
Dr. Bidisha Mahapatra, B20295, Dr. Sharmistha Behera, Dr. Pramod Kumar Sharma, Dr. Soni S.
Abstract
Aim: To evaluate the demographics and clinical features of eyelid masses in a tertiary eye hospital over 5-year period.Materials and Methods:Retrospective review performed for patients admitted with eyelid tumors from 2012 to 2016.Data collected and analyzed on the demographic features, location of the tumor, treatment given and pathologic findings.Results:Of 96 patients evaluated,76 were benign and 20were malignant.Most common benign tumors included melanocytic nevi (37.5%),papilloma (20.8%),cysts(12.5%),hair follicle tumors(4.16%)and pyogenic granuloma(4.16%).The most frequent malignant tumors included basal cell carcinoma (10.41%),sebaceous gland carcinoma (6.25%),squamous cell carcinoma (2.08%) and metastatic lesions(2.08%).The most common site for malignancy was the upper lid followed by the lower lid except for BCC which most commonly involved lower lid.Conclusion:Melanocytic nevus is most common benign and BCC is the most common malignant lesion in the eyelids.
Introduction :
Eyelid growth is a common clinical condition presented to ophthalmologists1. The eyelid is
rich in glandular tissue which includes sweat glands of the eyelid skin, lacrimal gland of Krause and Wolfring, the apocrine gland of Moll, meibomian and the glands of Zeiss [2]. Pathologic conditions affecting the eyelid may be inflammatory or neoplastic. It has been reported that 90% of skin cancers occurs in head and neck region and 10% of them are located at eyelid level2. Benign epithelial lesions, cystic lesions, and benign melanocytic lesions of eyelid are very common3. Among the benign lesions, squamous cell papilloma, seborrheic keratosis, melanocytic nevus are common. Most common malignant tumors of eyelid are basal cell carcinoma, squamous cell carcinoma and sebaceous carcinoma.Other less common malignant tumours include merkel cell carcinoma, lymphoma and secondary metastatic carcinoma4. Inflammatory and infectious lesions simulating neoplasm are also common. Basal cell carcinoma is the most common malignancy of eyelid. Eyelid tumors are rarely lethal, but late diagnosis of the tumors requires more invasive surgery and consequently will have adverse esthetic effects5. The incidence of eyelid skin tumors is mostly a result of environmental factors including sunlight and ultra violet exposure and genetic factors including skin pigmentation. Therefore, the prevalence of these types of tumor shows a geographical variation. The eyelids are composed of four layers: skin and subcutaneous tissue including its adnexa, striated muscle, tarsus with the meibomian glands, and the palpebral conjunctiva. Benign and malignant tumors can arise from each of the eyelid layers. Most eyelid tumors are of cutaneous origin, mostly epidermal, which can be divided into epithelial and melanocytic tumors. Following is the classification of eyelid tumors according to their origin. (??Copyrighted imag)
Methods
This retrospective case series was based on the review of the hospital records of the patients who had undergone biopsy of their lid lesions from january 2012 to december 2016. All benign and malignant tumors were managed by appropriate methods of surgical excision of the lesion. Tumors were excised by the ophthalmologist and the specimens were collected
by researcher for histopathology examination. Data collected and analyzed on the demographic features, location of the tumor, treatment given and pathologic findings.
