, et al; Hyogo Macular Disease Study Group. Visual outcome of photodynamic therapy for typical neovascular age-related macular degeneration and polypoidal choroidal vasculopathy over 5 years of follow-up. Jpn J Ophthalmol2013; 57:301-07.
- Schmidt-Erfurth U, Michels S, Barbazetto I, Laqua H. Photodynamic effects on choroidal neovascularization and physiological choroid. Invest Ophthalmol Vis Sci2002; 43:830–41.
- Schmidt-Erfurth U, Schlötzer-Schrehard U, Cursiefen C, Michels S, Beckendorf A, Naumann GO. Influence of photodynamic therapy on expression of vascular endothelial growth factor (VEGF), VEGF receptor 3, and pigment epithelium-derived factor. Invest Ophthalmol Vis Sci2003; 44:4473–80.
- Potter MJ, Claudio CC, Szabo SM. A randomized trial of bevacizumab and reduced light dose photodynamic therapy in age-related macular degeneration: the VIA study. Br J Ophthalmol2010; 94:174–79.
- Yamashita A, Shiraga F, Shiragami C, Shirakata Y, Fujiwara A. Two-year results of reduced-fluence photodynamic therapy for polypoidal choroidal vasculopathy. Am J Ophthalmol2013;155:96-102.e1.
- Hikichi T, Higuchi M, Matsushita T, Kosaka S, Matsushita R, Takami K, et al. Results of 2 years of treatment with as-needed ranibizumab reinjection for polypoidal choroidal vasculopathy. Br J Ophthalmol2013; 97:617-21.
- Gomi F, Sawa M, Wakabayashi T, Sasamoto Y, Suzuki M, Tsujikawa M. Efficacy of intravitreal bevacizumab combined with photodynamic therapy for polypoidal choroidal vasculopathy. Am J Ophthalmol2010;150:48–54.
- Saito M, Iida T, Kano M, Itagaki K. Two-year results of combined intravitreal ranibizumab and photodynamic therapy for polypoidal choroidal vasculopathy. Graefes Arch ClinExpOphthalmol2013; 251:2099-10.
- Lai TY, Lee GK, Luk FO, Lam DS. Intravitreal ranibizumab with or without photodynamic therapy for the treatment of symptomatic polypoidal choroidal vasculopathy. Retina2011; 31:1581-88.
- \Wang W, He M, Zhang X. Combined intravitreal anti-VEGF and photodynamic therapy versusphotodynamic monotherapy for polypoidal choroidal vasculopathy: A systematic review and meta-analysis of comparative studies. PLoS ONE2014, 9, e110667.
- Akaza E, Yuzawa M, Mori R. Three-year follow-up results of photodynamic therapy for polypoidal choroidal vasculopathy. J. Ophthalmol. 2011;55:39–44.
- Honda S, Kurimoto Y, Kagotani Y, Yamamoto H, Takagi H, Uenishi M Hyogo. Macular Disease Study Group. Photodynamic therapy for typical age-related macular degeneration and polypoidal choroidal vasculopathy: A 30-month multicenter study in Hyogo, Japan. J. Ophthalmol. 2009;53:593–97.
- Hata M, Mandai M, Kojima H, Kameda T, Miyamoto N, Kurimoto Y. Five-year visual outcomes of typical age-related macular degeneration and/or polypoidal choroidal vasculopathy patients who received photodynamic therapy (PDT) as initial treatment in comparison with patients prior to the PDT era. Nippon Ganka Gakkai Zasshi2012;116: 937–45.
- Jeon S, Lee W K, Kim K S. Adjusted retreatment of polypoidal choroidal vasculopathy after combination therapy: Results at 3 years. Retina 2013;33:1193–00.
- Kang H M, Kim YM, Koh H J. Five-year follow-up results of photodynamic therapy for polypoidal choroidal vasculopathy. J. Ophthalmol. 2013;155:438–47.
- Leal S, Silva R,Figueira J, Cachulo M L, Pires I, de Abreu J R, et al. Photodynamic therapy with verteporfin in polypoidal choroidal vasculopathy: Results after 3 years of follow-up. Retina2010;30:1197–05.
- Saito M, Iida T, Kano M, Itagaki K. Five-year results of photodynamic therapy with and without supplementary antivascular endothelial growth factor treatment for polypoidal choroidal vasculopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2014;252:227–35.
- Kang H M, Koh HJ, Lee CS, LeeS C. Combined photodynamic therapy with intravitreal bevacizumab injections for polypoidal choroidal vasculopathy: Long-term visual outcome. J. Ophthalmol. 2014;157:598–06.
- Sato T, Kishi S, Matsumoto H, Mukai R. Comparisons of outcomes with different intervals between adjunctive ranibizumab and photodynamic therapy for polypoidal choroidal vasculopathy. Am J Ophthalmol. 2013 ; 156:95-05.
- Ricci F, Calabrese A, Regine F, Missiroli F, Ciardella AP.Combined reduced fluence photodynamic therapy and intravitrealranibizumab for polypoidal choroidal vasculopathy. Retina 2012; 32:1280–88.
- Gomi F, Oshima Y, Mori R, Kano M, Saito M, Yamashita A,et al. Initial versus delayed photodynamic therapy in combination with ranibizumab for treatment of polypoidal choroidal vasculopathy: The Fujisan Study.Retina. 2015; 35:1569-76.
- Hata M, Tsujikawa A, Miyake M, Yamashiro K, Ooto S, Oishi A,et al. Two-year visual outcome of polypoidal choroidal vasculopathy treated with photodynamic therapy combined with intravitreal injections of ranibizumab. Graefes Arch ClinExpOphthalmol.2015; 253:189-97.
- Sakurai M, Baba T, Kitahashi M, Yokouchi H, Kubota-Taniai M, Bikbova G, et al. One year results of intravitreal ranibizumab combined with reduced-fluence photodynamic therapy for polypoidal choroidal vasculopathy. ClinOphthalmol 2014; 8:235-41.
- Lee YA, Yang CH, Yang CM, Ho TC, Lin CP, Huang JS, et al. Photodynamic therapy with or without intravitreal bevacizumab for polypoidal choroidal vasculopathy: two years of follow-up. Am J Ophthalmol. 2012;154:872–80.
Leave a Comment