
Dr. Naveen Keshav S, S19230, Dr. Rathinam
Sivakumar R
INTRODUCTION
Vogt-Koyanagi-Harada (VKH) disease is a chronic bilateral granulomatous panuveitis and exudative retinal detachment associated with poliosis, vitiligo, alopecia, auditory signs and CNS involvement1. The exact cause is unknown but suggested to be due to T helper cell (Th1 and Th17) mediated immune response to tyrosinase family protein antigens associated with melanocytes.2,3
The aim of therapy in VKH is to suppress the initial intraocular inflammation in acute posterior uveitis stage with early and aggressive use of systemic steroids, thereby preventing progression to chronic stage and reducing extra-ocular manifestations. 1,4,5 High doses (1 mg/kg/day prednisone) are required to bring the inflammation under control 6. The intraocular inflammation can result in recurrent anterior granulomatous uveitis with sunset glow fundus when not treated completely.
Systemic corticosteroid is the initial therapy for acute VKH and immunomodulators for chronic or recurrent VKH. 7 Observational studies on immunomodulators like azathioprine, methotrexate, mycophenolate mofetil, cyclosporine A and cyclophosphamide have been shown to be beneficial in treatment of VKH.
Cyclophosphamide, an alkylating agent was first introduced in 1952 for non-infectious uveitis of unknown etiology10. It has been studied that cyclophosphamide was an effective agent in treating recalcitrant cases of non-infectious uveitis. This study was undertaken to evaluate the role of cyclophosphamide (CP) in refractory cases of Vogt Koyanagi Harada disease (VKH)
MATERIALS AND METHODS
Design:-Retrospective observational case series
The study includes refractory cases of VKH who were started on cyclophosphamide. Of 199 patients of VKH who visited the uvea clinic in a tertiary eye care centre in South India over a period of 1 year, eight patients were started on cyclophosphamide therapy. The diagnosis of VKH was based on the Revised International Diagnostic Criteria with all patients atleast fulfilling the criteria for ‘probable’ VKH disease11
The medical records of all patients were reviewed. Demographic data included age, gender and laterality. Duration of VKH and the immunomodulators previously used were recorded. The initial presentation of VKH whether anterior uveitis or exudative retinal detachment was noted. Visual acuity at the initial visit, at the initiation of cyclophosphamide therapy, and after corticosteroid sparing control of inflammation was documented. Patient was monitored for leucocyte count, urine deposits, renal and liver function tests, erythrocyte sedimentation rate at the start of treatment and during subsequent follow-up.
Ocular examination of patient includes anterior chamber cells and flare according to SUN (Standardised Uveitis Nomenclature) guidelines. Lens status, posterior synechiae, vitritis, sunset glow fundus, chorioretinal scar and limbal depigmentation were recorded. Ocular complications like cataract, glaucoma, choroidal neovascular membrane, subretinal fibrosis, ocular hypertension were documented. Systemic side effects suggestive of hemorrhagic cystitis and urinary tract infections following cyclophosphamide therapy were recorded.
Indication for starting cyclophosphamide therapy:-
- Treatment failure to other immunosuppressant
- Steroid intolerance
- Intolerance to previous immunosuppressant
Recurrence of inflammation in the form of anterior uveitis, exudative retinal detachment, vitritis, optic disc oedema or depigmentation of the retinal pigment epithelium was recorded during follow-up. Clinical end-point of treatment was control of inflammation and improved visual acuity.
Statistical analysis:-The descriptive variables were given with mean (SD). The categorical variables were given with frequency. P value <0.05 is statistically significant. All statistical analysis were done in statistical software STATA 11.1 (Texas, USA)
RESULTS
Eight patients with VKH were included in the study. Mean (SD) age of presentation was 43.37(±10.56) years. 75% were females. Median duration of uveitis was 9 years. The initial presentation of VKH in 25% was anterior uveitis and 75% it was exudative retinal detachment. The initial line of management was on corticosteroid followed by immunomodulator before starting cyclophosphamide. These patients were initiated on cyclophosphamide due to failure to previous immunomodulator to control of inflammation, steroid intolerance, or intolerance to previous immunomodulator (Table1). Before starting cyclophosphamide 2 patients had azathioprine followed by mycophenolate mofetil (MMF). 1 patient had azathioprine followed by methotrexate, 2 were only on MMF and 3 only on methotrexate.
Posterior synechiae was observed in 68.5 % eyes. Sunset glow fundus was noted in 62.5 % eyes. Chorioretinal scar in 2 eyes and optic disc edema in 2 eyes were observed.