Results
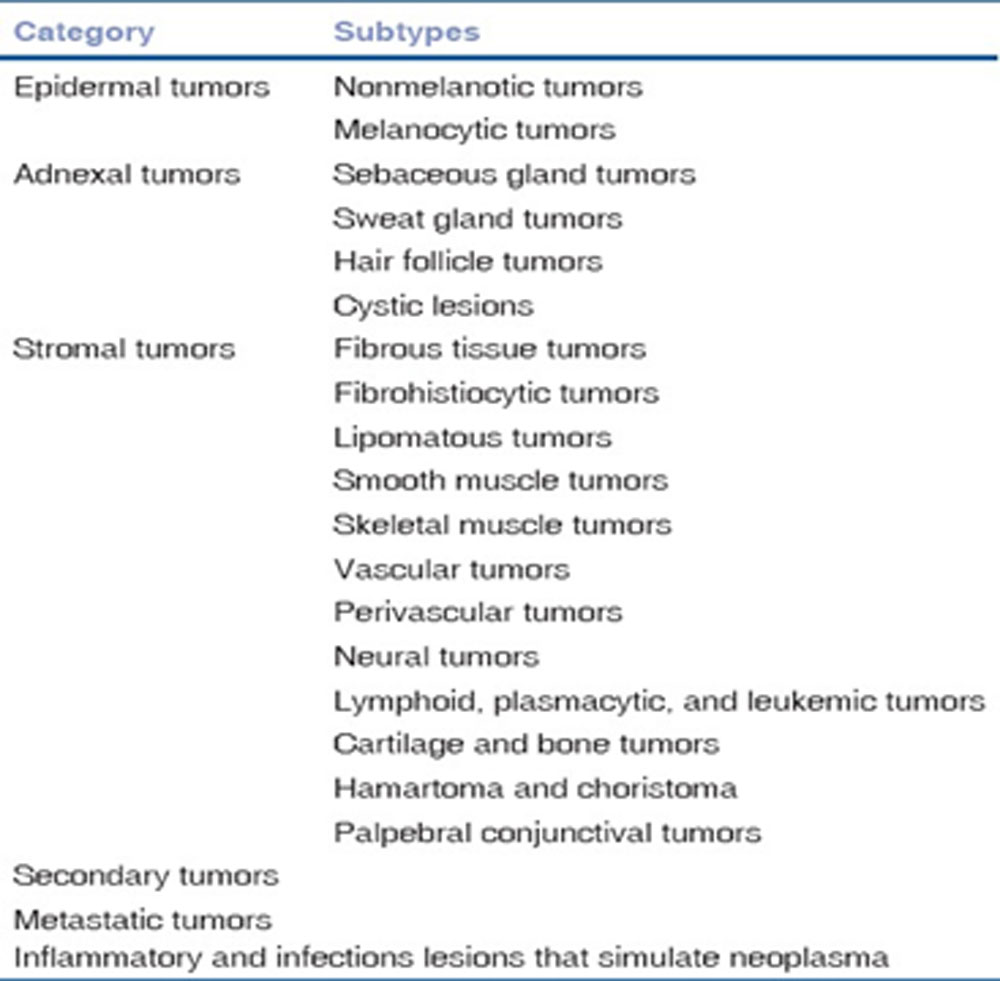
Out of 96 cases, 76(79.16 %) of the eyelid lesions were benign tumors and 20(20.8%) were malignant. The age of the patients ranged from 2 to 80 years.
Most benign tumors were diagnosed in patients under the age of 60 years. There were females 56 (58.33%) and 40 males (41.6 %), benign tumors were more prevalent among females (n=45, 59.2%) than in males (n=31, 40.78%),overall male to female ratio was 5:7. Benign tumors involved the upper eyelid (n=50, 65.7%) more commonly than lower lid (n=26, 34.2%).Involvement of the upper eyelid was more often noted in some pathologic lesions like papilloma,meibomian cysts,hair follicle tumors, epidermoid and dermoid cysts. Melanocytic nevi were equally distributed in both eyelids.
Most common benign tumors included melanocytic nevi (37.5%),papilloma (20.8%),cysts(12.5%),hair follicle tumors(4.16%)and pyogenic granuloma(4.16%).
A preference for upper lid (64.58%), but no gender preference was seen. Nevi represented 47.36% of all benign lesions , more commonly found in the 3rd to 4th decade and in the lower lid. . Papilloma accounted for 26.31% of cases, demonstrated a greater involvement of upper eyelid, but no gender or eye preference was seen. Mostly, cases were seen in the third and fourth decade. Meibomian cyst(chalazion),epidermal cysts and dermoid cysts represented 15.78% (24cases) of all benign lesions. These lesions were mostly seen on the upper eyelid,and dermoid cysts were seen mostly in the young children. No gender predilection was noted.
In the present study,20(20.8%) cases were diagnosed to be malignant eyelid tumors. The most frequent malignant tumors included basal cell carcinoma (50%),sebaceous gland carcinoma (30%),squamous cell carcinoma (20%) and metastatic lesions(20%)
The mean age of the patients under the malignant category was 57.9years.There was no gender predilection. Regarding the malignant group, the lower lid was involved more in basal cell carcinomas while sebaceous cell carcinomas and other malignant lesions mostly involved upper eyelids. The most common location of malignant tumors was upper lid (55%).
9 out of 10 cases of BCC being on the lower lid,the lower lid was also the most common location for BCC. The most common presenting complaint was mass with ulceration across all histological types of BCC. 4 out of 6 cases of sebaceous cell carcinomas came with complains of recurrent chalazion after insicion and curettage. Other associated complains included redness,pain,watering from the involved eye.
68 benign lesions underwent excision biopsy,14 lid tumors including benign and malignant masses involving less than 1/3rd lid margin underwent wide excision and lid reconstruction by Tenzel’s semicircular flap,6 meibomian cyst underwent incision and curettage,6 malignant growths underwent wide excision with Mustarde’s cheek rotation flap and 1 tumor was resected and lid reconstructed by Cutler-Beard procedure.
| Type of lesions | No of cases | % |
| benign
1. melanocytic nevi |
36 |
37.5 |
| 2. papilloma | 20 | 20.8 |
| 3.cysts | 12 | 12.5 |
| 4.hair follicle tumors | 4 | 4.16 |
| 5.pyogenic granuloma | 4 | 4.16 |
| Malignant
6.basal cell ca |
10 |
10.41 |
| 7.sebaceous gland ca | 6 | 6.25 |
| 8.squamous cell ca | 2 | 2.08 |
| 9.metastatic ca | 2 | 2.08 |
Table1:Distribution of various types of eyelid masses
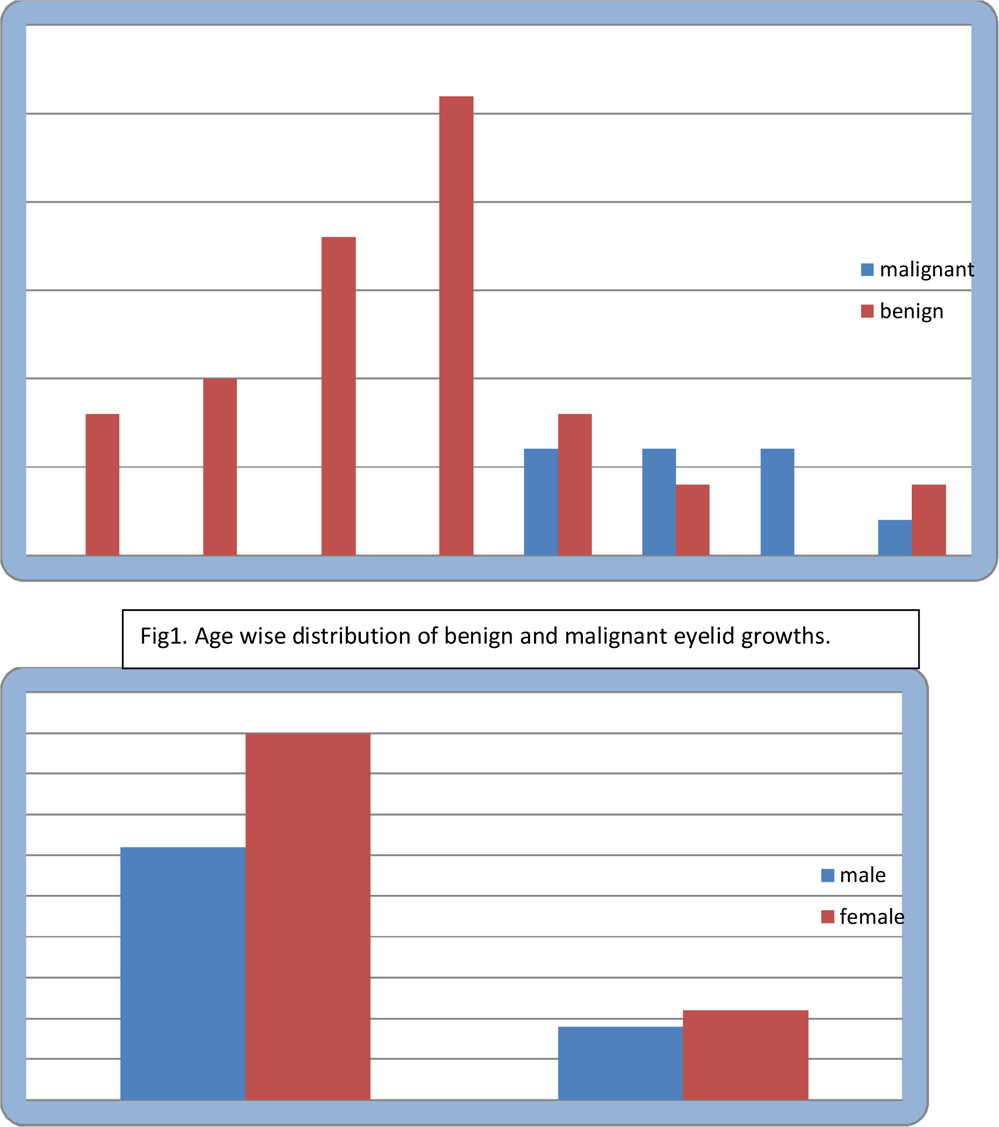
Fig2: sex wise distribution of benign and malignant eyelid growths
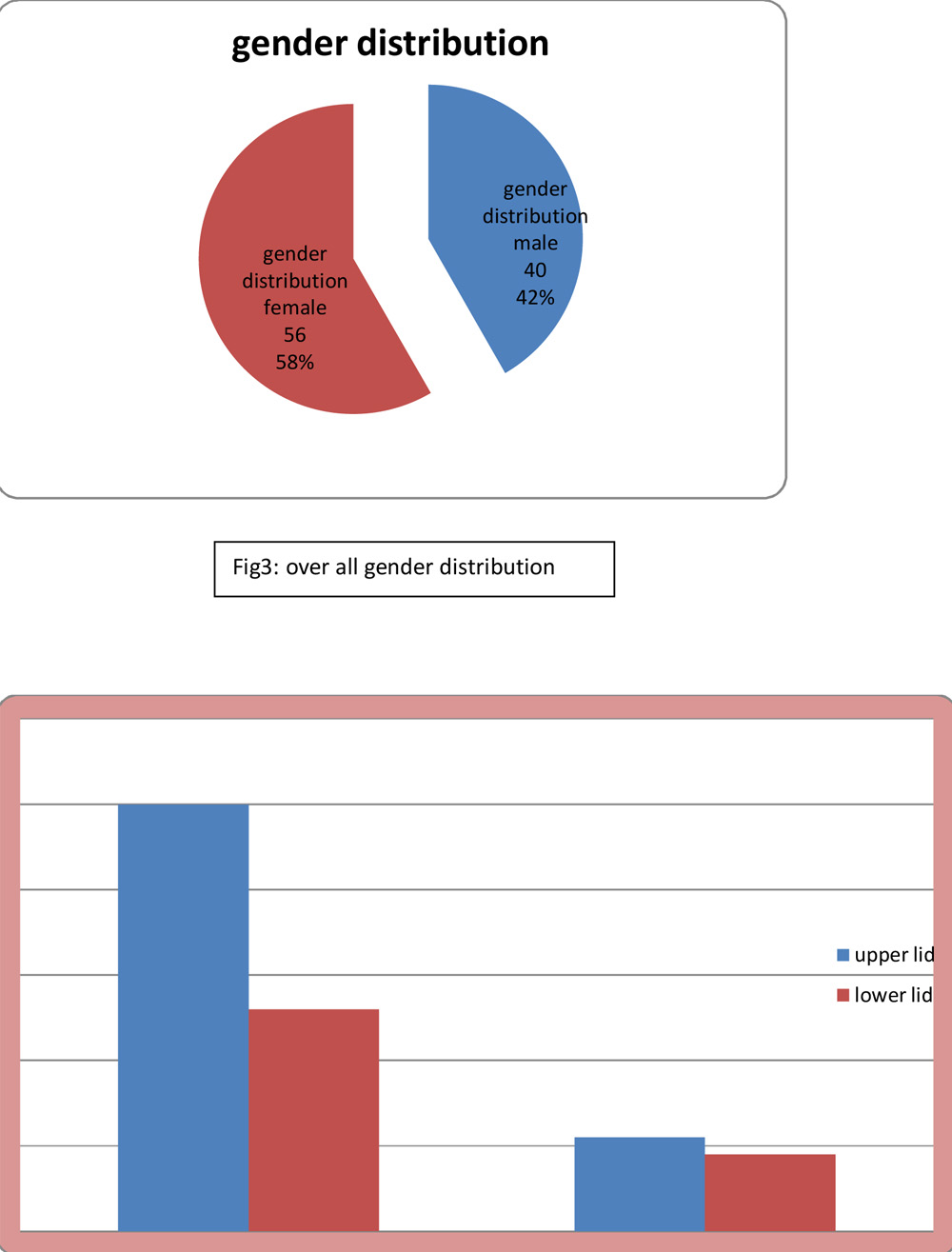
Fig4: location distribution of benign and malignant lesions
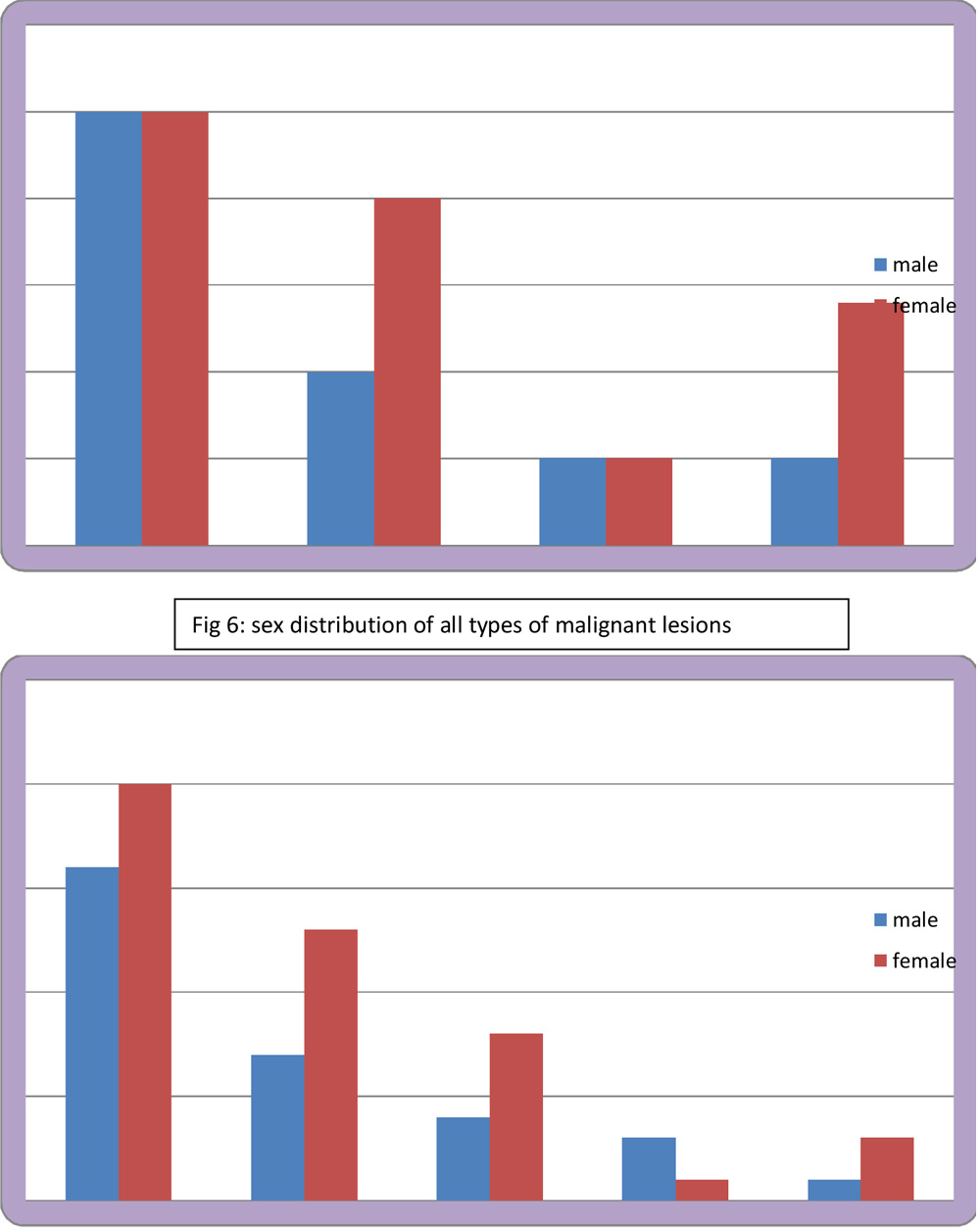
Fig 7: sex distribution of all types of benign lesions
| Types of procedure done | No of cases |
| 1.Excision and biopsy | 68 |