Table-2 Ocular complication
Table-1. Indication for Cyclophosphamide therapy
| Indication | N | % |
| Treatment failure to previous immunomodulator | 6 | 75 |
| teroid intolerance | 1 | 12.5 |
| Intolerance to previous immunomodulator | 1 | 12.5 |
| Total | 8 | 100 |
| Ocular complications | n | % |
| Cataract | 4 | 25.0 |
| Glaucoma | 2 | 12.5 |
| OHT | 2 | 12.5 |
| CNVM | 3 | 18.7 |
Ocular complications of these patients are listed in Table-2. One patient developed urinary tract infection during treatment. Urine deposits showed RBC cells in 37.5% of the patients but returned to normal on subsequent follow-up.
| Visual Acuity | Median
(Snellen’s equivalent) |
Min – Max | P-value W |
| Initial | 0.60(6/24) | 0.18 – 2.60 | 0.017 |
| Final | 0.39(~6/18) | 0.0 – 2.60 |
Five of the eight cases had 1 episode of recurrence. 2 episodes of recurrence occurred in one patient Recurrence of inflammation occurred in the form of anterior uveitis in all these cases. Oral steroid was stopped in one patient due to uncontrolled glaucoma following which recurrence occurred in 1 of these cases.
Visual acuity improvement was statistically significant (p=0.017) with cyclophosphamide. All cases had control of inflammation.
Table- 3 Analysis of visual outcome
Initial VA Final VA
DISCUSSION
Eight patients of VKH refractory to corticosteroid and antimetabolite therapy showed improvement in vision that was statistically significant (p=0.017) on cyclophophamide therapy. Moorthy et al reported use of single intravenous infusion of cyclophosphamide in 22% of cases. In our study only oral 100mg cyclophosphamide was given.
Recurrence in the form of anterior uveitis was observed in patients during follow-up. Fang et al (2008) showed that patients with recurrent VKH disease displayed a more intensive inflammation in the anterior segment and long-lasting disturbed blood aqueous barrier breakdown than those with initial-onset VKH disease13. This suggests that more aggressive treatment is needed for these patients.
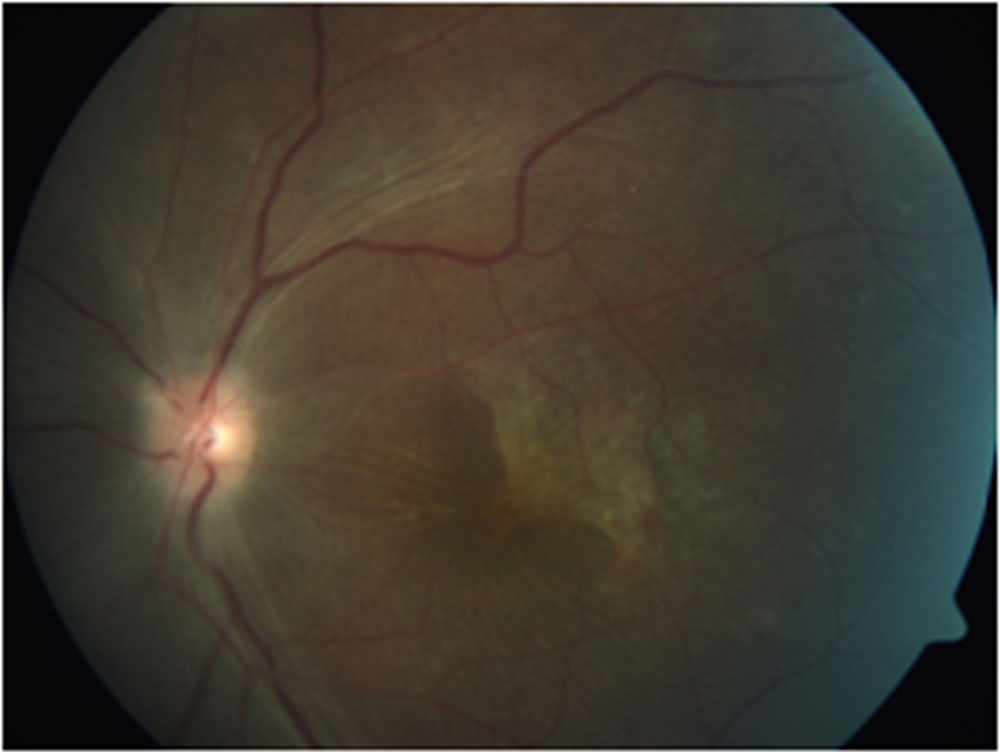
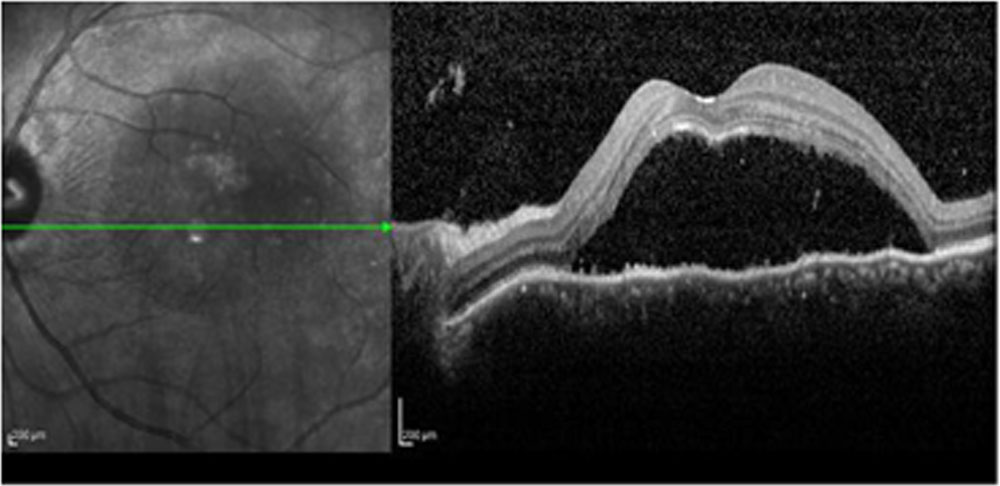
Figure-2 – Fundus photograph of a 38 year old female showing bilateral exudative retinal detachment with optic disc edema
According to Pujari et al cyclophosphamide was successful in achieving complete control of inflammation in 49.1% and 76.3% by 6 months and 12 months respectively in scleritis, uveitis and ocular pemphigoid. Corticosteroid-sparing success (sustained control of inflammation while tapering prednisone to 10 mg or less) was gained by 30.0% and 61.2% over 6 and 12 months respectively.