| 2.Wide excision with lid reconstruction by Tenzels semicircular flap | 14 |
| 3.Incision and curettage | 6 |
| 4.wide excision with Mustard’s cheek rotation flap | 4 |
| 5.Cutler-Beard procedure | 2 |
Table 2: various treatment modalities for the different lesions
Discussion
In our study, 76 cases (79.16%) were benign eyelid tumours, nearly similar to that reported by Xu et al from Beijing (86.2% benign involving 2638 patients)6, Deprez et al (84% benign from study on 5504 cases)7, Paul S et al (855 cases, 75.9% were benign)8, and Obata H et al (73% of 131 cases)9. However studies by Abdi et al1 from India and Bagheri A et al10 from Tehran have reported only 58.9% (n= 207 cases) and 45.5% (n=182 cases)respectively, showing comparatively lesser incidence of benign lesions.
In our study most common benign lid tumor was nevus(47.36%),followed by papilloma(26.31%) and cysts.3 separate studies from China, Southern Taiwan and South Korea the most frequent benign tumors were, in descending order, nevus, papilloma, and cyst11,12,6.The most prevalent benign masses in the studies by Kersten et al.13 and Ni14 were papilloma. In the study by Hsu and Lin15 the most frequent type of benign tumors in patients was dermoid cysts. Certain demographic, geographic and climate conditions can also influence the frequency of different type of eyelid masses.
In the our study,65.78% benign lesions were located on the upper lid. In a similar study from Thailand, 51% of benign tumors originated from the upper eyelid.16 Similarly, a study from Southern Taiwan reported 46% of benign cases were located in the upper eyelid.11 In contrast, a Chinese study, reported the lower eyelid was involved slightly more frequently than upper eyelid6.
In our study,most common malignant eyelid lesion was BCC(50%) followed by sebaceous cell carcinoma(30%).Worldwide, BCC is the most common eyelid malignant tumour (table 2)6,7,11,16,17,18
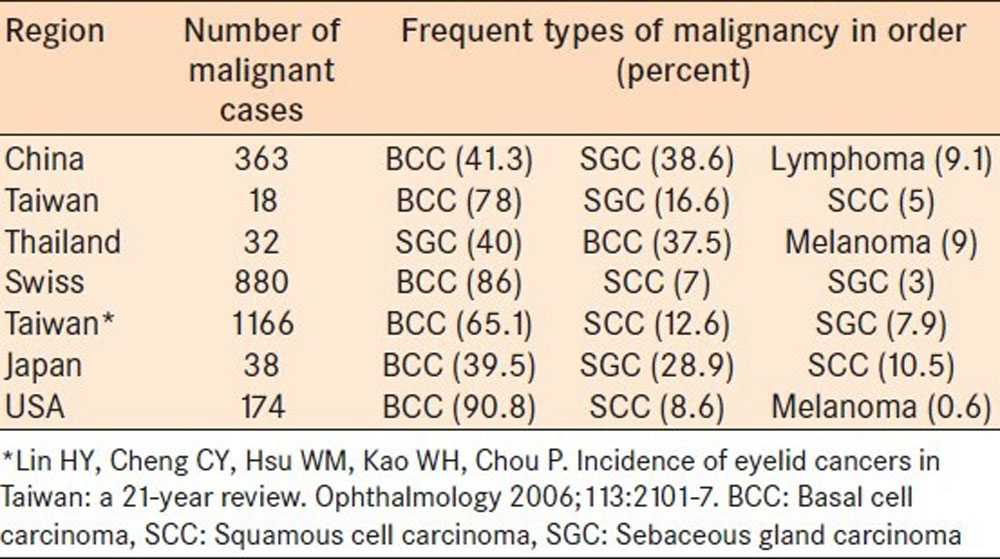
However,asian countries like Thailand, India, Japan, China studies provide evidence, in favour of a higher proportion (30-40%) of occurrence of SGC. Some reports from central India(Sihota et al (30%), Jahagirdar S S et al (44.5%), Kale SM et al (48.2%)19,20,21show a relatively lower incidence of BCC.
In our study,mean age of presentation of malignant lesions was 57.9years,while that of benign lesions was 40.6years. Results were consistent with other similar studies. Wang et al reported 127 cases of malignant eyelid tumor with a mean age of presentation of 62.6 year22. Rathod et al reported 100 cases of eyelid tumors with mean age of malignant eyelid tumors presentation was 58.59±11.271 and benign tumors was 37.02±16.84723.
In our study,female preponderance was slightly higher compared to males(7:5). In both benign(59.2%) and malignant(55%) groups,females were more affected. In the malignant group, all types except sebaceous cell carcinomas showed no sex predilection. In sebaceous cell carcinomas,female:male ratio was 2:1. Wang et al. reported that though the incidence of lid malignancies was more in women than men (54.3% vs. 45.7%), there was a slight predominance of BCC in men (43 males, 36 females). Women outnumbered men in SGC (21 females, 9 males)22.
Also,the occurrence of SGC is more in upper eyelid than lower eyelid(5 out of 6cases). This preference is linked to relatively greater number of meibomian glands located in the upper lid versus the lower lid. Various studies have reported greater number of SGC cases in upper eye lid21,24.
In general, 20% of BCC occur in the periocular area of which half of the cases present in the lower eyelid, one-third in the medial canthus, 15% in the upper eyelid and 5% in the lateral canthus.25,26 Similarly, in the present study, most (60%) cases of BCC were in the lower eyelid.
Conclusion
Eyelid malignancies are completely treatable if detected early. Early diagnosis of eyelid growth is thus of extreme importance to avoid high morbidity and mortality. The incidence of eyelid tumors is increasing. Eyelid tumors thus form an important part of ophthalmology practice, and are by far the most common neoplasms encountered in ophthalmic practice.
- Abdi UN, Tyagi V, Maheshwari V, Gogi R, Tyagi SP. Tumors of eyelid: A clinicopathologic study. J Indian Med Assoc 1996;94:405-9, 416, 418 .
- Myers M, Gurwood AS. Periocular malignancies and primary eye care. Optometry. 2001; 72(11): 705–712.
- Pe’er J . Pathology of eyelid tumors. Indian J Ophthalmol. 2016; 64(3): 177–190
- . Klintworth GK, Cummings TJ. The eye and ocular adnexia. In: Mills SE, Carter D, Greenson JK, Reuter VE, Stoler MH, editors. Sternberg’s diagnostic surgical pathology, Vol. I. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2009, p965.
- Hilovsky JP. Lid lesions suspected of malignancy. J Am Optom Assoc. 1995;66:510–5. [PubMed]
- Xu XL, Li B, Sun XL, Li LQ, Ren RJ, Gao F, et al. Eyelid neoplasms in the Beijing Tongren Eye Centre between 1997 and 2006. Ophthalmic Surg Lasers Imaging 2008; 39: 367-72.
- Deprez M, Uffer S. Clinicopathological features of eyelid skin tumors. A retrospective study of 5504 cases and review ofliterature. Am J Dermatopathol 2009; 31: 256-62.