One patient developed urinary tract infection and 37.5 % showed RBC cells in urine deposits when compared to pujari et al where the most common side effects were leukopenia (18.1%) and cystitis/hematuria (7.7%). But these side effects were transient and lab values returned to normal on subsequent follow- up. The risk of side effects is substantially greater than with alternative agents, and requires very careful monitoring, and prophylaxis against opportunistic infections.
Figure-2 Figure-3
CONCLUSION
The result suggests that cyclophosphamide is an effective treatment modality in controlling inflammation and improving visual acuity in refractory cases of VKH. Thus cyclophosphamide should be considered when there is a high risk of vision loss or when other treatment modalities have failed to succeed.
REFERENCES
-
- Moorthy RS, Inomata H & Rao NA (1995):Vogt–Koyanagi–Harada syndrome. Surv Ophthalmol 39: 265–292
- Yamaki K, Gocho K, Hayakawa K et al.(2000a): Tyrosinase family proteins are antigens specific to Vogt–Koyanagi–Harada disease. J Immunol 165: 7323–7329
- Abu El-Asrar AM, Struyf S, Kangave D et al. (2011): Cytokine profiles in aqueous humor of patients with different clinical entities of endogenous uveitis. Clin Immunol 139: 177–184.
- Abu El-Asrar AM, Al-Kharashi AS, Aldibhi H et al. (2008): Vogt-Koyanagi-Harada disease in children. Eye (Lond) 22: 1124–1131.
- Ohno S, Minakawa R & Matsuda H (1988):Clinical studies of Vogt–Koyanagi–Harada disease. Jpn J Ophthalmol 32: 334–343.
- Sasamoto Y, Ohno S, Matsuda H. Studies on corticosteroid therapy in Vogt Koyanagi Harada disease. Ophthalmologica 1990;201(3):162–167
- .Read RW, Rao NA, Cunningham ET. Vogt Koyanaga Harada disease.Curr Opin Ophthalmol. 2000;11(6):437–442.
- Cuchacovich M, Solanes F, Diaz G, et al. Comparison of the clinical efficacy of two different immunosuppressive regimens in patients with chronic vogt-koyanagi-harada disease. Ocul Immunol Inflamm 2010;18(3):200-207
- .Abu El-Asrar AM, Hemachandran S, Al-Mezaine HS, Kangave D, Al-Muammar AM.The outcomes of mycophenolate mofetil therapy combined with systemic corticosteroids in acute uveitis associated with vogt-koyanagi-harada disease. Acta Ophthalmol 2012;90(8):e603-608.
- Roda Perez E. Nitrogen mustard therapy of uveitis of unknown etiology [undetermined language] Rev Clin Esp. 1952;44:173–80
- Read RW, Holland GN, Rao NA, et al. Revised diagnostic criteria for Vogt-Koyanagi-Harada disease: report of an international committee on nomenclature.Am JOphthalmol 2001;131(5):647-52
- Murthy SI, Moroker MR, Sangwan VS, et al. The spectrum of Vogt-Koyanagi-Harada disease in South India. Int Ophthalmol. 2007;27: 131-136.
- Fang W, Zhou H, Yang P, Huang X, WangL & Kijlstra A (2008): Longitudinal quantification of aqueous flare and cells in Vogt-Koyanagi-Harada disease. Br J Ophthalmol 92: 182–185
- Pujari SS, Kempen JH, Newcomb CW, Gangaputra S, Daniel E, Suhler EB, et al. Cyclophosphamide for ocular inflammatory diseases.Ophthalmology. 2010 Feb;117(2):356
Leave a Comment