- Paul S, Dat T. Vo, Rona Z. Silkis et al: Malignant and Benign Eyelid Lesions in San Franscisco: Study of a Diverse Urban Population:American Journal of Clinical Medicine- Winter 2011, Volume Eight, Number One: page 40-46
- Obata H, Aoki Y, Kubota S, Kanai N, Tsuru T Incidence of benign and malignant lesions of eyelid and conjunctival tumors. Nihon Ganka Gakkai Zasshi. 2005 Sep; 109 (9): 573-9.
- Bagheri A, Tavakoli M, Kanaani A, Zavareh R B, Esfandiari H, Aletaha M, Salour H. Eyelid Masses: A 10-year Survey from a Tertiary Eye Hospital in Tehran: Middle East African Journal of Ophthalmology Jul 9, 2013: vol 20, issue 3: page187-192.
- Chang CH, Chang SM, Lai YH, Huang J, Su MY, Wang HZ, et al. Eyelid tumors in southern Taiwan: A 5-year survey from a medical university. Kaohsiung J Med Sci. 2003;19:549–54. [PubMed]
- Chi MJ, Baek SH. Clinical analysis of benign eyelid and conjunctival tumors. Ophthalmologica. 2006;220:43–51. [PubMed])
- Kersten RC, Ewing-Chow D, Kulwin DR, Gallon M. Accuracy of clinical diagnosis of cutaneous eyelid lesions. Ophthalmology. 1997;104:479–84. [PubMed]
- Ni Z. Histopathological classification of 3,510 cases with eyelid tumor. Zhonghua Yan Ke Za Zhi. 1996;32:435–7. [PubMed]
- Hsu HC, Lin HF. Eyelid tumors in children: A clinicopathologic study of a 10-year review in southern Taiwan. Ophthalmologica. 2004;218:274–7. [PubMed]
- Pornpanich K, Chindasub P. Eyelid tumors in Siriraj Hospital from 2000-2004. J Med Assoc Thai. 2005;88:S11–4. [PubMed]
- Cook BE, Jr, Bartley GB. Epidemiologic characteristics and clinical course of patients with malignant eyelid tumors in an incidence cohort in Olmsted County, Minnesota. Ophthalmology. 1999;106:746–50. [PubMed]
- . Takamura H, Yamashita H. Clinicopathological analysis of malignant eyelid tumor cases at Yamagata university hospital: Statistical comparison of tumor incidence in Japan and in other countries. Jpn J Ophthalmol. 2005;49:349–54. [PubMed]
- Sihota RK, Tandon SM, Betharia SM, Arora R. Malignant eyelid tumors in an Indian population. Arch Ophthalmol 1996; 114: 108-9.
- . Sameer S Jahagirdar, Tushar P Thakre, Satish M Kale, Hemant Kulkarni, Manju Mamtani A clinicopathological study of eyelid malignancies from central India Year: 2007 | Volume: 55 | Issue: 2 | Page: 109-112.
- Satish M. Kale, Surendra B. Patil, Nishant Khare, Mahantesh Math, Arvind Jain, and Sumeet Jaiswal Clinicopathological analysis of eyelid malignancies – A review of 85 cases Indian J Plast Surg. 2012 Jan-Apr; 45 (1): 22–28. doi: 10.4103/0970-0358.96572
- Wang JK, Liao SL, Jou JR, Lai PC, Kao SC, Hou PK, Chen MS. Malignant eyelid tumors in Taiwan. Eye (Lond). 2003; 17(2):216-220.
- Jahagirdar SS, Thakre TP, Kale SM, Kulkarni H, Mamtani M. A clinicopathological study of eyelid malignancies from central India. Indian J Ophthalmol. 2007; 55(2):109-112.
- Suresh Saquil, Raman Malhotra.The importance of considering Sebaceous gland carcinoma in presumed chalazia in South Asian patients.Br J Gen Pract.Feb 2013; 63 (607): 74.
- Allali J, D’Hermies F, Renard G. Basal cell carcinomas of the eyelids. Ophthalmologica. 2005;219:57–71. [PubMed]
- Perlman GS, Hornblass A. Basal cell carcinoma of the eyelids: A review of patients treated by surgical excision. Ophthalmic Surg. 1976;7:23–7. [PubMed]
Leave a Comment